Page 3 of 32
PA25.1-2 | Pneumonia & Lung Abscess — SDL Guide (Part 3)
Lung Abscess — Gross and Microscopic Features
Lung Abscess: Gross and Microscopic Features
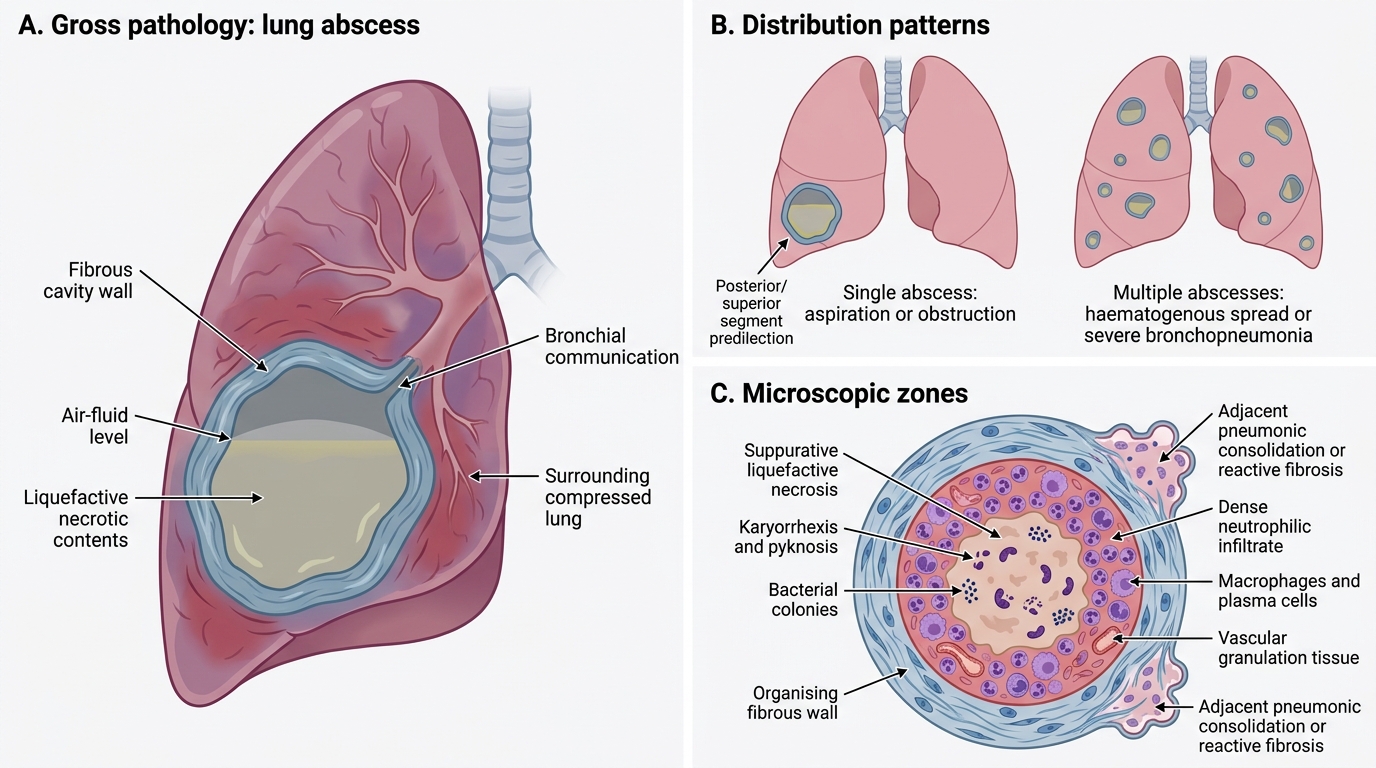
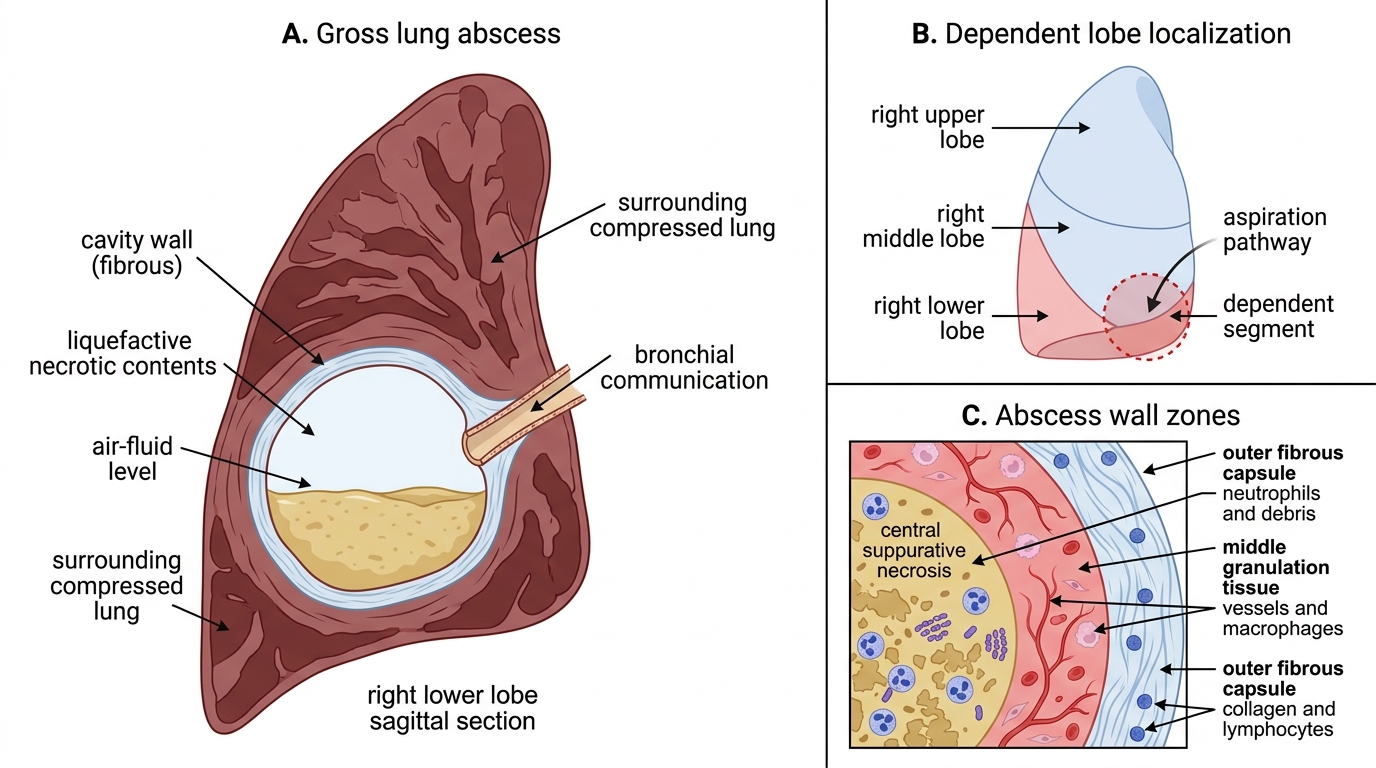
Gross pathology
- Single (aspiration, post-obstructive) or multiple (haematogenous, severe bronchopneumonia).
- Location: follows the mechanism (posterior/superior segments for aspiration — see above).
- Size: variable — 1 cm to >10 cm ('giant abscess').
- Cavity wall: initially ill-defined, ragged, and red-grey; over weeks the wall becomes thick and fibrous (white-grey, firm).
- Cavity contents: semi-liquid, greyish-yellow, foul-smelling purulent necrotic material (liquefactive necrosis).
- If communicates with a bronchus (usual): air-fluid level visible on chest X-ray / CT.
Gross Pathology of Lung Abscess
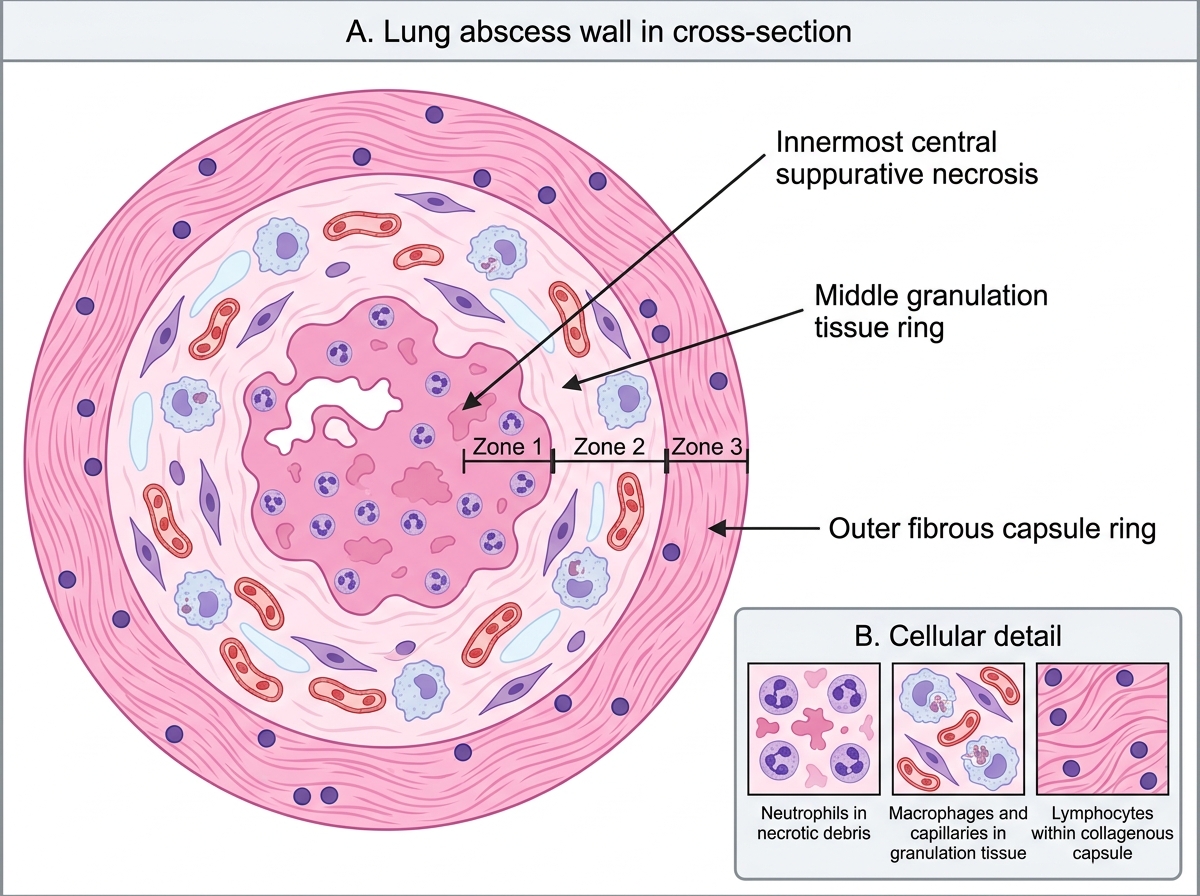
Microscopic pathology
- Central zone: suppurative (liquefactive) necrosis — amorphous eosinophilic debris, nuclear fragmentation (karyorrhexis, pyknosis of dead neutrophils), colonies of organisms.
- Mid-zone: dense neutrophilic infiltrate admixed with macrophages and plasma cells; vascular granulation tissue.
- Outer zone: organising fibrous wall (collagen, fibroblasts, lymphocytes); over time becomes a thick collagenous capsule.
- Adjacent lung: pneumonic consolidation or reactive fibrosis.
Microscopic Zones of a Lung Abscess Wall
SELF-CHECK
A pathology resident examining a lung abscess specimen notes the cavity is located in the posterior segment of the right upper lobe. Which aetiological mechanism is most consistent with this location?
A. Septic emboli from right-sided endocarditis
B. Aspiration in a supine patient
C. Obstructive carcinoma of the right upper lobe bronchus
D. Post-pneumonic abscess following bronchopneumonia
Reveal Answer
Answer: B. Aspiration in a supine patient
The posterior segment of the right upper lobe is a classically dependent segment in the supine position — the most likely landing zone for aspirated material in a recumbent (e.g. unconscious, post-operative) patient. Septic emboli from endocarditis typically produce multiple peripheral bilateral abscesses. Obstructive abscesses are distal to the obstruction and often accompanied by collapse/consolidation of the segment. Post-pneumonic abscesses follow bronchopneumonia's patchy bilateral lower-lobe pattern.
Lung Abscess — Complications and Clinical Features
Lung Abscess: Clinical Features and Complications
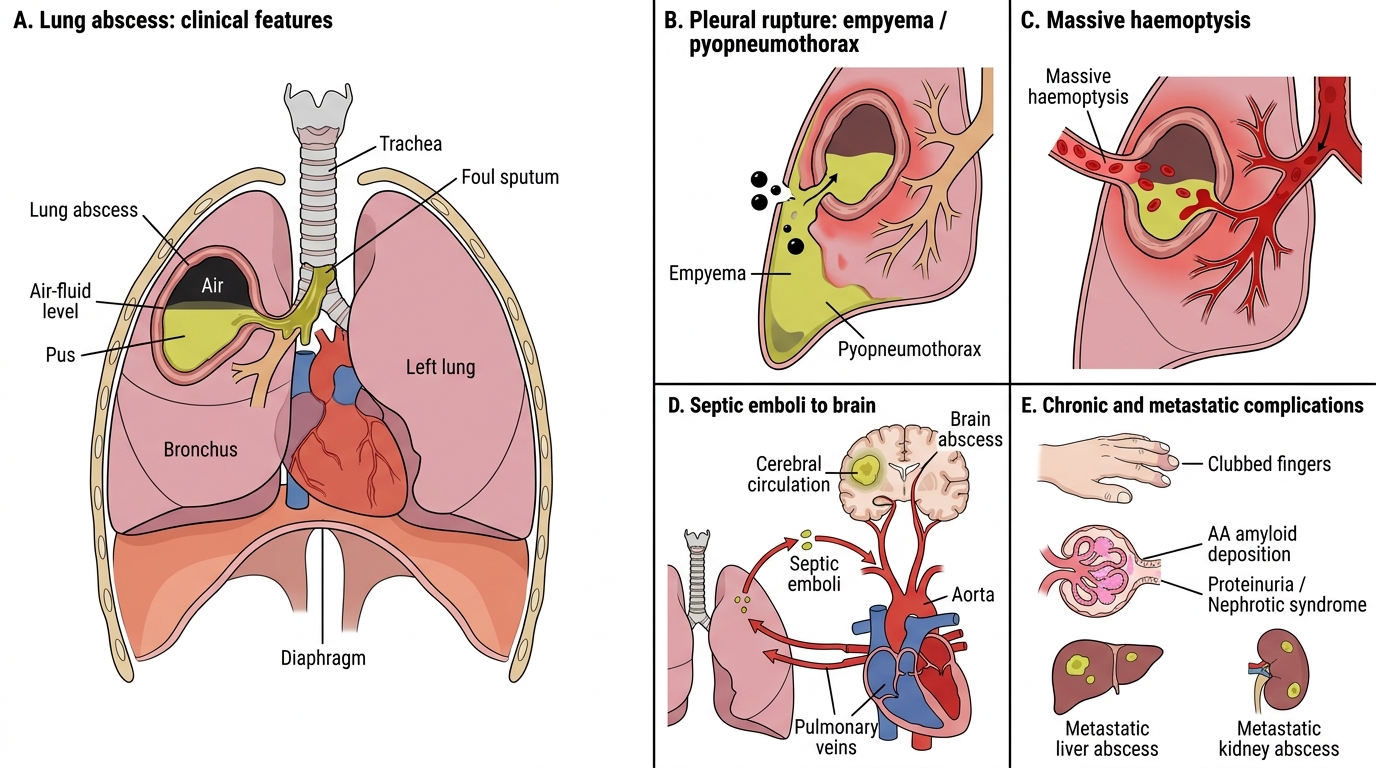
Complications
1. Rupture into pleural space → empyema or pyopneumothorax: pus tracks across the visceral pleura. Pyopneumothorax (pus + air in pleural space) when the abscess communicates with both pleura and bronchus simultaneously. Medical emergency.
2. Massive haemoptysis: erosion of a pulmonary artery branch by the abscess wall. Can be fatal.
3. Haematogenous spread → brain abscess: septic emboli travel via pulmonary veins → left heart → cerebral circulation. Right temporal/parietal lobe most common site (middle cerebral artery territory). Presents with focal neurological signs weeks after the chest diagnosis.
4. Metastatic abscesses: liver, kidneys (haematogenous seeding).
5. Secondary amyloidosis (AA amyloidosis): chronic suppurative infection → sustained IL-6/IL-1 → hepatic synthesis of serum amyloid A protein → AA amyloid deposits in kidneys, spleen, liver. Presents as proteinuria/nephrotic syndrome in a patient with a months-long history of lung abscess.
6. Empyema without rupture: direct extension through the pleural surfaces.
7. Clubbing of the fingers: occurs with chronic lung abscess; mechanism involves platelet-derived growth factor (PDGF) and megakaryocyte fragment deposition in peripheral capillaries.
Clinical features
- Cough (initially dry → later productive)
- Foul-smelling (putrid) sputum: virtually diagnostic of anaerobic infection; patient often notices the sputum stains the pillow overnight (positional drainage of the cavity during sleep).
- Fever (high, swinging, septic pattern)
- Pleuritic chest pain (if pleura involved)
- Haemoptysis (streaky → massive)
- Constitutional symptoms: weight loss, anaemia (chronic disease), digital clubbing
- Chest signs: dullness ± amphoric/cavernous breath sounds over the cavity; post-tussive crackles.
CLINICAL PEARL
Foul sputum = anaerobes = aspiration: whenever a patient has foul or putrid-smelling sputum, the pathogen is almost certainly anaerobic, and the mechanism is almost certainly aspiration. Ask about risk factors: alcoholism, seizures, stroke, dental disease, oesophageal motility disorders. The radiological location will confirm it — posterior segment right upper lobe (supine) or basal segments right lower lobe (upright). This is a classic exam trigger: if the clinical vignette mentions foul sputum + right-sided upper/lower lobe lesion + risk factor for aspiration → the answer is almost always aspiration lung abscess with anaerobes.