Page 1 of 32
PA25.1-2 | Pneumonia & Lung Abscess — SDL Guide
Learning Objectives
- Define pneumonia and classify it by aetiology, acquisition setting, and anatomical pattern.
- Describe the four classical stages of lobar pneumonia with their gross and microscopic features.
- Distinguish lobar pneumonia from bronchopneumonia and interstitial pneumonia on pathological grounds.
- Explain the mechanisms that normally protect the lung and how their failure precipitates pneumonia.
- Enumerate the complications of pneumonia and recognise their pathological basis.
- Describe the aetiology, gross and microscopic features, and complications of lung abscess (PA25.2).
INSTRUCTIONS
Pneumonia remains one of the top-five causes of death globally and is among the commonest conditions encountered in clinical practice. Understanding its pathological basis — why a consolidating lobe looks and feels different at each stage, why an abscess forms in a dependent segment after aspiration, and how a suppurative process can seed the brain — gives you a predictive framework that makes clinical signs and radiology instantly interpretable. This module builds that framework from first principles.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch 15 (The Lung) (textbook)
- Harsh Mohan — Textbook of Pathology, 7th ed., Ch 17 (Respiratory System) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 65-year-old smoker with poorly controlled diabetes presents with high fever, pleuritic chest pain, and rusty-brown sputum. His chest X-ray shows complete opacification of the right lower lobe. Three days later the same lobe, now slightly darker on imaging, begins to re-aerate from the periphery. A week after that, the radiograph is nearly clear. What was happening inside that lobe on each of those days — and why does the sputum turn rusty? By the time you finish this module you will be able to narrate the story of that lobe, stage by stage, in cellular and molecular terms.
WHY THIS MATTERS
Pneumonia accounts for more than 2.5 million deaths per year globally. In India, it is the single leading infectious cause of under-5 mortality. For a Year-2 MBBS student, pneumonia is a nexus topic: it links your Year-1 knowledge of innate immunity, vascular physiology, and respiratory anatomy directly to clinical signs (dullness to percussion, bronchial breathing, aegophony), radiology (air-space vs interstitial patterns), and microbiology (Gram-positive cocci vs atypical organisms). The lung abscess section extends this into surgical and intensive-care territory — foul sputum and clubbing are classic long-case findings.
RECALL
Before proceeding, recall the following from Year 1:
• Innate lung defences: mucociliary escalator, alveolar macrophages, surfactant, secretory IgA, cough reflex, tight junctions of alveolar epithelium.
• Exudate vs transudate: the vascular permeability mechanism driving exudate formation.
• Neutrophil recruitment cascade: margination → rolling → adhesion (ICAM-1/selectin) → diapedesis → chemotaxis (IL-8, C5a, LTB4).
• Basic lung anatomy: acinus, terminal bronchiole, respiratory bronchiole, alveolar duct, alveolus; hilum, lobar and segmental bronchi.
If any of these feel shaky, spend five minutes with your PY or AN notes before continuing — the pathology will make far more sense.
Definition and Classification of Pneumonia
Definition and Classification of Pneumonia
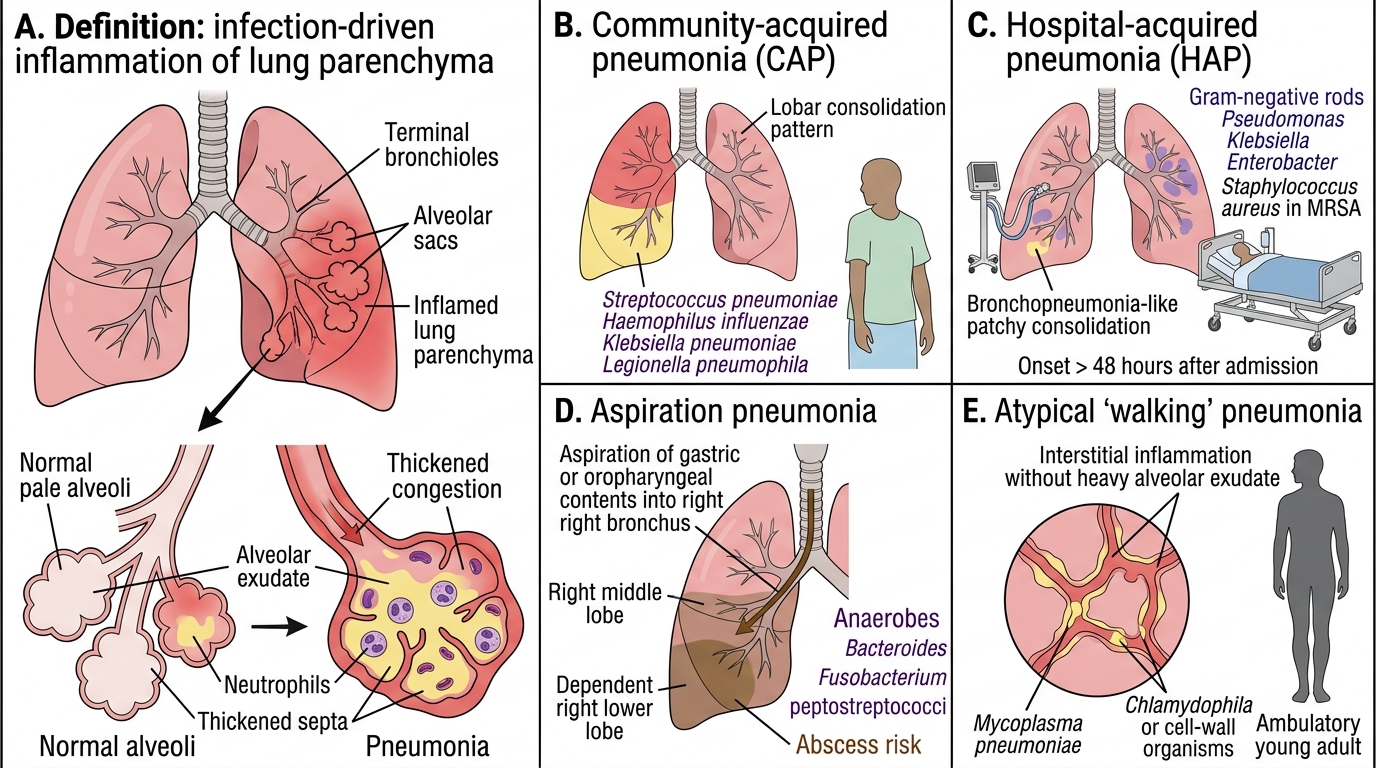
Pneumonia is defined as infection-driven inflammation of the lung parenchyma (alveoli and/or terminal airways). The term encompasses a wide range of diseases; two complementary classification systems are used clinically and pathologically.
Classification by acquisition setting
1. Community-acquired pneumonia (CAP): onset outside hospital or within 48 hours of admission. Principal agent: Streptococcus pneumoniae (causing the classical lobar pattern in immunocompetent adults). Others: Haemophilus influenzae, Klebsiella pneumoniae (classically in alcoholics — 'currant jelly' sputum), Legionella pneumophila (atypical CAP).
2. Hospital-acquired (nosocomial) pneumonia (HAP): onset >48 hours after admission. Flora shifts toward Gram-negative rods (Pseudomonas, Klebsiella, Enterobacter) and Staphylococcus aureus (including MRSA). Occurs in ventilated, immunosuppressed, or post-operative patients.
3. Aspiration pneumonia: inhalation of oropharyngeal or gastric contents. Typically mixed flora (anaerobes: Bacteroides, Fusobacterium, peptostreptococci). Location: right lower lobe (supine) or right middle lobe (semi-upright) because the right main bronchus is wider and more vertical. Predisposes strongly to abscess formation.
4. Atypical (walking) pneumonia: caused by organisms that lack a peptidoglycan cell wall or are intracellular. Mycoplasma pneumoniae (commonest cause of atypical CAP in young adults), Chlamydophila pneumoniae, influenza virus, SARS-CoV-2, Legionella pneumophila (shares features of both typical and atypical). Characteristically produces interstitial/diffuse alveolar damage rather than lobar consolidation; Gram stain negative; does not respond to beta-lactams.
Classification by anatomical pattern (the pathologist's lens — and the focus of this module)
| Pattern | Distribution | Histology | Key agent |
|---|---|---|---|
| Lobar pneumonia | Entire lobe | Alveolar exudate | S. pneumoniae |
| Bronchopneumonia | Patchy, peri-bronchial, bilateral | Neutrophilic bronchiolitis + alveolitis | Mixed/secondary |
| Interstitial pneumonia | Alveolar walls/septa | Mononuclear infiltrate, thickened septa | Viruses, Mycoplasma |
SELF-CHECK
A 30-year-old college student presents with gradual onset of fever, non-productive cough, and bilateral patchy infiltrates on X-ray. Sputum Gram stain shows no organisms. Which pathological lung pattern does this most likely represent?
A. Lobar pneumonia
B. Bronchopneumonia
C. Interstitial (atypical) pneumonia
D. Lung abscess
Reveal Answer
Answer: C. Interstitial (atypical) pneumonia
Gradual onset, non-productive cough, bilateral patchy (not lobar) infiltrates, and a negative Gram stain in a young adult are classic features of atypical (interstitial) pneumonia — most commonly caused by Mycoplasma pneumoniae. The organism lacks a cell wall (Gram-stain invisible) and spreads via alveolar walls rather than filling alveolar spaces, producing interstitial thickening rather than lobar consolidation.
Pathogenesis — How Lung Defences Fail
Pathogenesis of Pneumonia: How Lung Defences Fail
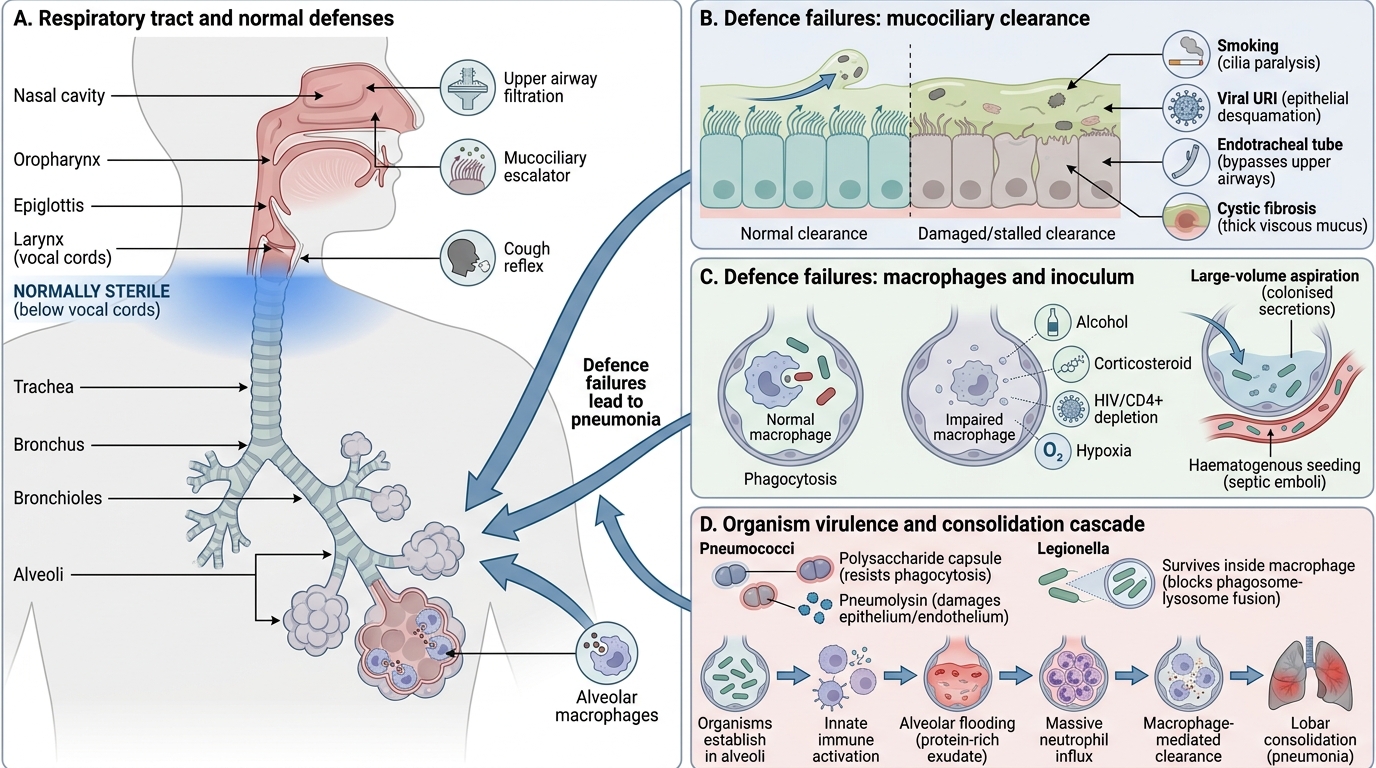
The healthy lung below the vocal cords is normally sterile. Pneumonia requires one or more of the following defence failures:
- Impaired mucociliary clearance: smoking (ciliotoxic), viral URI (desquamates epithelium), intubation (bypasses upper airways), cystic fibrosis (viscous mucus trap).
- Impaired alveolar macrophage function: alcohol (inhibits macrophage oxidative burst and opsonisation), corticosteroids, HIV (depletes CD4+ T-helper cells that activate macrophages), hypoxia.
- Overwhelmed defences by inoculum size: aspiration of large volume of colonised secretions, haematogenous seeding from a distant infective focus (septic emboli).
- Virulence factors of the organism: S. pneumoniae polysaccharide capsule resists phagocytosis; pneumolysin (a cholesterol-dependent cytolysin) disrupts alveolar epithelia and endothelia; Legionella survives intracellularly within macrophages by blocking phagosome–lysosome fusion.
Once organisms establish in alveoli, the innate immune cascade produces the hallmark changes of consolidation — alveolar flooding, massive neutrophil influx, and eventual macrophage-mediated clearance. This cascade is precisely what the four stages of lobar pneumonia describe.
Lobar Pneumonia — The Four Classic Stages
Four Classic Stages of Lobar Pneumonia
Lobar pneumonia proceeds through four sequential pathological stages. In the antibiotic era, patients rarely complete all four stages uninterrupted, but the stages remain the foundation of understanding consolidation.
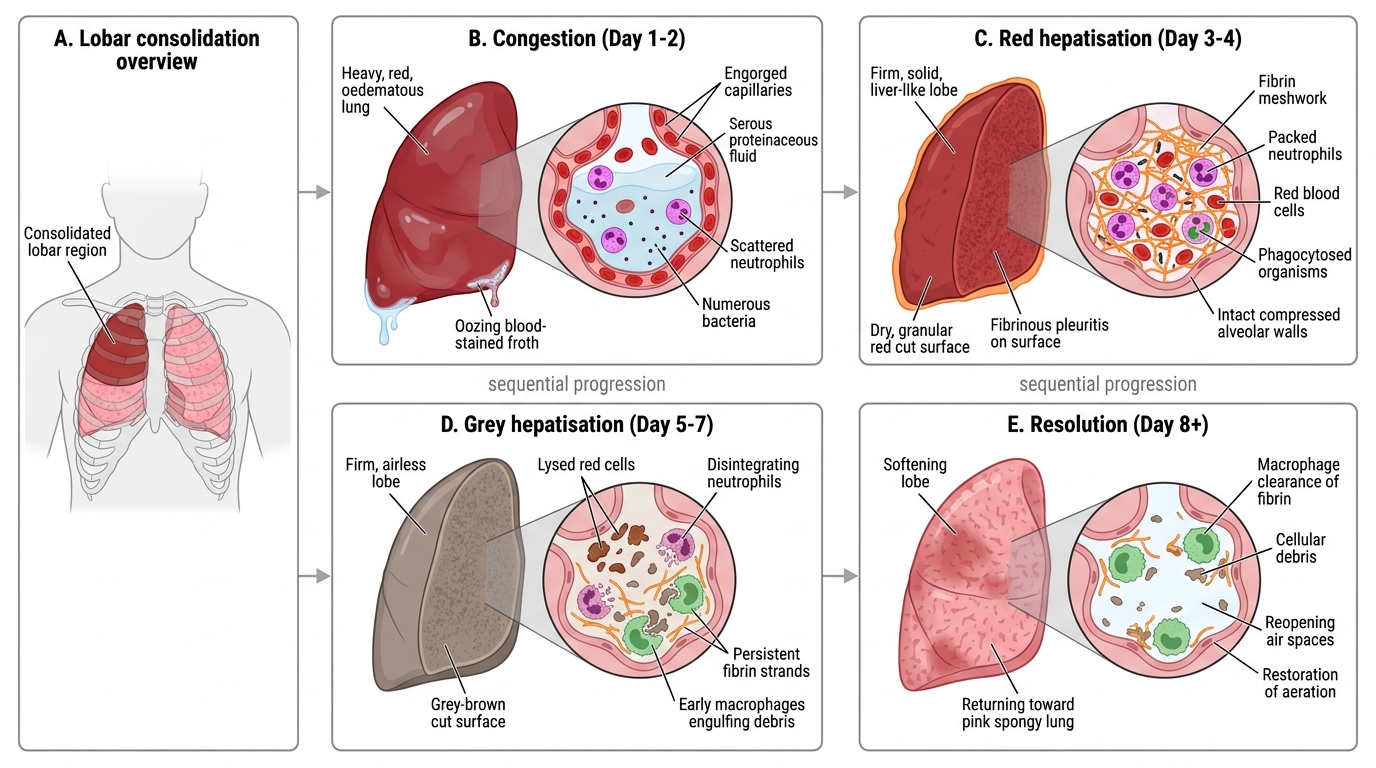
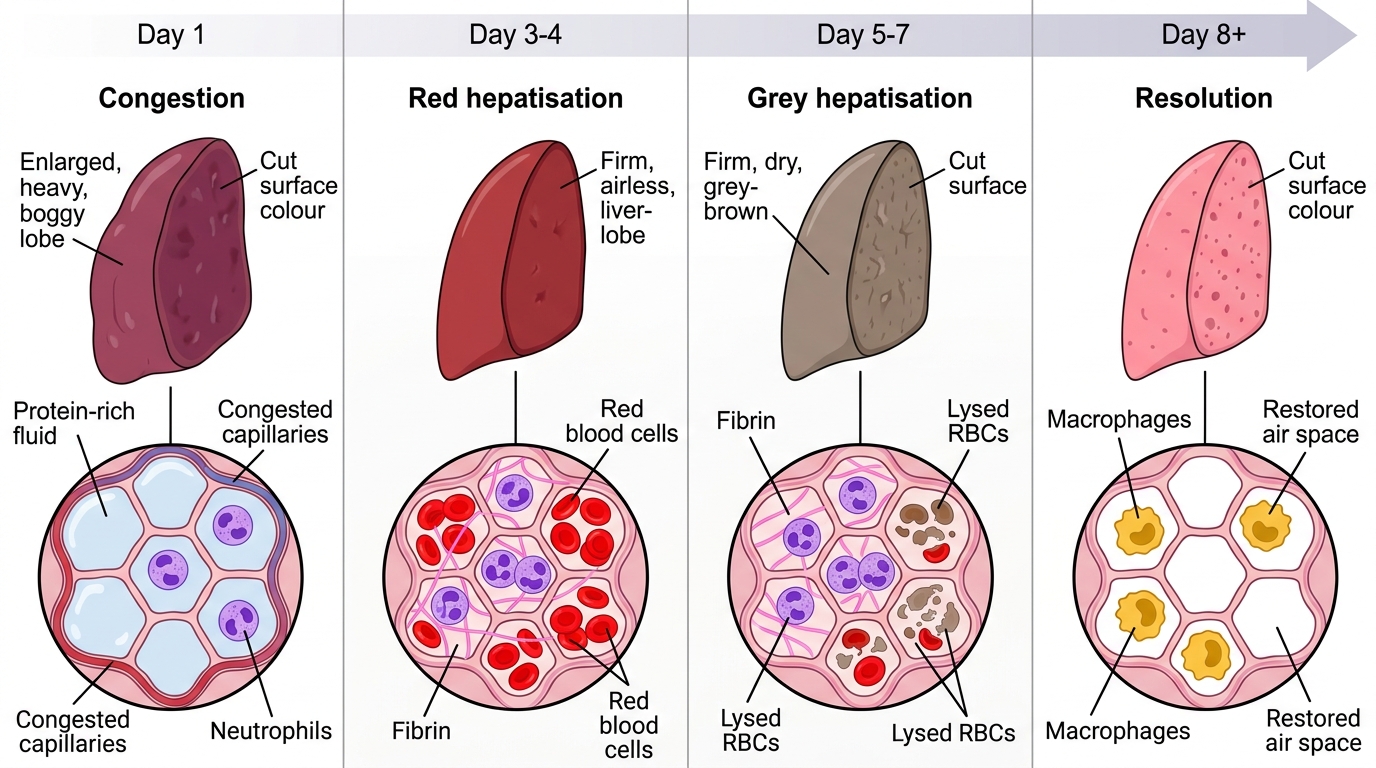
Stage 1 — Congestion (Day 1–2)
- Gross: lobe is heavy, red-red, and oedematous; cuts with blood-stained froth.
- Micro: alveolar capillaries are engorged; alveoli contain serous, proteinaceous fluid with scattered neutrophils; organisms are abundant.
- Mechanism: bacterial products trigger vasodilation and increased vascular permeability (IL-1, TNF-α, complement).
Stage 2 — Red Hepatisation (Day 3–4)
- Gross: lobe is firm, airless, liver-like (hepatisation); cut surface is dark red and dry. Pleuritis often visible on surface.
- Micro: alveoli packed with fibrin meshwork, neutrophils, and red blood cells (the red colour). Alveolar walls intact but compressed. Organisms phagocytosed by neutrophils.
- Mechanism: fibrinogen leaks out, polymerises to fibrin; RBCs extravasate through damaged capillaries.
Stage 3 — Grey Hepatisation (Day 5–7)
- Gross: lobe remains firm and airless but turns grey-brown (RBCs lysed).
- Micro: neutrophils disintegrate; fibrin strands remain; macrophages begin to appear and engulf debris. Fewer RBCs (hence grey).
- Mechanism: neutrophil apoptosis; macrophage recruitment driven by IL-4, IL-10 (resolution phase cytokines).
Stage 4 — Resolution (Day 8+)
- Gross: lobe softens; cut surface becomes granular and then normal-looking as air re-enters.
- Micro: macrophages phagocytose fibrin and cellular debris; proteolytic enzymes (plasminogen activator, elastase) digest the exudate; normal alveolar architecture restored.
- Mechanism: fibrinolysis; alveolar epithelial regeneration (type II pneumocytes proliferate → differentiate → type I). Lymphatics carry cleared debris.
- Clinical correlate: 'post-pneumonic fibrosis' (organisation) may occur if resolution fails — fibrin organises into fibrous tissue (carnification).
IMPORTANT NOTE: the stages merge and overlap; modern imaging often shows partial resolution within 5–7 days with antibiotics.
Stages of Lobar Pneumonia
SELF-CHECK
On autopsy of a patient who died on Day 4 of untreated pneumococcal pneumonia, the pathologist finds the right lower lobe firm, dark red, and airless, with alveoli packed with fibrin, neutrophils, and red blood cells. Which stage of lobar pneumonia does this represent?
A. Congestion
B. Red hepatisation
C. Grey hepatisation
D. Resolution
Reveal Answer
Answer: B. Red hepatisation
Dark red, liver-like firmness with alveoli packed by fibrin, neutrophils, AND red blood cells is the hallmark of red hepatisation (Stage 2, Day 3–4). The red colour is conferred by RBC extravasation. In grey hepatisation the RBCs lyse (lobe turns grey-brown) and macrophages appear. In congestion the lobe is engorged but not yet fibrinous; in resolution, macrophages dominate and the lobe softens.