Page 14 of 32
PA25.5 | Occupational & Interstitial Lung Disease — SDL Guide (Part 2)
Silicosis
Silicosis: Exposure, Pathogenesis and Morphology
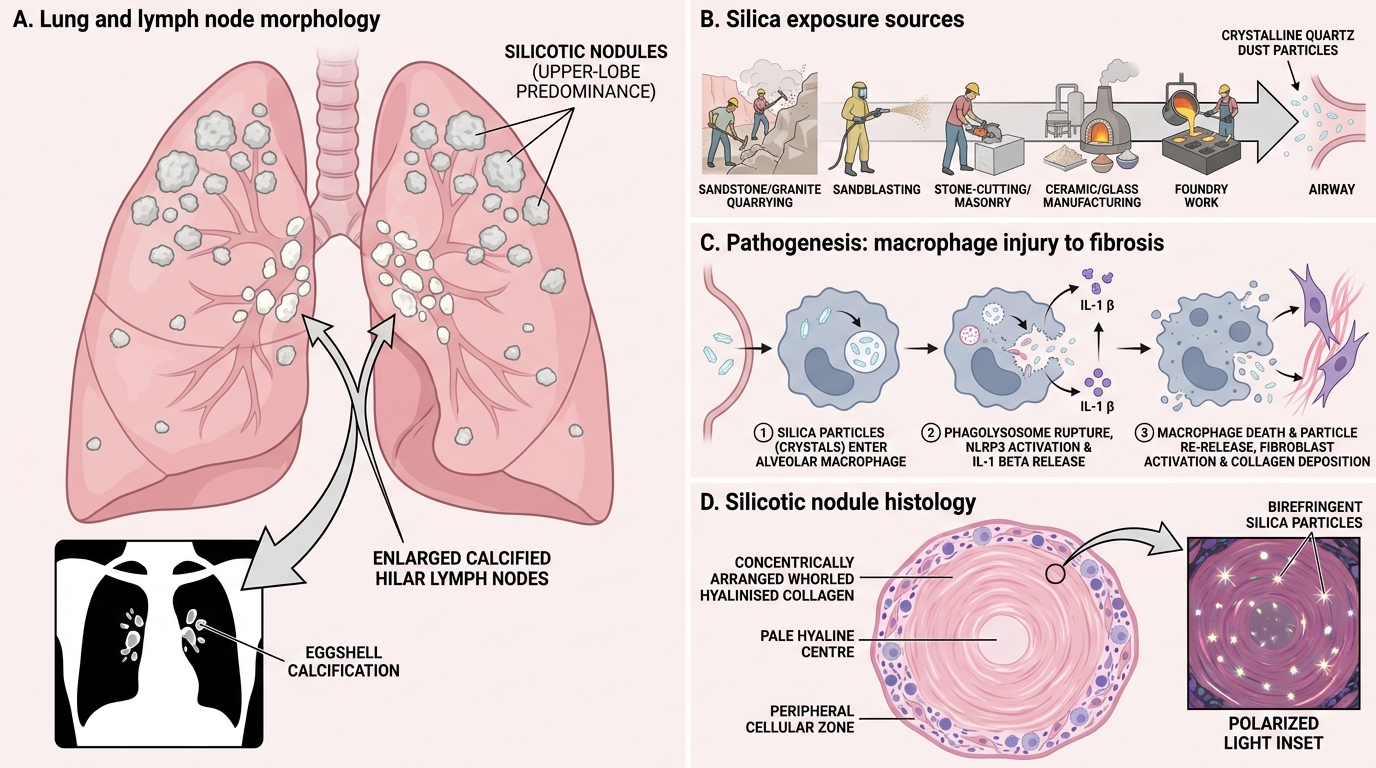
Silica (silicon dioxide, SiO₂, crystalline form = quartz) is the most abundant mineral in the earth's crust and the most common cause of occupational lung disease worldwide.
High-risk occupations (India-relevant):
• Sandstone/granite quarrying (Rajasthan, Uttarakhand)
• Sandblasting (construction, metal fabrication)
• Stone-cutting, masonry
• Ceramic and glass manufacturing
• Foundry work
Pathogenesis (silica is uniquely fibrogenic):
Silica surfaces have reactive silanol groups that interact with phospholipids and proteins on phagolysosomal membranes. This causes:
1. NLRP3 inflammasome activation → IL-1β release
2. Phagolysosome rupture → macrophage death → particle re-release (amplification loop)
3. Intense fibroblast stimulation → whorled hyaline collagen
Morphology:
• Grossly: firm, greyish-white nodules, upper lobes predominantly
• Histologically: silicotic nodule — concentrically arranged (whorled) layers of hyalinised collagen with a cellular zone at the periphery
• Under polarised light: birefringent silica particles within the nodule
• Lymph nodes: enlarged, calcified; classic 'eggshell calcification' on X-ray (peripheral rim calcification of hilar nodes)

Silicotic Nodule: Histology and Pathogenesis
Special risks of silicosis:
1. ↑ TB susceptibility: Silica impairs macrophage bactericidal function — silica-loaded macrophages cannot kill Mycobacterium tuberculosis effectively. 'Silicotuberculosis' is a recognised entity; lesions may cavitate and look like primary progressive TB.
2. Eggshell calcification of hilar lymph nodes — virtually pathognomonic on X-ray
3. Lung cancer risk: IARC classifies crystalline silica as Group 1 carcinogen
4. Progression may continue after cessation of exposure (unlike coal dust)
Accelerated silicosis: Occurs within 5–10 years of intense exposure (sandblasters); ordinary silicosis takes 20–45 years.
SELF-CHECK
A sandblaster develops bilateral upper-lobe fibrosis with 'eggshell' calcification of hilar nodes. He is also found to have AFB-positive sputum. What is the most likely explanation for his TB?
A. Silica directly infects macrophages with mycobacteria
B. Silica impairs macrophage bactericidal capacity, reducing ability to kill M. tuberculosis
C. Eggshell calcification ruptures into airways, seeding TB
D. PMF cavities provide an anaerobic environment for TB growth
Reveal Answer
Answer: B. Silica impairs macrophage bactericidal capacity, reducing ability to kill M. tuberculosis
Silica particles within macrophage phagolysosomes impair the oxidative burst and lysosomal killing mechanisms that normally destroy mycobacteria. The result is failed clearance of M. tuberculosis from the alveolar macrophage pool — the same cell type that is the primary host for mycobacteria. This is an acquired cellular immune defect confined to silica-exposed lung macrophages, not a systemic immunodeficiency.
Asbestosis
Asbestosis: Fibres, Fibrosis, and Pleural Disease
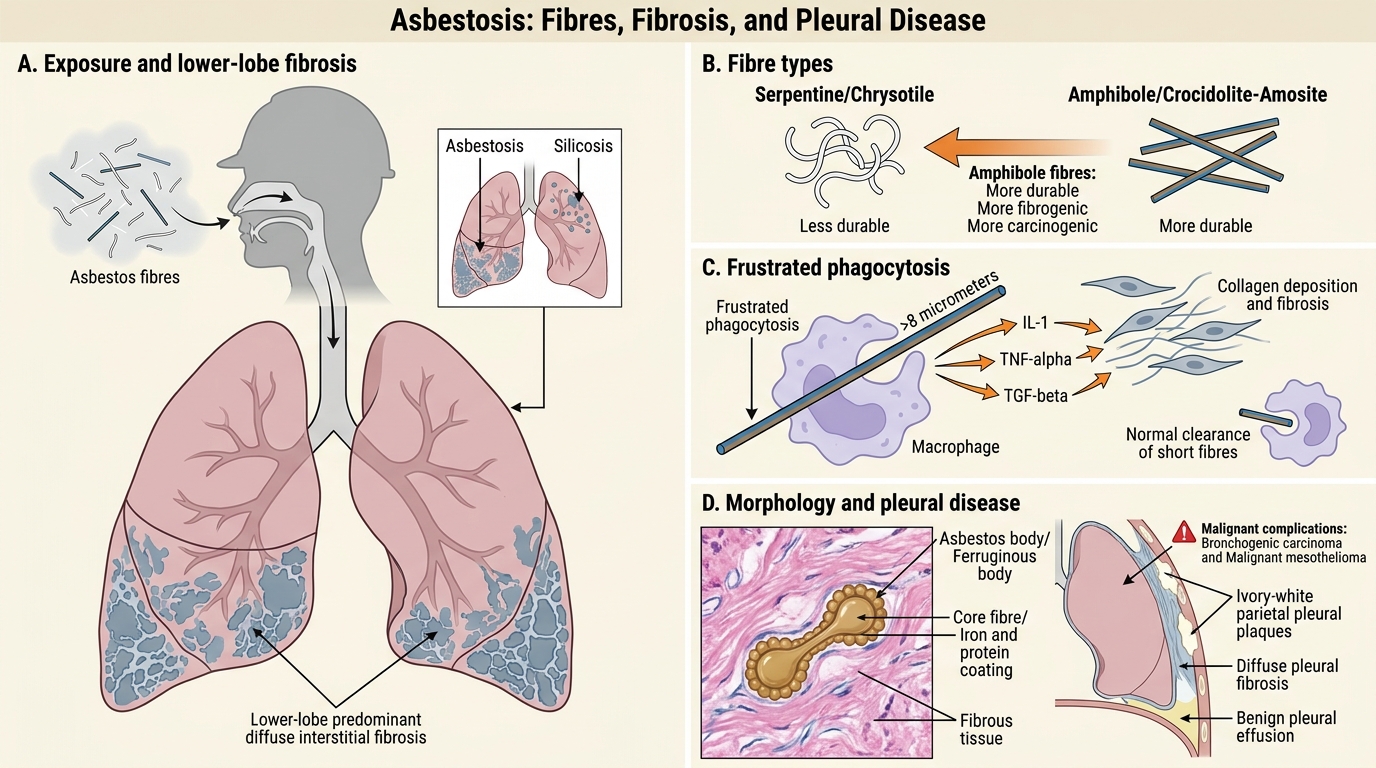
Asbestos is a family of naturally occurring silicate minerals that separate into thin fibres. Two main types:
• Serpentine (chrysotile — 'white asbestos'): curly, flexible fibres; cleared more easily; still fibrogenic
• Amphibole (crocidolite 'blue', amosite 'brown'): straight, rigid, durable; MORE carcinogenic and fibrogenic
High-risk occupations: insulation work, roofing, shipbuilding, brake-lining manufacture, construction demolition.
Pathogenesis: Long fibres (>8 µm) cannot be fully engulfed by macrophages → frustrated phagocytosis → persistent fibrogenic cytokine release (IL-1, TNF-α, TGF-β). Short fibres cleared normally.
Morphology:
Asbestosis (pulmonary fibrosis):
• Diffuse interstitial fibrosis — starts in lower lobes (contrast silicosis: upper lobes)
• Honeycombing in end-stage
• Asbestos bodies (ferruginous bodies): asbestos fibres coated with haemosiderin + protein — golden-brown, dumbbell-shaped or beaded rods visible on H&E
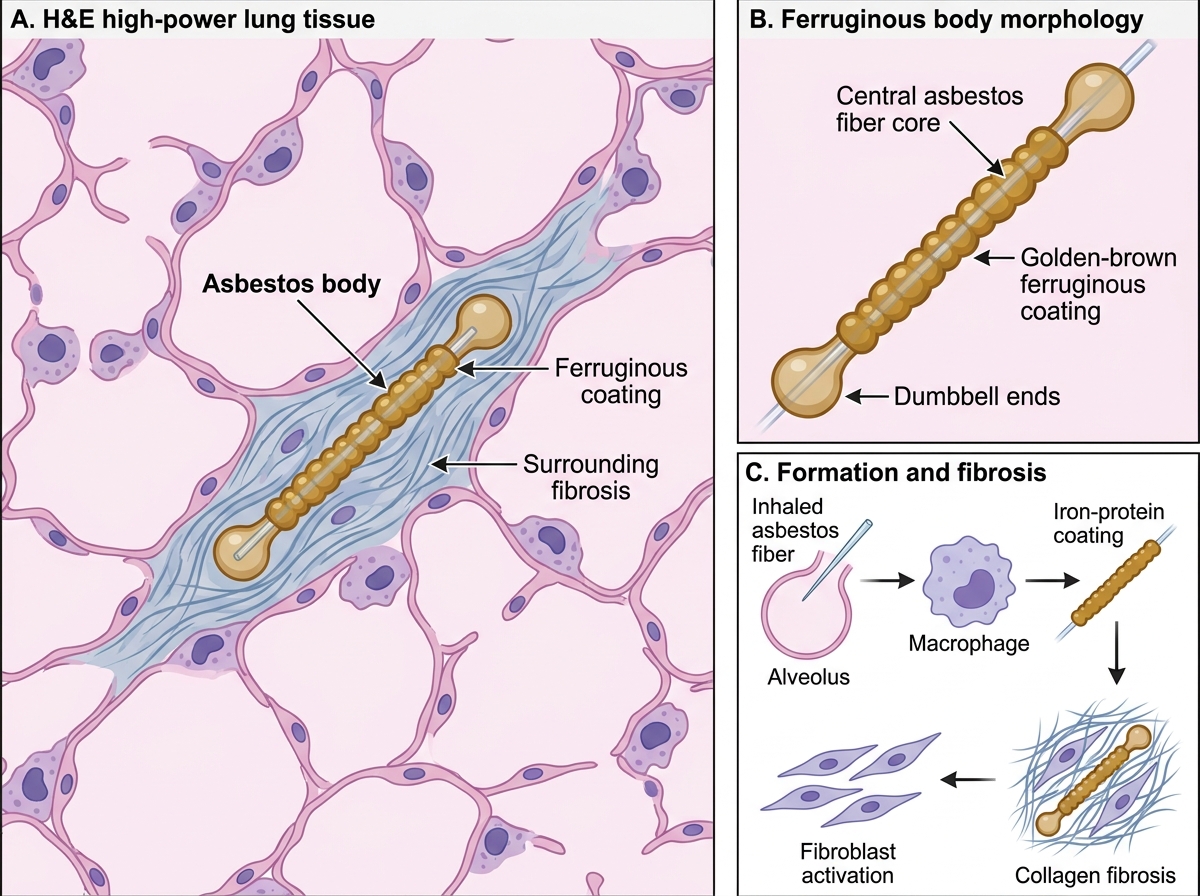
Asbestos Body in Lung Tissue
Pleural disease (does NOT require heavy parenchymal disease):
• Pleural plaques: discrete, ivory-white, acellular hyaline collagen on parietal pleura — most common asbestos-related lesion; not pre-malignant
• Diffuse pleural fibrosis, pleural effusion (benign)
Malignant complications — the critical associations:
| Malignancy | Relative risk (vs unexposed) | Notes |
|---|---|---|
| Mesothelioma | 1000-fold ↑ | Malignant tumour of pleural/peritoneal mesothelium; LONG latency (30–40 years); not dose-dependent — even brief exposure sufficient |
| Bronchogenic carcinoma | 5-fold ↑ (synergistic with smoking: 55-fold ↑) | All cell types; smoking + asbestos = multiplicative, not additive |
> Cross-reference: Mesothelioma morphology (epithelioid, sarcomatoid, biphasic) is covered in the RS Tumours SDL.
Dose-response: For asbestosis and bronchogenic carcinoma, risk is dose-dependent. For mesothelioma, even brief low-level exposure is sufficient — no safe threshold.
Pneumoconioses — Comparison at a Glance
Major Pneumoconioses: Comparison at a Glance
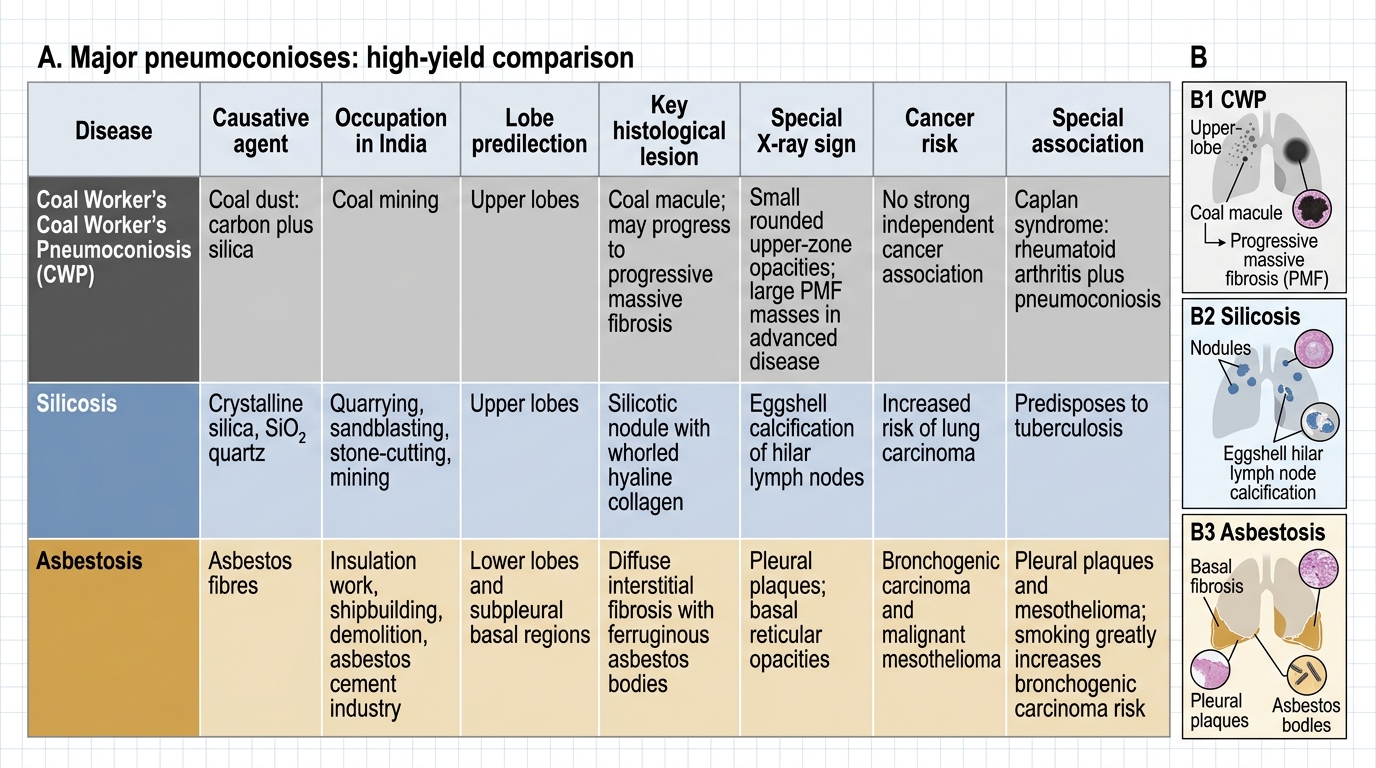
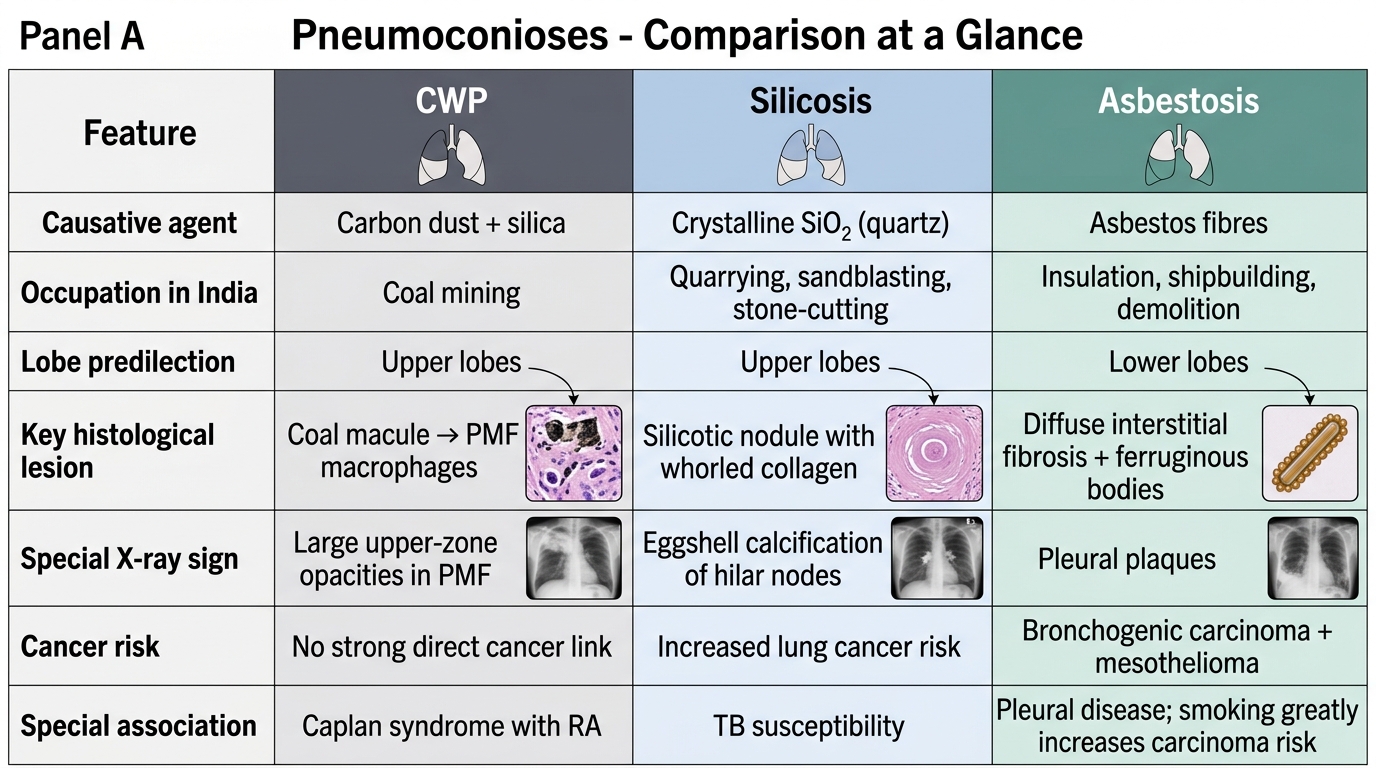
Major Pneumoconioses: CWP, Silicosis, and Asbestosis
| Feature | CWP | Silicosis | Asbestosis |
|---|---|---|---|
| Agent | Carbon + silica | Crystalline SiO₂ (quartz) | Asbestos fibres |
| Occupation | Coal mining | Quarrying, sandblasting, stone-cutting | Insulation, shipbuilding, demolition |
| Lobe | Upper | Upper | Lower |
| Key lesion | Coal macule → PMF | Silicotic nodule (whorled hyaline collagen) | Diffuse interstitial fibrosis + asbestos bodies |
| Specific marker | Anthracotic pigment, PMF | Birefringent particles, eggshell calcification | Asbestos/ferruginous bodies, pleural plaques |
| Cancer risk | Minimal | ↑ Lung Ca (Group 1 IARC) | ↑↑ Mesothelioma; ↑ Bronchogenic Ca |
| Special association | Caplan syndrome (RA) | Silicotuberculosis | Pleural plaques (not pre-malignant) |
CLINICAL PEARL
The 'lower lobe' clue in asbestosis: All three major pneumoconioses are associated with upper-lobe predominance EXCEPT asbestosis, which preferentially affects the lower lobes. This is because asbestos fibres, being longer and less easily deflected, travel further down to sub-pleural lower lobe alveoli. In any exam question or clinical case, lower-lobe fibrosis + occupational history = think asbestos first.
Synergy with smoking: Asbestos alone increases lung cancer risk ~5×. Smoking alone ~10×. Together: ~55×. This multiplicative (not merely additive) interaction is a favourite exam point and a critical counselling message for asbestos-exposed workers.