Page 10 of 32
PA25.4 | Pulmonary Tuberculosis — SDL Guide (Part 2)
Secondary (Post-Primary / Reactivation) Tuberculosis
Secondary Tuberculosis: Reactivation Pattern
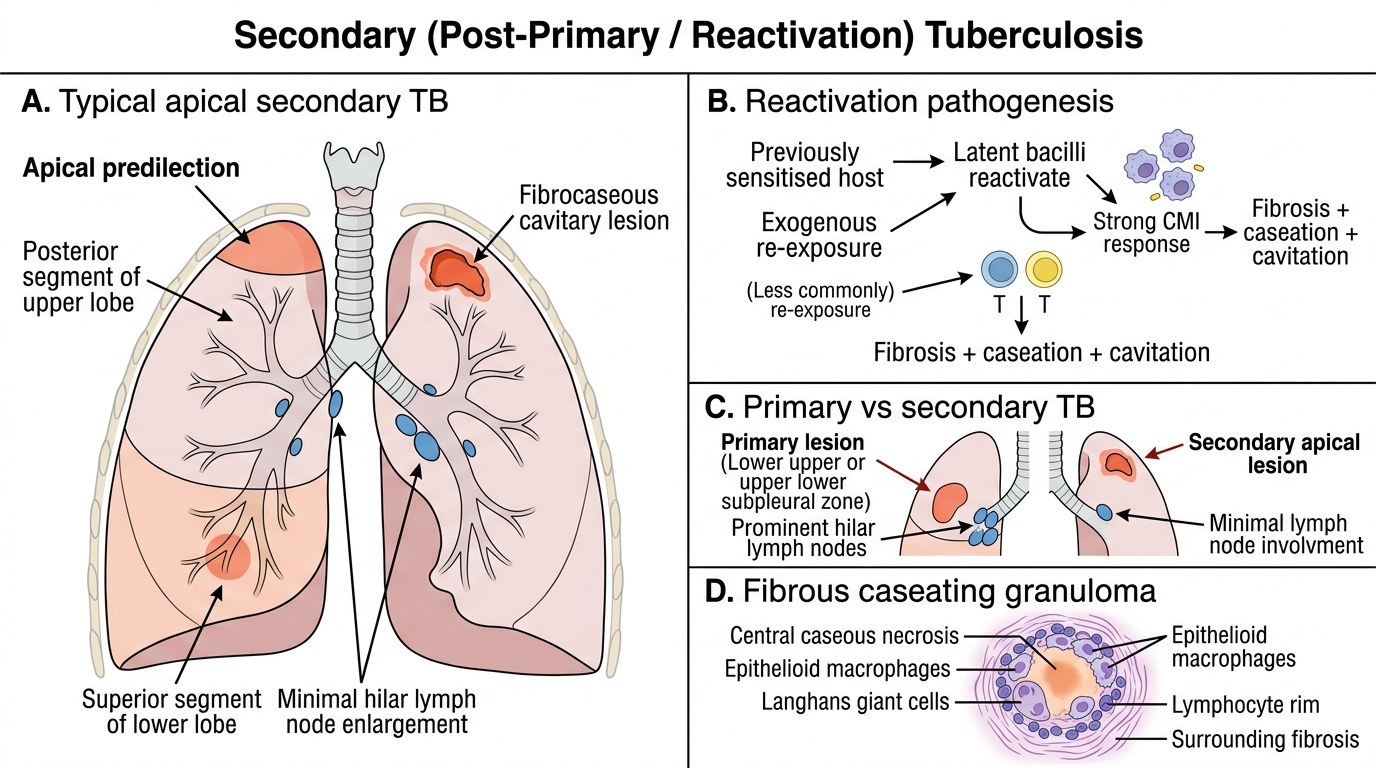
Secondary TB arises in previously sensitised individuals — either from reactivation of latent bacilli (endogenous reinfection) or, less commonly, exogenous re-exposure. Because the host now has established CMI, the disease behaves differently from primary TB:
| Feature | Primary TB | Secondary TB |
|---|---|---|
| Sensitisation | None (first exposure) | Present (prior exposure) |
| Site of parenchymal lesion | Lower upper / upper lower zone (subpleural) | Apex (posterior segment of upper lobe, or superior segment of lower lobe) |
| Lymph node involvement | Prominent | Minimal |
| Granuloma quality | Florid, with caseation | More fibrous, harder containment of reactivation |
| Cavitation | Rare | Common (hallmark) |
| Haematogenous spread | Absent (contained) | Possible (miliary TB) |
Why the apex in secondary TB? Apical zones have the highest V/Q ratio and therefore the highest O₂ tension — optimal for the obligate aerobe M. tuberculosis. Bacterial load in reactivation bypasses the lymph-node filtering seen in primary disease.
Apical cavitation: cascading granulomas coalesce → large area of caseation → liquefaction (proteases from activated macrophages) → softened caseum drains via connecting bronchi → cavity with a thin fibrous wall, surrounding fibrous scar, and ongoing seeding of bacilli into the bronchial tree.
IMPORTANT IMAGE BELOW — PRIMARY VS SECONDARY TB:
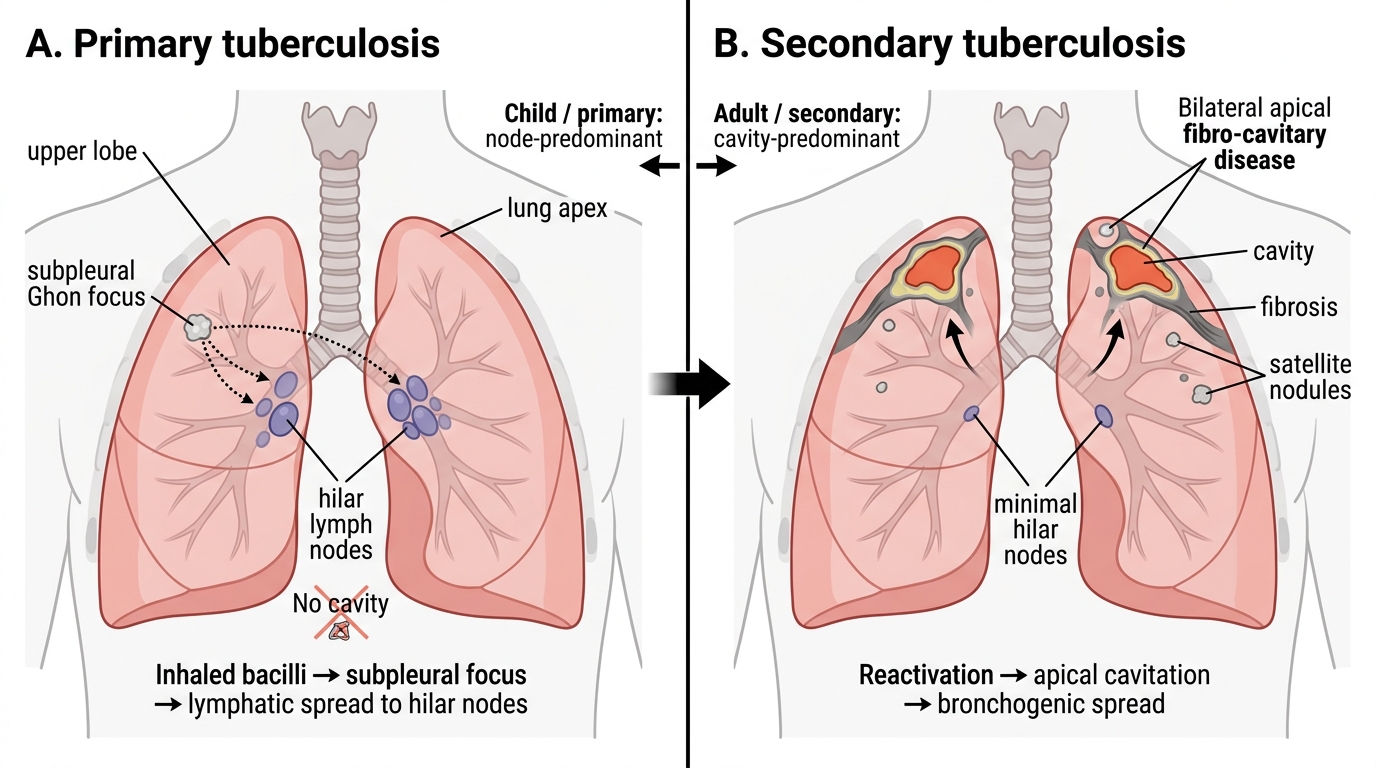
Primary vs Secondary Pulmonary Tuberculosis
CLINICAL PEARL
The apex rule in practice: When you see a chest X-ray with unilateral or bilateral upper-zone opacities, haziness, or cavity — think secondary TB first. The classic description is "fibro-cavitary disease in the apices with adjacent satellite nodules." A lower-zone opacity in a child with hilar prominence is primary TB until proved otherwise. These patterns are tested in every MBBS and MD entrance exam — and more importantly, they determine whether you are dealing with a child (lymph node–predominant) or adult (cavity–predominant) presentation with very different implications for drug resistance and contact-tracing.
Morphology — Gross and Microscopic Appearances
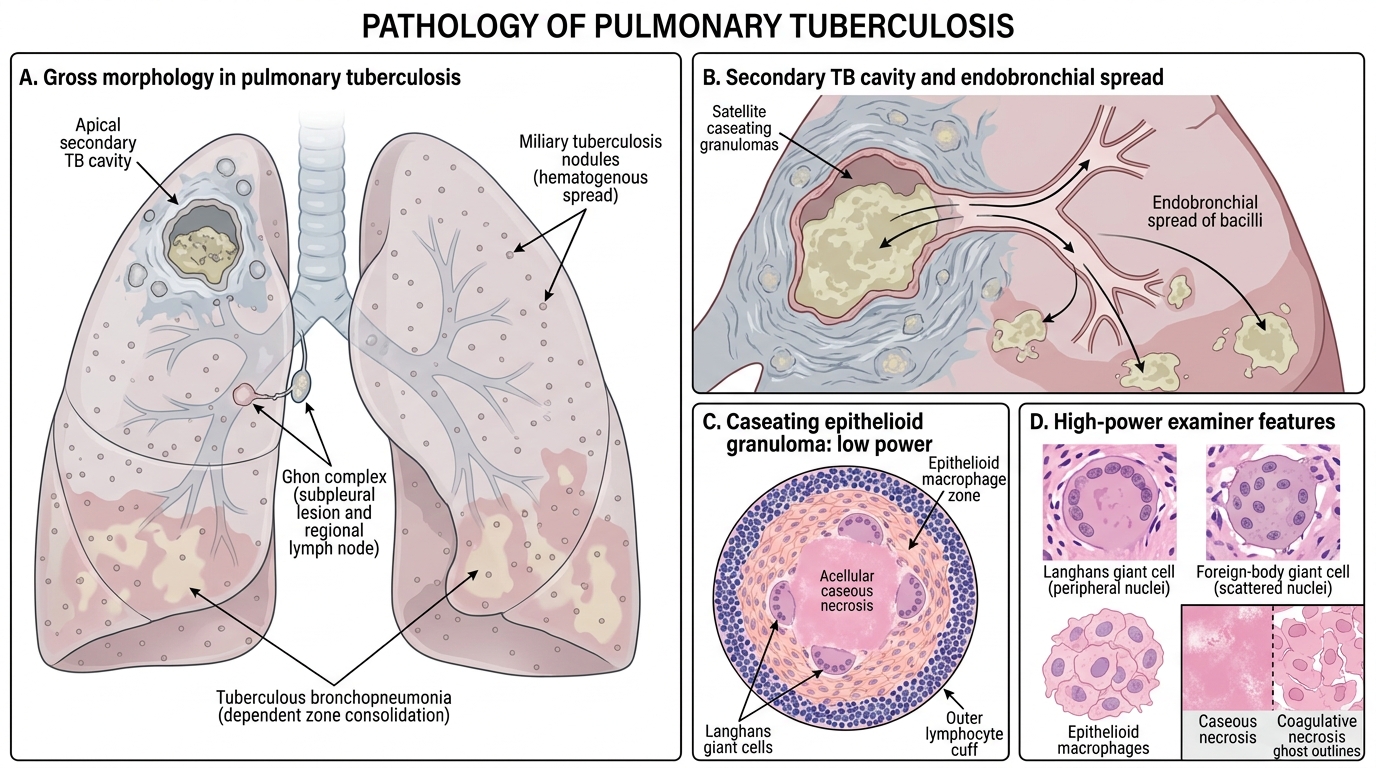
Pulmonary Tuberculosis: Gross and Microscopic Morphology
Gross morphology:
- Ghon lesion: small, firm, grey-white subpleural nodule, often calcified on cut section in healed cases.
- Secondary TB cavity: irregular-walled cavity, up to several centimetres, inner wall coated with grey-yellow caseous material; surrounding lung shows old fibrosis and new satellite granulomas.
- Miliary nodules: 1–2 mm millet-seed (Latin: milium) yellow-white nodules scattered throughout the lung — individually they represent discrete caseating granulomas seeded by haematogenous spread.
- Tuberculous bronchopneumonia: confluent patchy consolidation, multiple caseous foci in dependent zones — results from endobronchial spread of bacilli from a cavity.
Microscopic morphology (THE examiner favourite):
The hallmark lesion is the caseating epithelioid granuloma, composed of:
1. Central caseous necrosis — acellular, finely granular eosinophilic material; no preserved tissue architecture (contrast with coagulative necrosis where ghost outlines persist).
2. Surrounding epithelioid macrophages — activated macrophages with abundant pale pink cytoplasm and oval, vesicular nuclei; arranged in a sheet around the caseous core.
3. Langhans giant cells — multinucleate giant cells (up to 40+ nuclei) with nuclei arranged in a horseshoe or peripheral arc at the cell periphery. Distinguish from foreign-body giant cells (nuclei scattered randomly throughout cytoplasm).
4. Outer lymphocyte cuff — CD4+ T-lymphocytes (and some CD8+) forming the immunological barrier.
5. Peripheral fibrous capsule — proportional to lesion age; older granulomas are more densely fibrous.
IMPORTANT IMAGE BELOW — MICROSCOPY:
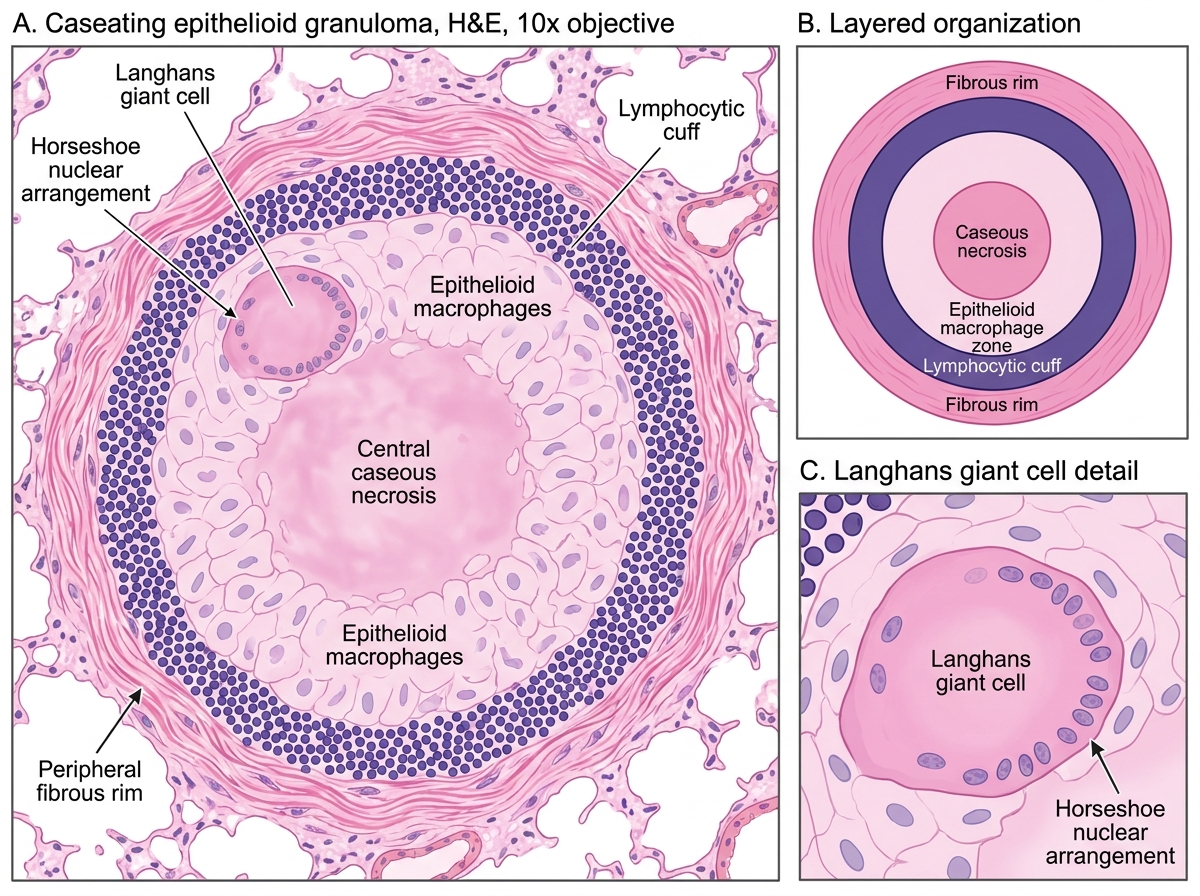
Caseating Epithelioid Granuloma in Secondary Tuberculosis
Ziehl-Neelsen (ZN) stain: AFB appear as beaded red rods on a blue background. Bacilli are present in small numbers — diligent search or concentration is needed. High bacterial load (positive ZN smear) indicates active, progressive disease.
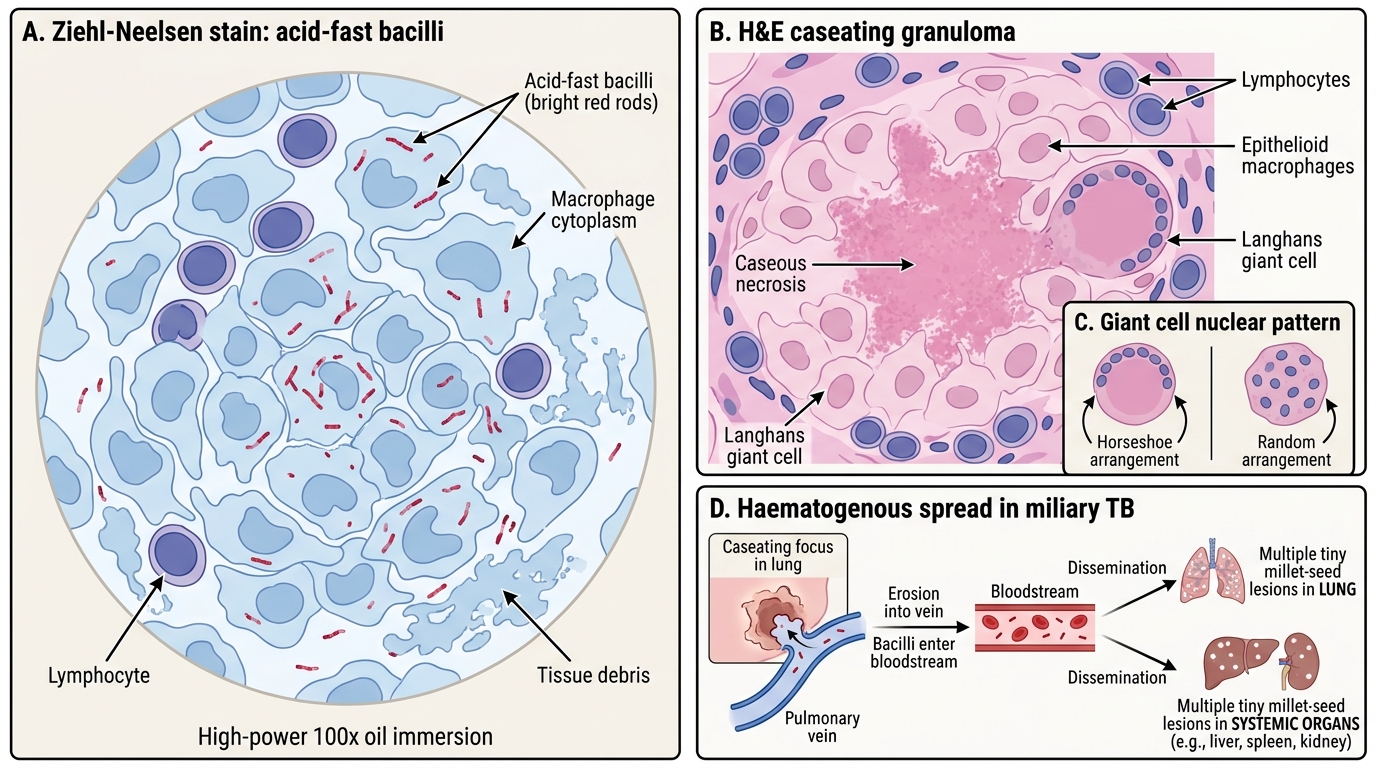
Tuberculosis: Acid-Fast Bacilli, Caseating Granuloma, and Miliary Spread
SELF-CHECK
On H&E staining of a lung biopsy, you observe multinucleate giant cells with nuclei arranged in a peripheral horseshoe pattern, surrounding central structureless eosinophilic material. What is the most likely diagnosis?
A. Fungal granuloma (e.g., Histoplasma) — foreign body-type giant cells
B. Sarcoidosis — non-caseating granuloma with asteroid/Schaumann bodies
C. Rheumatoid nodule — palisading macrophages around fibrinoid necrosis
D. Caseating epithelioid granuloma consistent with tuberculosis — Langhans giant cells
Reveal Answer
Answer: D. Caseating epithelioid granuloma consistent with tuberculosis — Langhans giant cells
The horseshoe (peripheral arc) arrangement of nuclei is the defining feature of Langhans giant cells — not to be confused with foreign-body giant cells (random nuclear distribution) or sarcoid giant cells (Schaumann/asteroid bodies, non-caseating). The central 'structureless eosinophilic material' is caseous necrosis — no ghost outlines, no viable cells, which distinguishes it from coagulative necrosis.
Miliary Tuberculosis and Haematogenous Spread
Miliary Tuberculosis and Haematogenous Spread
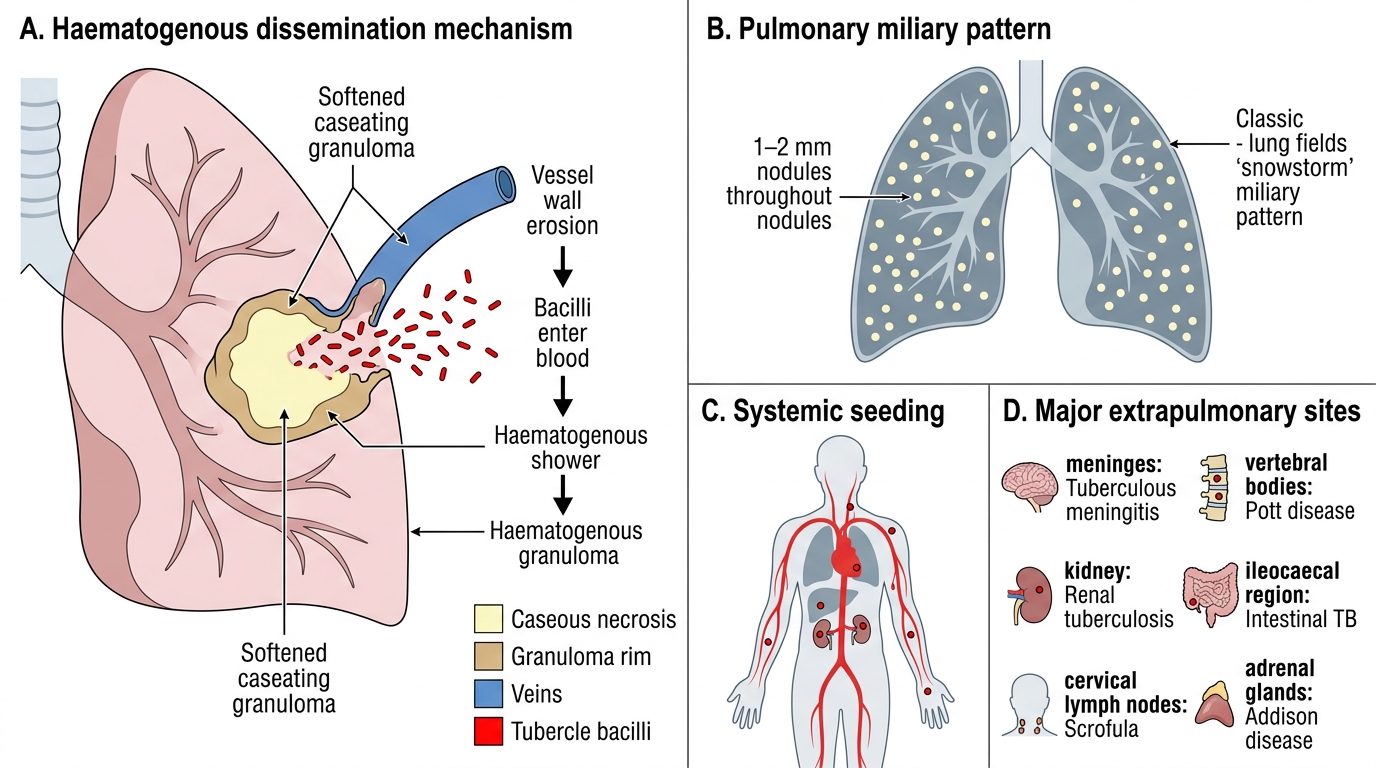
Miliary TB is the consequence of massive haematogenous dissemination — when caseation erodes into a pulmonary vein (or, less commonly, the thoracic duct), releasing a shower of bacilli into the systemic or pulmonary circulation.
Mechanism: Caseous material from a softened granuloma → erodes vessel wall → bacilli enter blood → seed every organ simultaneously.
Pulmonary miliary pattern: Bilateral, symmetrical, uniformly sized (1–2 mm) nodules throughout both lung fields on chest X-ray — the classic "snowstorm" pattern. Each nodule is a tiny caseating granuloma at haematogenous implantation site.
Systemic miliary spread reaches:
• Meninges → tuberculous meningitis (commonest cause of TBM in India; CSF: lymphocytic pleocytosis, low glucose, high protein, cobweb clot)
• Spine (vertebral bodies) → Pott disease (TB spondylitis; L1–L4 most common; vertebral collapse → angular kyphosis = "gibbus")
• Kidneys → renal TB (sterile pyuria, haematuria; "putty kidney" calcification)
• Intestines → ileocaecal TB (swallowed sputum; "napkin-ring" stricture)
• Lymph nodes → TB lymphadenitis (commonest extrapulmonary TB in India; cervical nodes most often; "collar-stud abscess" through deep cervical fascia)
• Adrenals → Addison disease (bilateral adrenal destruction)
IMPORTANT IMAGE BELOW — MILIARY TB:
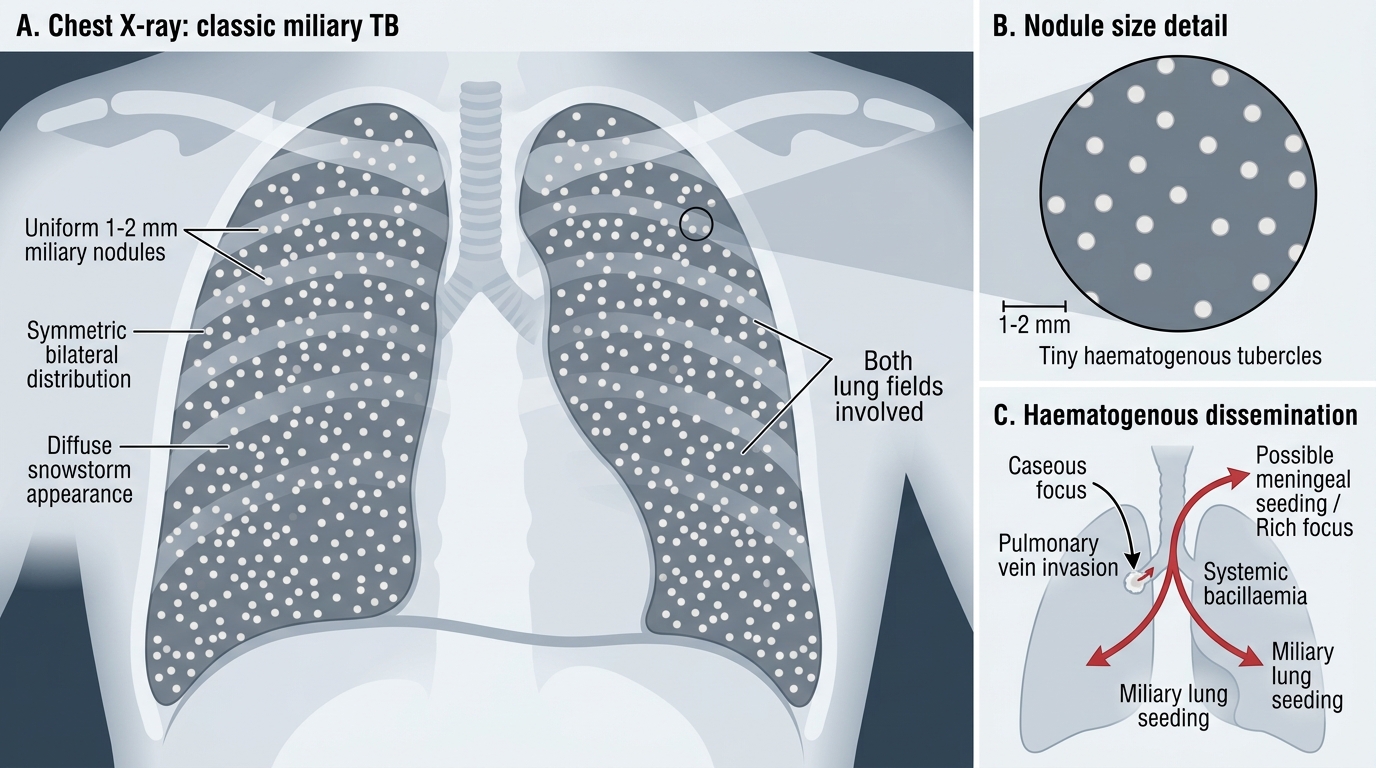
Classic Miliary Tuberculosis on Chest X-ray
SELF-CHECK
A 35-year-old man with known pulmonary TB on treatment develops sudden onset confusion, neck stiffness, and photophobia. CSF analysis shows lymphocytic pleocytosis, glucose 30 mg/dL (serum 90 mg/dL), protein 180 mg/dL, and a cobweb clot. What is the route by which TB reached the meninges?
A. Lymphatic permeation via the thoracic duct to the cisterna magna
B. Aspiration of infected sputum directly through the cribriform plate
C. Direct extension from adjacent Pott disease vertebral osteomyelitis
D. Haematogenous dissemination from caseous erosion into a pulmonary vein
Reveal Answer
Answer: D. Haematogenous dissemination from caseous erosion into a pulmonary vein
Tuberculous meningitis results from haematogenous spread — either in the miliary phase (systemic bacillaemia) or from rupture of a small cortical or meningeal granuloma (Rich focus) into the subarachnoid space. The CSF picture described (lymphocytosis, very low glucose, high protein, cobweb clot on standing) is classic for TBM. Direct extension from Pott disease is a rare, localised mechanism, not the commonest route.