Page 16 of 32
PA25.5 | Occupational & Interstitial Lung Disease — SDL Guide (Part 4)
Shared Complications of Progressive ILD
Shared Complications of Progressive ILD
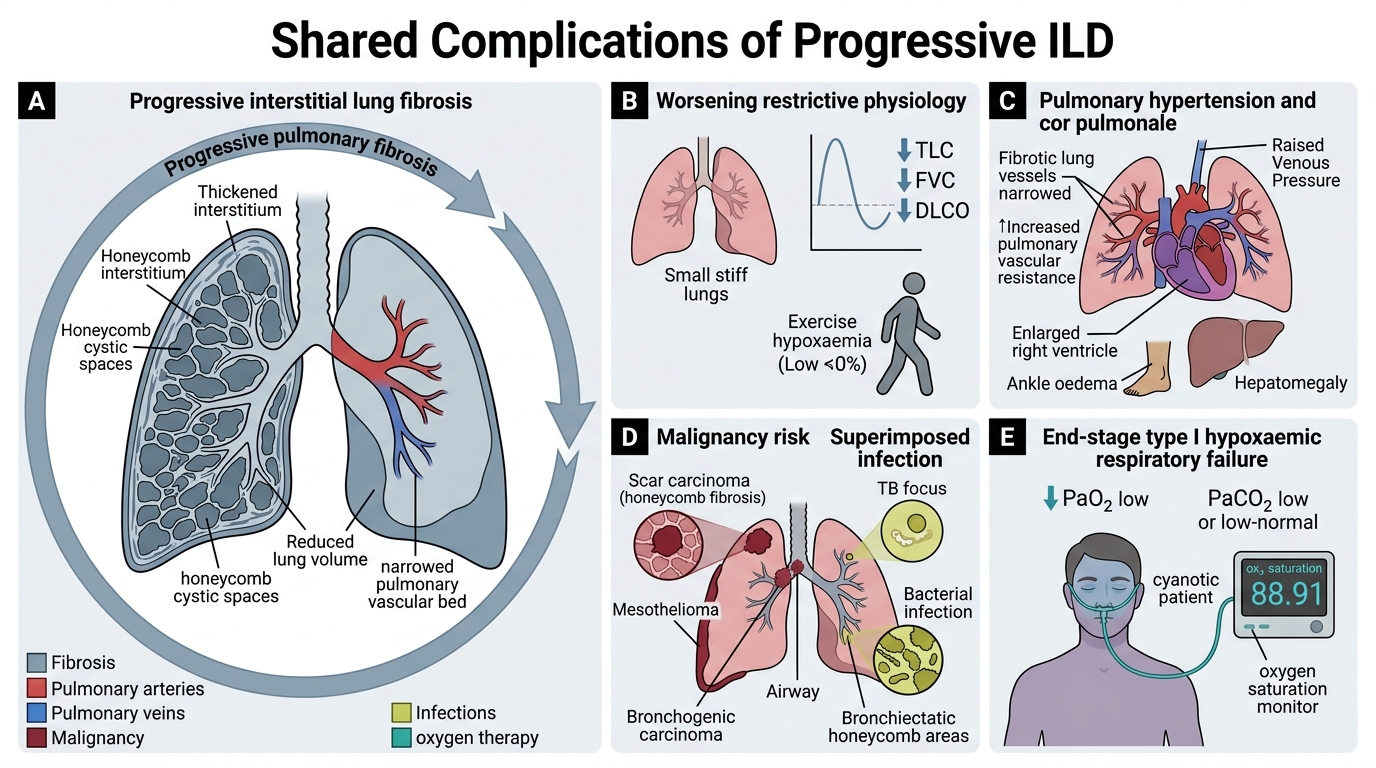
Regardless of the initial cause, progressive pulmonary fibrosis leads to a predictable cascade of complications:
1. Worsening restrictive physiology
• ↓ TLC, ↓ FVC, ↓ DLCO (diffusion capacity)
• Exercise-induced hypoxaemia before resting hypoxaemia
2. Pulmonary hypertension
• Fibrosis obliterates the pulmonary vascular bed → ↑ pulmonary vascular resistance
• Hypoxic vasoconstriction compounds the problem
3. Cor pulmonale
• Cor pulmonale (right heart failure from pulmonary hypertension): right ventricular hypertrophy → dilatation → failure
• Clinically: raised JVP, peripheral oedema, hepatomegaly
• This is the most common cause of death in pneumoconioses
4. Malignancy
• As covered: silicosis → lung Ca; asbestosis → mesothelioma + bronchogenic Ca
• Chronic fibrosis (any cause) also confers a modest ↑ risk of lung adenocarcinoma (honeycomb scar carcinoma)
5. Superimposed infection
• Silicosis → TB (silicotuberculosis)
• Non-specific bacterial infections in bronchiectatic / honeycomb areas
6. Respiratory failure
• End-stage: type I (hypoxaemic) respiratory failure requiring supplemental oxygen
CLINICAL PEARL
Taking an occupational history — a clinical skill this SDL trains: PA25.5 is not only about histopathology; it is about recognising the exposure-disease link. Always ask: 'What is your occupation? How long have you done it? Are you exposed to dust, fibres, or fumes? Do you use protective equipment?' In India, many patients do not volunteer occupational history — you must ask.
Latency trap: Mesothelioma may appear 30–40 years after asbestos exposure, long after the patient has changed jobs or retired. The index of suspicion must survive the patient's job change.
SELF-CHECK
Which of the following statements about asbestos bodies (ferruginous bodies) is CORRECT?
A. Their presence alone is diagnostic of asbestosis (diffuse pulmonary fibrosis)
B. They are found only in asbestosis, not in normal urban lungs
C. They are found predominantly in upper lobes, similar to silicotic nodules
D. They represent the asbestos fibre coated with haemosiderin and protein, appearing as golden-brown beaded rods
Reveal Answer
Answer: D. They represent the asbestos fibre coated with haemosiderin and protein, appearing as golden-brown beaded rods
Asbestos bodies (ferruginous bodies) are asbestos fibres coated with an iron-protein complex (haemosiderin + glycoprotein), producing the characteristic golden-brown, dumbbell-shaped or beaded rod appearance on H&E. Option A is wrong — asbestos bodies are a marker of exposure, not of disease; asbestosis requires additional clinical-radiological-pathological correlation. Option B is wrong — asbestos bodies can be found in lungs of people with low-level environmental exposure without clinical disease. Option C is wrong — asbestosis is a lower-lobe disease, unlike silicosis.