Page 2 of 32
PA25.1-2 | Pneumonia & Lung Abscess — SDL Guide (Part 2)
Bronchopneumonia — Patchy Consolidation
Bronchopneumonia: Patchy Peribronchial Consolidation
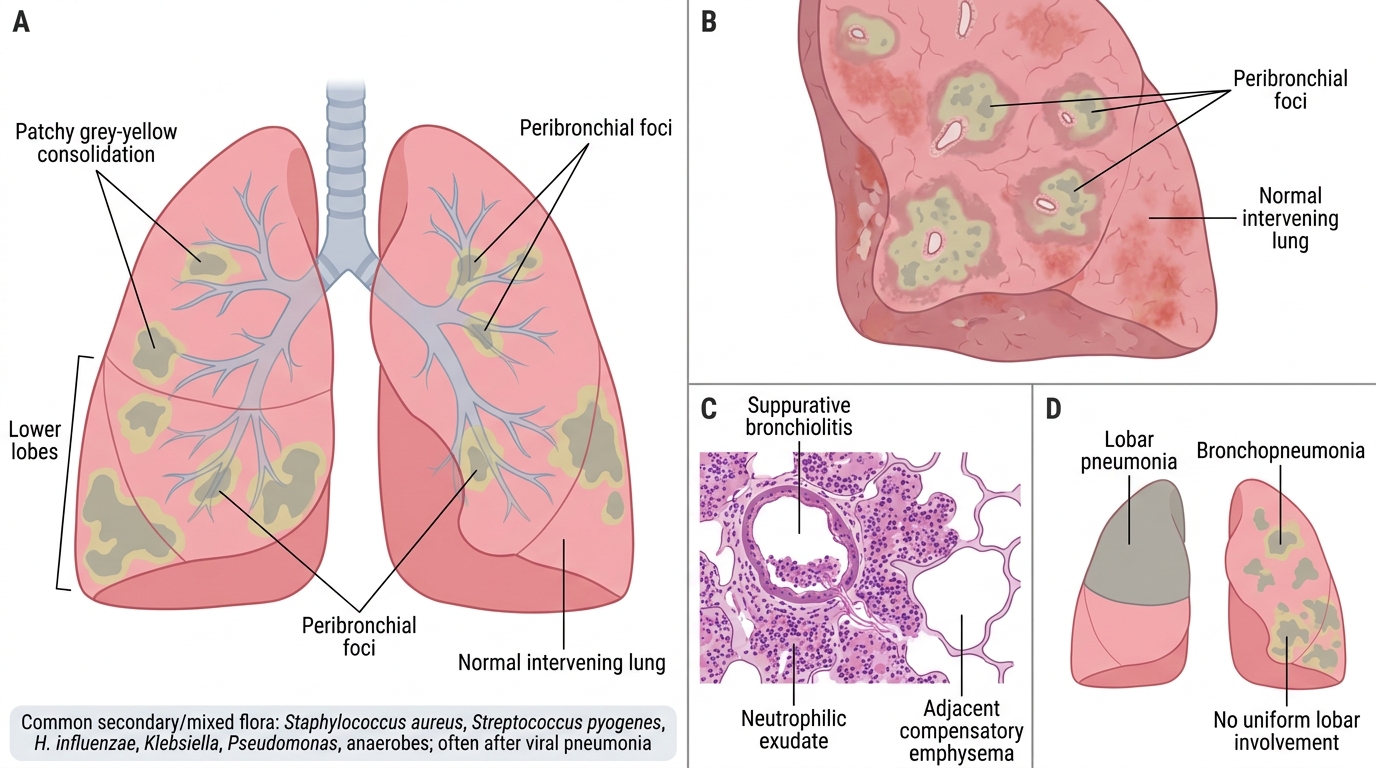
Bronchopneumonia (lobular pneumonia) is the other major anatomical pattern of acute bacterial pneumonia. It is more common than lobar pneumonia at the extremes of age (infants, elderly) and in hospitalised, debilitated, or post-surgical patients.
Macroscopic features
- Multiple foci of grey-yellow consolidation (2–4 cm patches), typically bilateral and predominantly in the lower lobes and posterior segments (gravity-dependent distribution).
- Foci are centred on bronchioles ('peribronchial' consolidation). Between foci, lung may be relatively normal or haemorrhagic.
Microscopic features
- Suppurative bronchiolitis: bronchiole and surrounding alveoli are filled with a neutrophilic exudate.
- Fibrin formation is less prominent than in lobar pneumonia.
- Adjacent alveoli may show compensatory emphysema.
- No stage-by-stage progression (lobe is not uniformly involved).
Causative organisms: secondary/mixed flora — Staphylococcus aureus, Streptococcus pyogenes, H. influenzae, Klebsiella, Pseudomonas, anaerobes. Also follows viral pneumonias (influenza superinfection).
Comparison with lobar pneumonia
| Feature | Lobar | Bronchopneumonia |
|---|---|---|
| Distribution | Entire lobe | Bilateral, patchy, lower lobes |
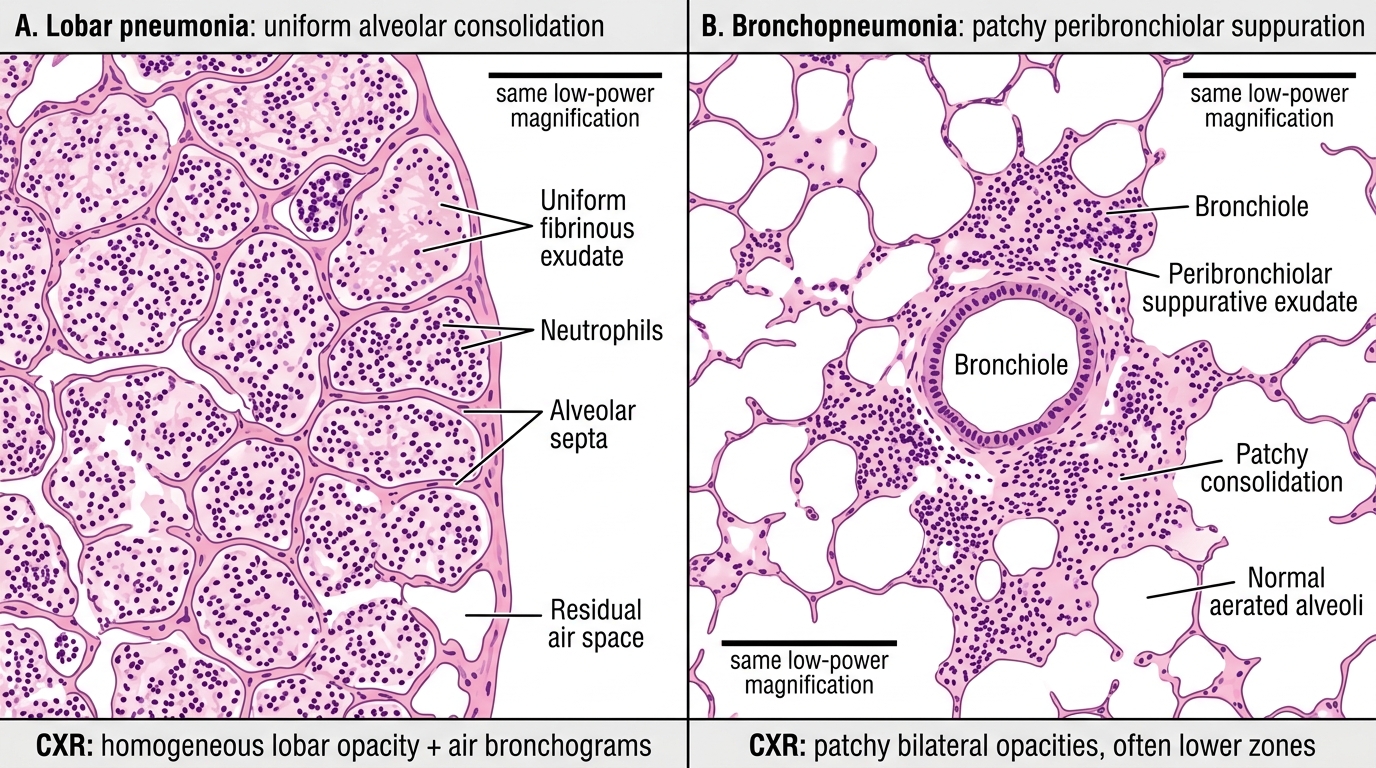
| Exudate centre | Alveoli | Bronchiole + surrounding alveoli |
| Fibrin | Abundant | Scanty |
| Stages | 4 classic stages | None |
| Common age | Young adults | Infants, elderly, debilitated |
| Primary agent | S. pneumoniae | Mixed; secondary |
| Prognosis | Better (with Rx) | Worse (underlying disease) |
Lobar Pneumonia vs Bronchopneumonia
CLINICAL PEARL
Clinical-radiological correlation: In lobar pneumonia, the entire lobe consolidates → chest X-ray shows a homogeneous opacity with air bronchograms (air-filled bronchi visible within the dense lobe). In bronchopneumonia, scattered foci of consolidation produce patchy bilateral opacities without a lobar distribution — sometimes called 'bilateral lower-zone haziness'. This difference is diagnostically important: if the CXR shows bilateral patchy shadowing in a 70-year-old who just had hip surgery, you should think bronchopneumonia (nosocomial, mixed flora, gram-negatives), not pneumococcal lobar pneumonia.
Complications of Pneumonia
Complications of Pneumonia
Most cases of bacterial pneumonia resolve without sequelae with appropriate antibiotic therapy. However, several clinically important complications can occur:
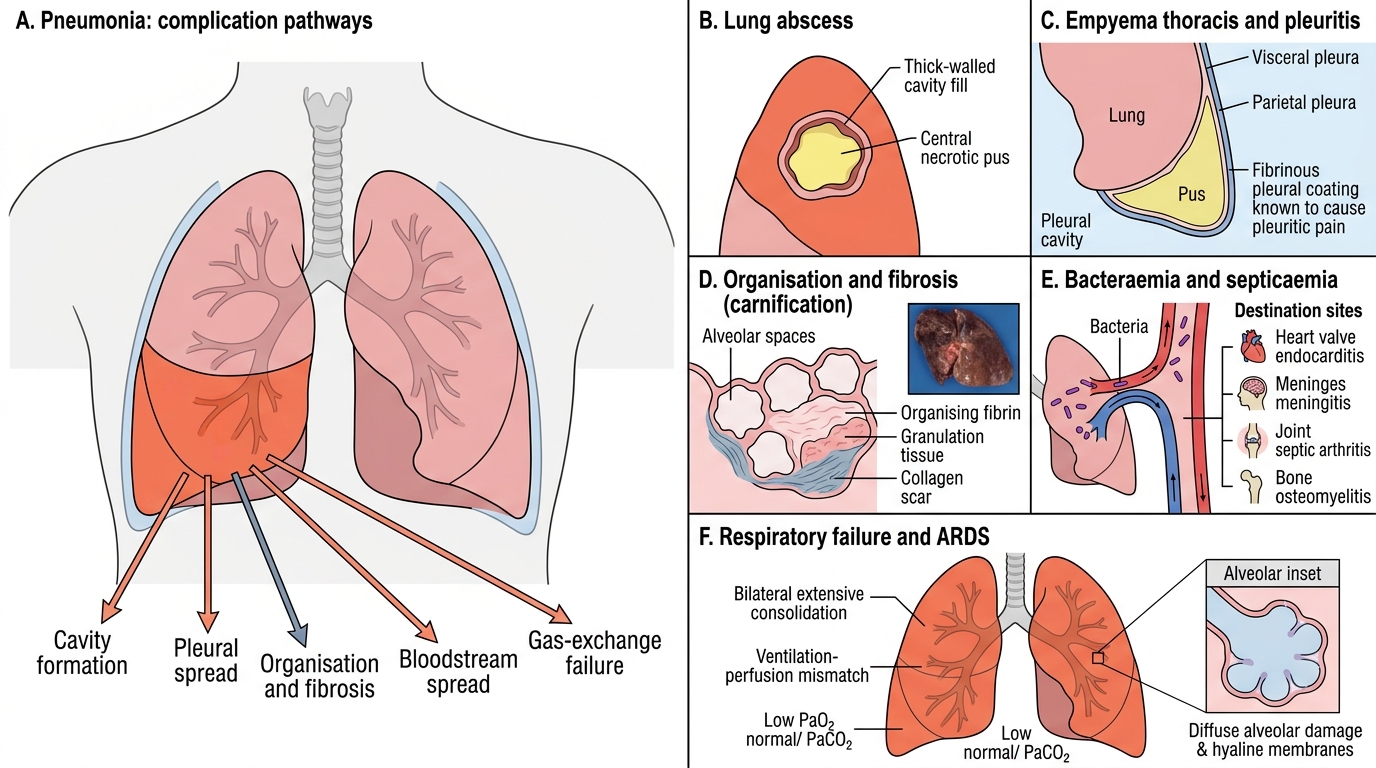
- Lung abscess: failure of resolution with central liquefactive necrosis → cavity formation. Particularly follows aspiration pneumonia, necrotising organisms (S. aureus, Klebsiella, anaerobes). Discussed in detail in the next section.
- Empyema thoracis (pyothorax): extension of infection across the visceral pleura → pus in the pleural cavity. Presents with systemic sepsis + dullness to percussion + reduced breath sounds. Requires chest drainage (intercostal tube or VATS decortication).
- Organisation and fibrosis (carnification): failure of fibrinolysis → fibrin organises into granulation tissue → collagenous scar replaces alveoli. Lobe becomes solid, dark, and shrunken ('fleshy' — carnification from carnis, flesh). Permanent loss of that lung segment's function.
- Bacteraemia and septicaemia: organisms enter pulmonary veins → systemic circulation → sepsis syndrome. Can seed heart valves (endocarditis), meninges (meningitis), joints (septic arthritis), or bones (osteomyelitis).
- Respiratory failure: bilateral extensive consolidation → ventilation–perfusion mismatch → type I respiratory failure (low PaO₂, normal/low PaCO₂). In severe cases: ARDS (diffuse alveolar damage superimposed).
- Pleuritis: fibrinous pleuritis over the involved lobe causes the classic pleuritic chest pain (sharp, worse on inspiration). Pleural rub on auscultation. Usually resolves with pneumonia.
SELF-CHECK
A 55-year-old alcoholic is treated for right lower-lobe pneumonia but continues to spike fever despite two weeks of antibiotics. Repeat CT chest shows a thick-walled cavity in the right lower lobe with an air-fluid level. Which complication of pneumonia has most likely developed?
A. Empyema thoracis
B. Carnification (organisation)
C. Lung abscess
D. Respiratory failure
Reveal Answer
Answer: C. Lung abscess
A thick-walled cavity with an air-fluid level on CT, persisting after pneumonia treatment in an alcoholic (who is at high risk for aspiration), is the classic presentation of a lung abscess. Empyema is pleural (not intrapulmonary) and appears as a D-shaped pleural fluid collection, not an intrapulmonary cavity. Carnification produces a solid, not cavitary, lobe. Respiratory failure would not produce a localised cavity.
Lung Abscess — Aetiology and Pathogenesis
Lung Abscess: Aetiology and Pathogenesis
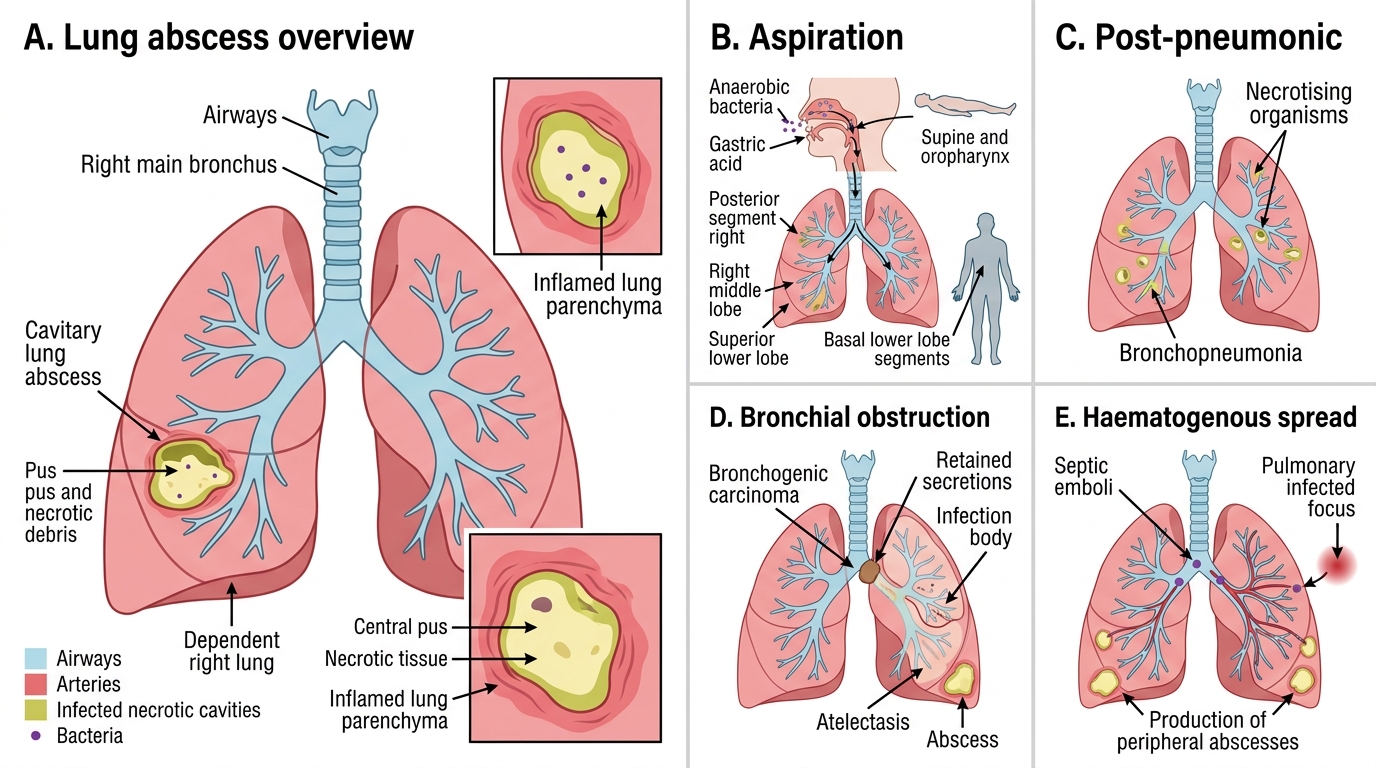
A lung abscess is a localised area of suppurative necrosis within the lung parenchyma, resulting in a cavity containing pus and necrotic tissue.
Aetiology — the four main mechanisms
1. Aspiration (commonest, ~60%)
- Predisposing states: altered consciousness (alcoholism, general anaesthesia, epilepsy, drug overdose, stroke), dysphagia (neurological disease, oesophageal disease), dental sepsis.
- Aspirated material: oropharyngeal bacteria (predominantly anaerobes — Bacteroides fragilis, Fusobacterium nucleatum, peptostreptococci) + gastric acid (chemical injury → secondary infection).
- Location: right lung > left lung (wider, more vertical right main bronchus); in supine patients — posterior segment of right upper lobe or superior segment of right lower lobe (these are the dependent segments in the supine position); in upright/semi-upright — right middle lobe or lower lobe basal segments).
2. Post-pneumonic (secondary to pneumonia)
- Necrotising organisms: Staphylococcus aureus (especially in children and post-influenza adults), Klebsiella pneumoniae (Type III — thick capsule, 'mucoid' colonies), Pseudomonas aeruginosa, anaerobes.
- Multiple small abscesses in bronchopneumonia pattern.
3. Bronchial obstruction
- Tumour (bronchogenic carcinoma — most important in adults >40), foreign body aspiration (especially in children), mucus plug.
- Mechanism: obstructive atelectasis → retained secretions → infection → abscess distal to obstruction.
- Clinical rule: any lung abscess in an adult >40 must prompt bronchoscopy to exclude carcinoma.
4. Septic emboli (haematogenous)
- Source: right-sided infective endocarditis (tricuspid valve), septic thrombophlebitis, IV drug users.
- Pattern: multiple, bilateral, peripheral abscesses.