Page 9 of 32
PA25.4 | Pulmonary Tuberculosis — SDL Guide
Learning Objectives
- Describe the etiology and transmission of Mycobacterium tuberculosis
- Explain the pathogenesis of TB through Type IV hypersensitivity and cell-mediated immunity
- Distinguish primary (Ghon complex) from secondary/post-primary TB in terms of lesion site, host immunity, and outcome
- Describe the morphological features of the caseating granuloma including Langhans giant cells and ZN-stained AFB
- Outline the progression routes of TB — miliary spread, cavitation, bronchopneumonia, and systemic dissemination
- List the major complications of pulmonary TB including haemoptysis, empyema, amyloidosis, and cor pulmonale
- State the diagnostic modalities: sputum AFB smear, culture, GeneXpert/CBNAAT, Mantoux, and chest imaging
- Briefly explain drug resistance — MDR-TB and XDR-TB
INSTRUCTIONS
Tuberculosis is the world's leading cause of death from a single infectious agent and India carries approximately one-quarter of the global TB burden. Understanding its pathology — from the first Ghon focus to miliary seeding — is essential for every clinician. This module traces the disease from inhaled bacillus to granuloma to cavity, integrating the cell biology you learned in general pathology with the systemic consequences you will encounter on wards.
References
- Robbins & Kumar Basic Pathology, 11th ed., Ch 15 — Lung (textbook)
- Harsh Mohan Textbook of Pathology, 8th ed., Ch 17 — Lungs (textbook)
- WHO Global Tuberculosis Report 2023 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 22-year-old engineering student presents with a 6-week history of low-grade evening fever, drenching night sweats, and a productive cough with occasional blood-streaks. His weight has dropped 6 kg. Chest X-ray reveals a right upper-lobe cavity with surrounding infiltrates and ipsilateral hilar prominence. Sputum smear shows acid-fast bacilli. He has no prior TB history and is HIV-negative.
Before you manage this man you need to answer: Why the apex? Why a cavity? Why haemoptysis? This module gives you those answers — from the first inhaled bacillus to the caseating lung destroyed by its own immune response.
WHY THIS MATTERS
India notified 2.8 million TB cases in 2023 — every physician here will encounter active TB within the first year of practice. PA25.4 is examined in every university and postgraduate entrance. More importantly, recognising the pathological stage of TB (primary vs secondary, latent vs active, cavity vs miliary) determines management — including whether to suspect drug resistance.
RECALL
Before we start, activate what you already know:
- From General Pathology — describe a granuloma: what cells form it, and how does it differ from acute inflammation?
- From Microbiology — which stain identifies Mycobacterium tuberculosis in tissue and sputum? Why does the organism need a special stain?
- From Physiology — why is the lung apex more susceptible to reactivation TB? (Hint: think ventilation-perfusion ratio and oxygen tension.)
Hold these ideas in mind — they will return throughout the module.
The Organism and Transmission
Tuberculosis: Organism, Transmission, and Granuloma Formation
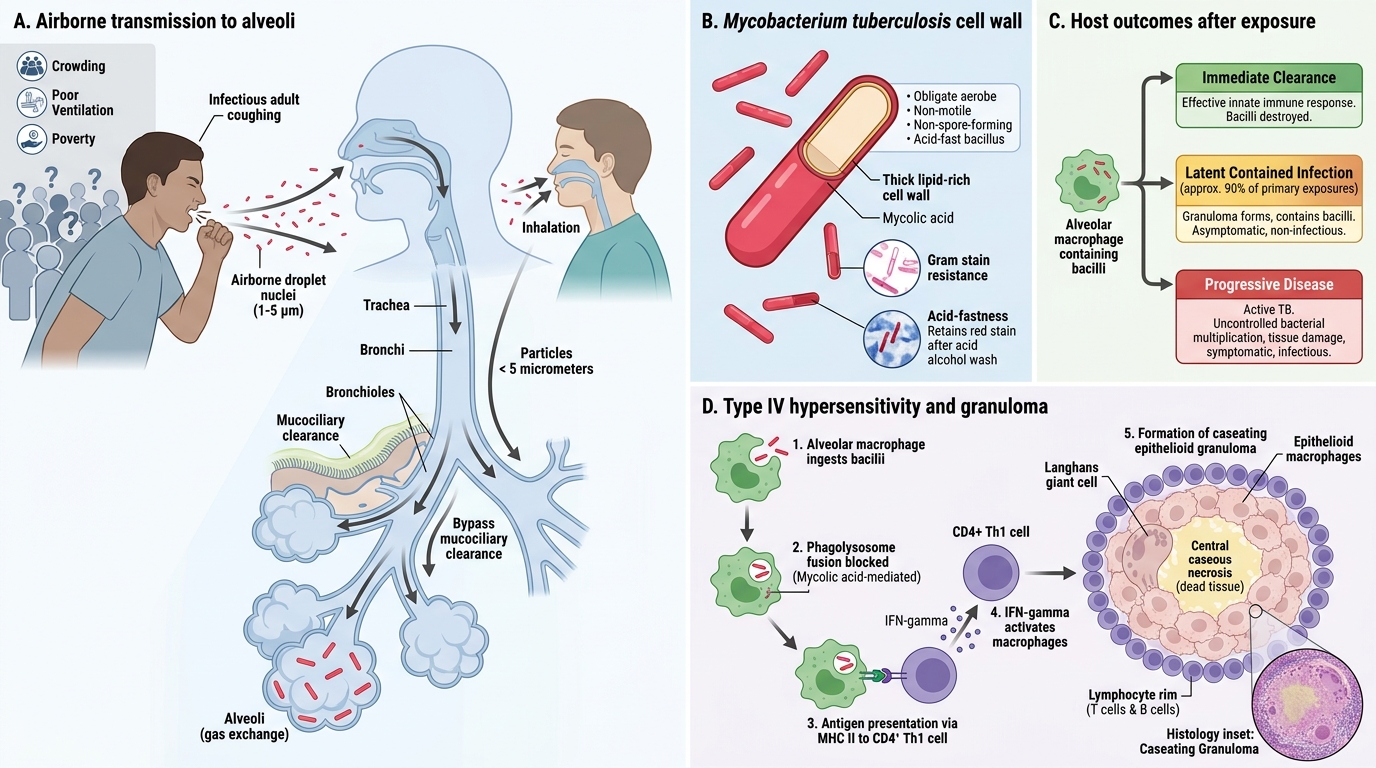
Mycobacterium tuberculosis is an obligate aerobe, non-motile, non-spore-forming acid-fast bacillus (AFB). Its thick, lipid-rich cell wall (containing mycolic acid) is responsible for acid-fastness, resistance to Gram stain, and resistance to phagocytic killing — the cornerstone of its pathogenicity.
Transmission is almost exclusively via inhalation of infectious droplet nuclei (1–5 µm, produced by coughing, sneezing, or speaking). A single cough can aerosolise thousands of particles; droplet nuclei <5 µm bypass mucociliary clearance and reach alveoli directly. Crowded housing, poor ventilation, and poverty drive India's TB burden.
Key concept: although TB is classically "the great imitator" at clinical level, at pathological level it almost always produces one signature lesion — the caseating epithelioid granuloma.
Pathogenesis: Type IV Hypersensitivity and the Granuloma
Type IV Hypersensitivity and Caseating Granuloma in Tuberculosis
Once bacilli reach alveolar macrophages, three possible fates exist: (1) immediate clearance in immunocompetent hosts, (2) contained latent infection (90% of primary exposures), or (3) progressive disease.
Cell-mediated immunity (CMI) is the primary defence. The sequence:
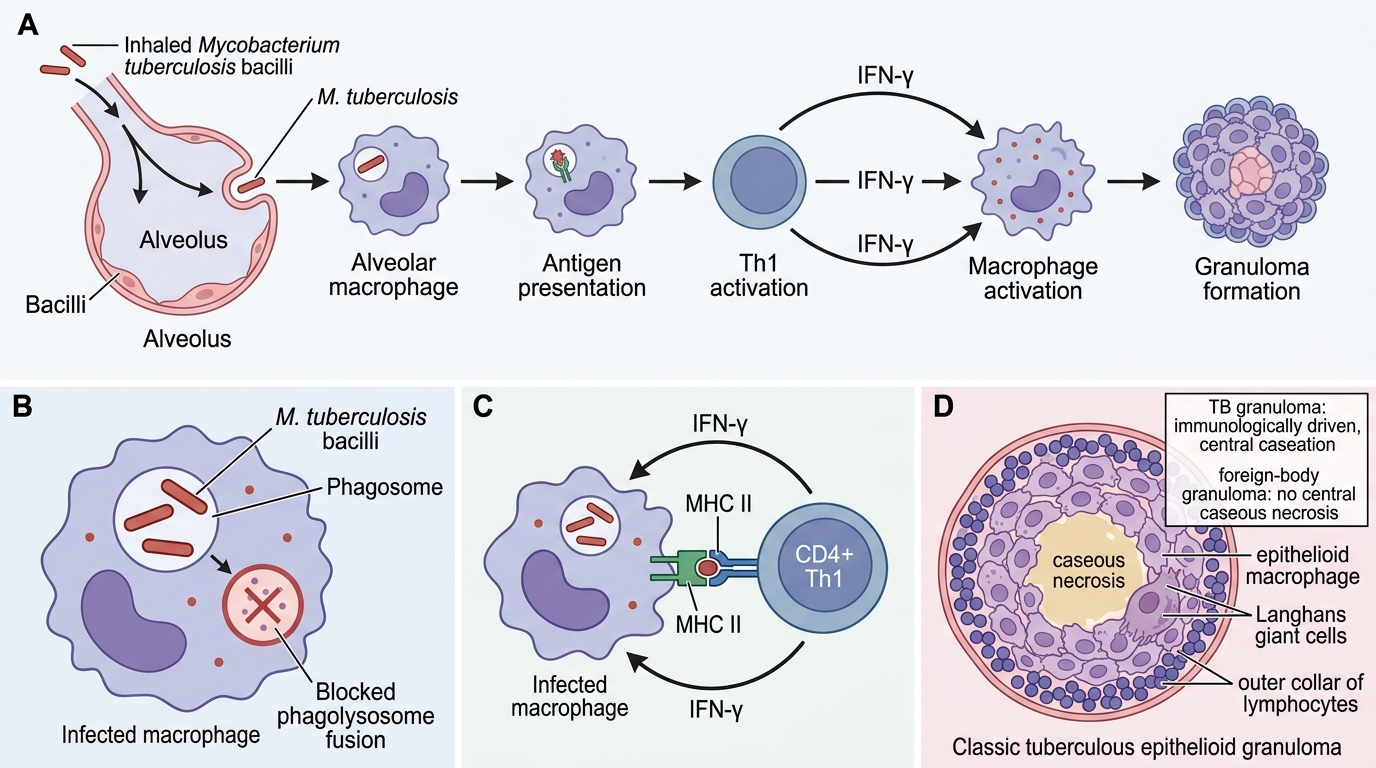
- Alveolar macrophages ingest bacilli → fail to kill due to mycolic acid blocking phagolysosome fusion.
- Infected macrophages present antigen via MHC II → activate CD4+ Th1 lymphocytes.
- Th1 cells secrete IFN-γ → activates macrophages to produce reactive oxygen species and nitric oxide → partial bacillary killing.
- Activated macrophages differentiate into epithelioid cells and fuse to form Langhans giant cells.
- A collar of lymphocytes surrounds the epithelioid centre → classic epithelioid granuloma.
- Type IV (delayed-type) hypersensitivity mediates central necrosis → caseous necrosis (cheese-like, acellular, homogeneous eosinophilic material).
The granuloma is protective (walls off bacilli) but also destructive (caseation destroys normal tissue). This dual role explains nearly every complication of TB.
IMPORTANT: The granuloma in TB is NOT the same as a foreign-body granuloma — it is immunologically driven and centrally necrotic. (Cross-reference your General Pathology notes on granulomatous inflammation.)
SELF-CHECK
A macrophage infected with M. tuberculosis fails to kill the bacillus despite phagocytosis. Which virulence mechanism is most responsible?
A. Production of IgA protease that cleaves mucosal antibodies
B. Capsular polysaccharide preventing complement activation
C. Mycolic acid-rich cell wall blocking phagolysosome fusion
D. Exotoxin that lyses macrophage membranes before phagosome formation
Reveal Answer
Answer: C. Mycolic acid-rich cell wall blocking phagolysosome fusion
M. tuberculosis survives inside macrophages primarily because its mycolic acid-rich cell wall prevents fusion of the phagosome with the lysosome, blocking acidification and enzymatic killing. This is distinct from organisms like Staphylococcus (which produce leukocidins) or encapsulated bacteria (which resist opsonisation).
Primary Tuberculosis and the Ghon Complex
Primary Tuberculosis and the Ghon Complex
Primary TB occurs in individuals without prior sensitisation — most commonly children and young adults encountering TB for the first time.
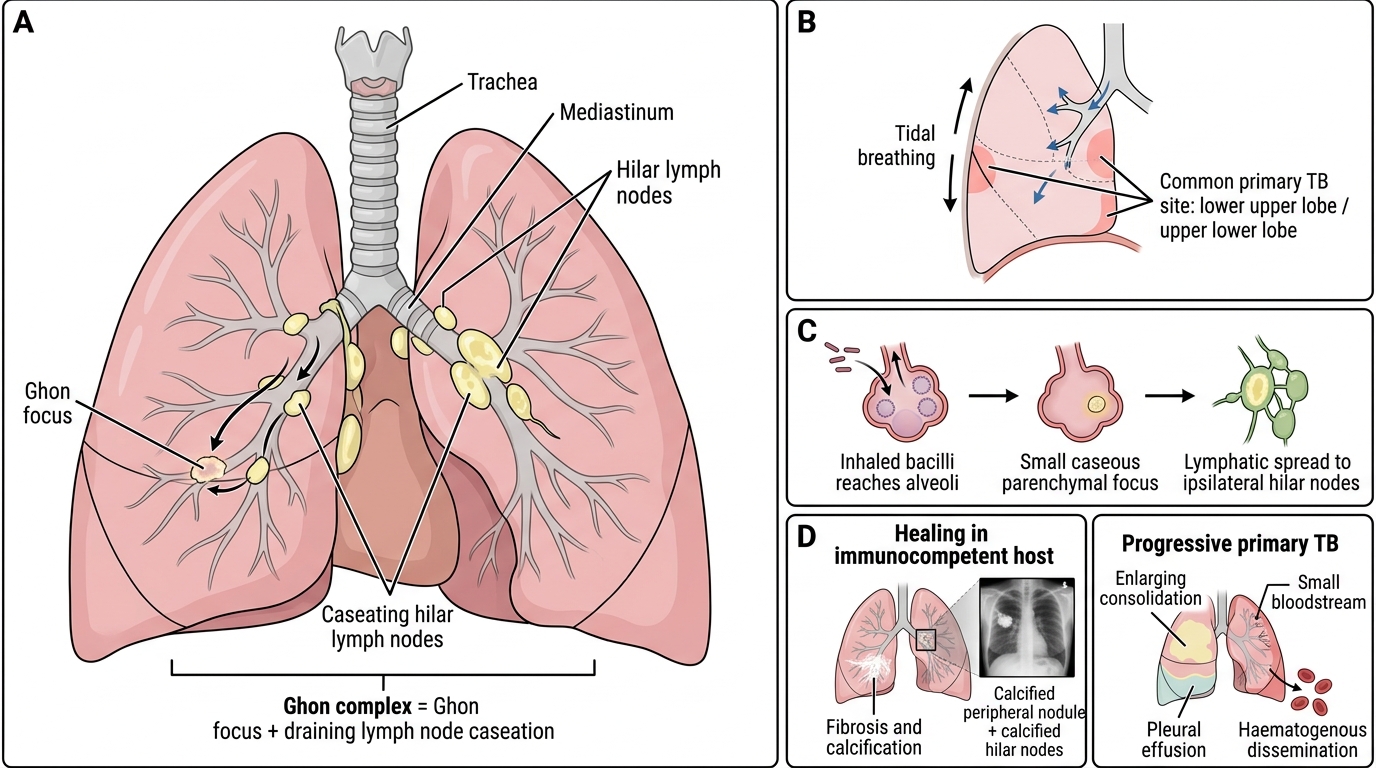
Ghon focus: the initial parenchymal lesion, typically a small (1–2 cm) subpleural area of caseous consolidation in the lower part of the upper lobe or upper part of the lower lobe (areas of highest airflow during tidal breathing). Haematogenous or lymphatic spread from the Ghon focus reaches the ipsilateral hilar/mediastinal lymph nodes → they too undergo caseation.
Ghon complex = Ghon focus + draining lymph node caseation (the primary complex of Ranke).
IMPORTANT: The lymph node component is characteristically larger than the parenchymal focus in children — this distinguishes primary from secondary TB radiologically.
Usual fate (immunocompetent): healing with progressive fibrosis and calcification (Ghon lesion on plain X-ray as a calcified peripheral nodule + calcified hilar nodes). The bacilli are walled off in a granuloma but may remain viable for decades → latent TB infection (LTBI).
Progressive primary TB (immunocompromised — HIV, malnutrition, infants): the primary focus enlarges without containment → lobar consolidation, pleural effusion, haematogenous dissemination. In infants, primary TB itself can be rapidly fatal.
IMPORTANT IMAGE BELOW — GHON COMPLEX ANATOMY:
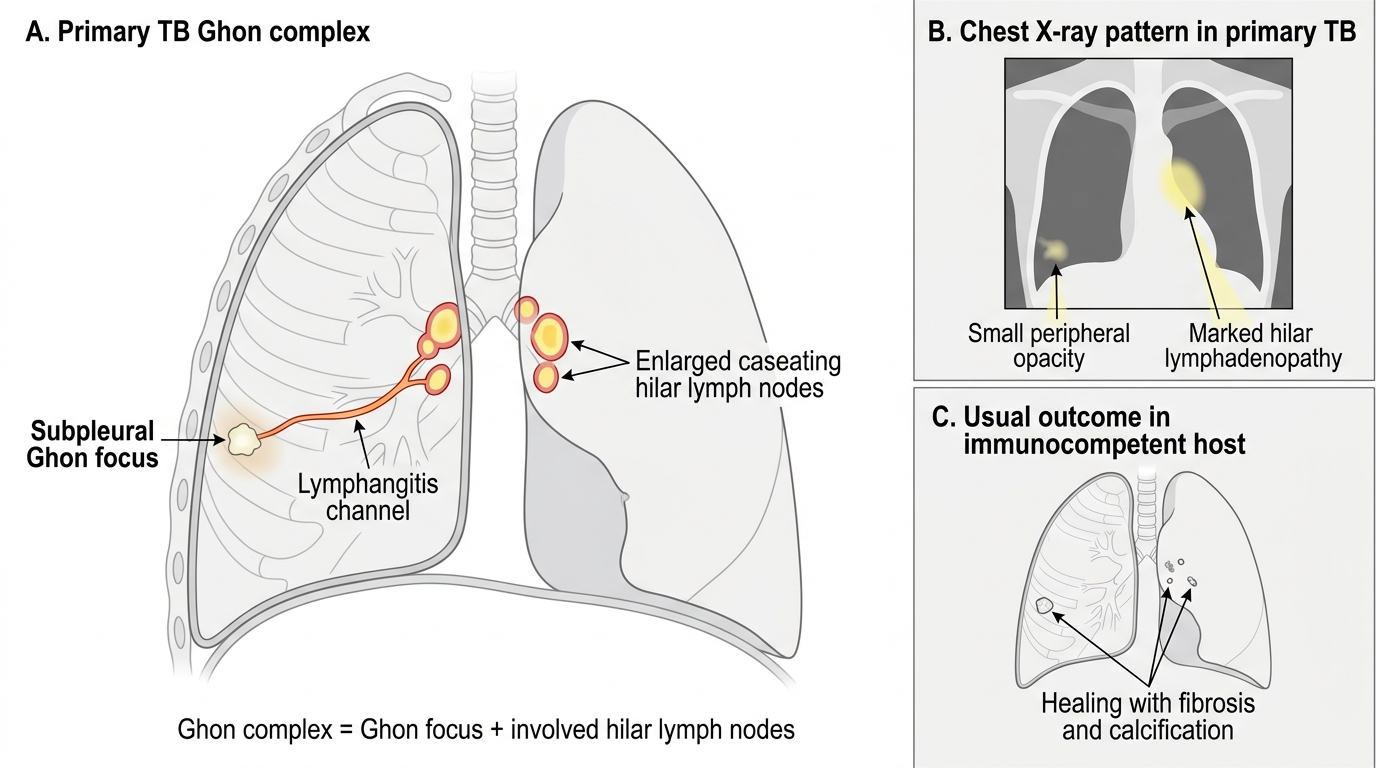
Primary TB Ghon Complex
SELF-CHECK
In a 7-year-old child with primary TB, the chest X-ray shows a small peripheral opacity in the right lower zone and a markedly enlarged right hilar shadow. What does this combination represent?
A. Ghon complex — subpleural Ghon focus with reactive hilar lymphadenopathy
B. Secondary TB with apical cavitation
C. Tuberculous bronchopneumonia — acinar spread via the bronchial tree
D. Miliary TB with haematogenous seeding of both lungs
Reveal Answer
Answer: A. Ghon complex — subpleural Ghon focus with reactive hilar lymphadenopathy
The Ghon complex (= Ghon focus + hilar node involvement) is the hallmark of primary TB. The lymph node enlargement is typically disproportionately large relative to the parenchymal focus in children. Secondary TB is a reactivation disease affecting the apices. Miliary TB produces bilateral millet-seed nodules throughout both lungs.