Page 11 of 32
PA25.4 | Pulmonary Tuberculosis — SDL Guide (Part 3)
Complications of Pulmonary Tuberculosis
Complications of Pulmonary Tuberculosis
Understanding complications is examining priority and clinical reality:
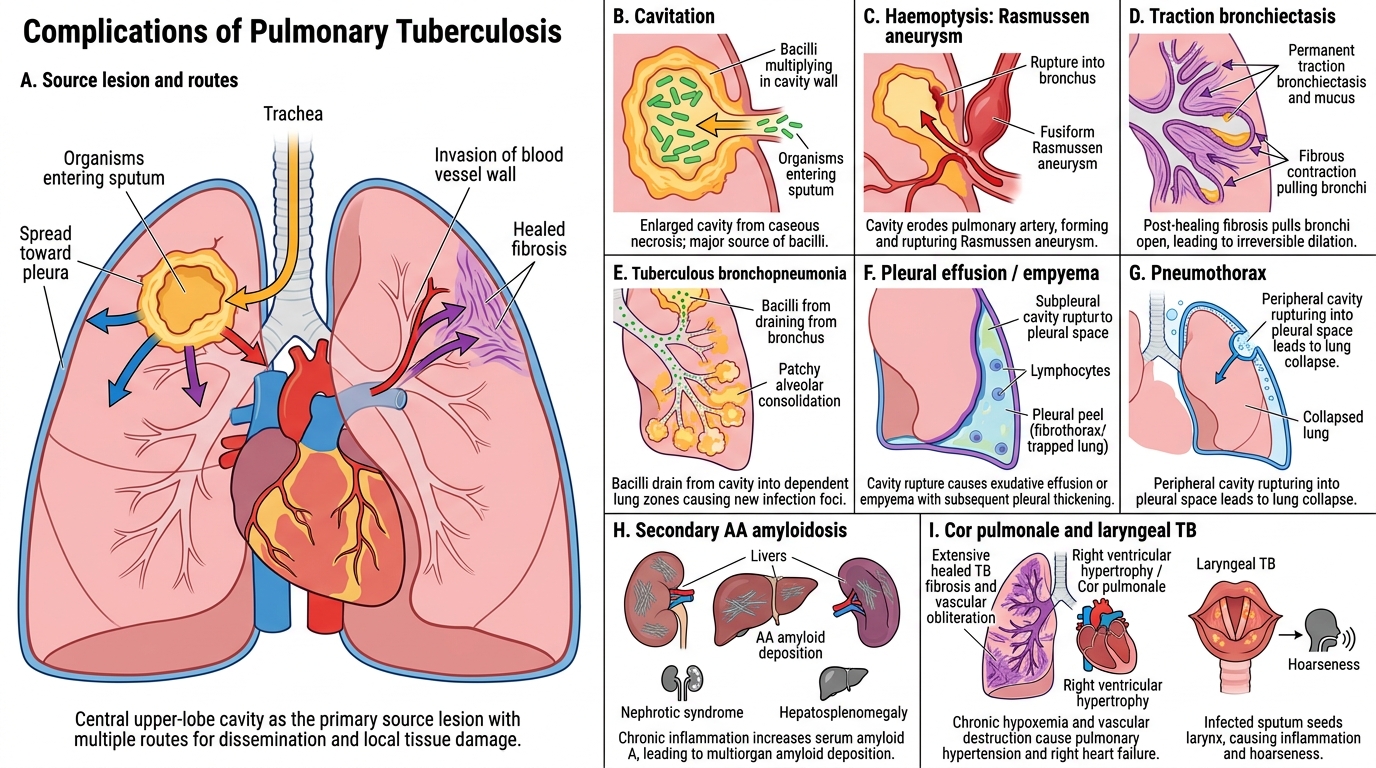
Local / pulmonary complications:
- Cavitation — ongoing cavity enlargement with failure to heal; bacilli multiply in cavity wall and are shed into sputum (high infectivity).
- Haemoptysis — erosion of a branch pulmonary artery in a cavity wall → Rasmussen aneurysm (fusiform dilatation from inflammatory weakening) → rupture → massive haemoptysis (emergency). Minor haemoptysis from granulation tissue.
- Bronchiectasis — fibrous contraction and traction on bronchi after healing → permanent bronchial dilatation → recurrent secondary infections.
- Tuberculous bronchopneumonia — bacilli drain from cavity into bronchi → diffuse alveolar filling in dependent zones; fulminant, high mortality.
- Pleural effusion / empyema — rupture of a subpleural granuloma or cavity into pleural space → tuberculous pleuritis (exudative lymphocytic effusion) → if untreated, empyema → fibrothorax (trapped lung).
- Pneumothorax — rupture of a peripheral cavity into pleural space.
Systemic / remote complications:
- Secondary amyloidosis (AA type) — chronic TB produces sustained high serum amyloid A protein → amyloid deposits in kidney, liver, spleen → nephrotic syndrome, hepatosplenomegaly.
- Cor pulmonale — extensive pulmonary fibrosis and vascular obliteration after healed TB → pulmonary hypertension → right ventricular hypertrophy and eventual failure.
- Laryngeal TB — seeding from infected sputum → hoarseness, dysphonia; highly infectious.
- Intestinal TB — swallowed sputum → ileocaecal involvement → malabsorption, stricture, fistula.
- Renal / adrenal / bone TB (as above — haematogenous).
Memory anchor: "Every TB cavity can bleed (Rasmussen), collapse (pneumothorax), fill with fluid (empyema), or spread (bronchopneumonia). Untreated chronic disease causes amyloid and cor pulmonale."
CLINICAL PEARL
Rasmussen aneurysm — the most dramatic TB complication: When a pulmonary artery branch lies in the wall of a TB cavity, chronic inflammation weakens its muscular wall → pseudoaneurysm formation (Rasmussen aneurysm). Rupture causes sudden, massive haemoptysis — bright red blood in large volumes, often fatal. On HRCT, it appears as an enhancing nodule within a cavity wall. Endovascular bronchial artery embolisation is the emergency treatment. This is examined regularly because it links TB morphology directly to a life-threatening clinical emergency.
Latent TB, Reactivation Triggers, and Drug Resistance
Latent TB, Reactivation, and Drug Resistance
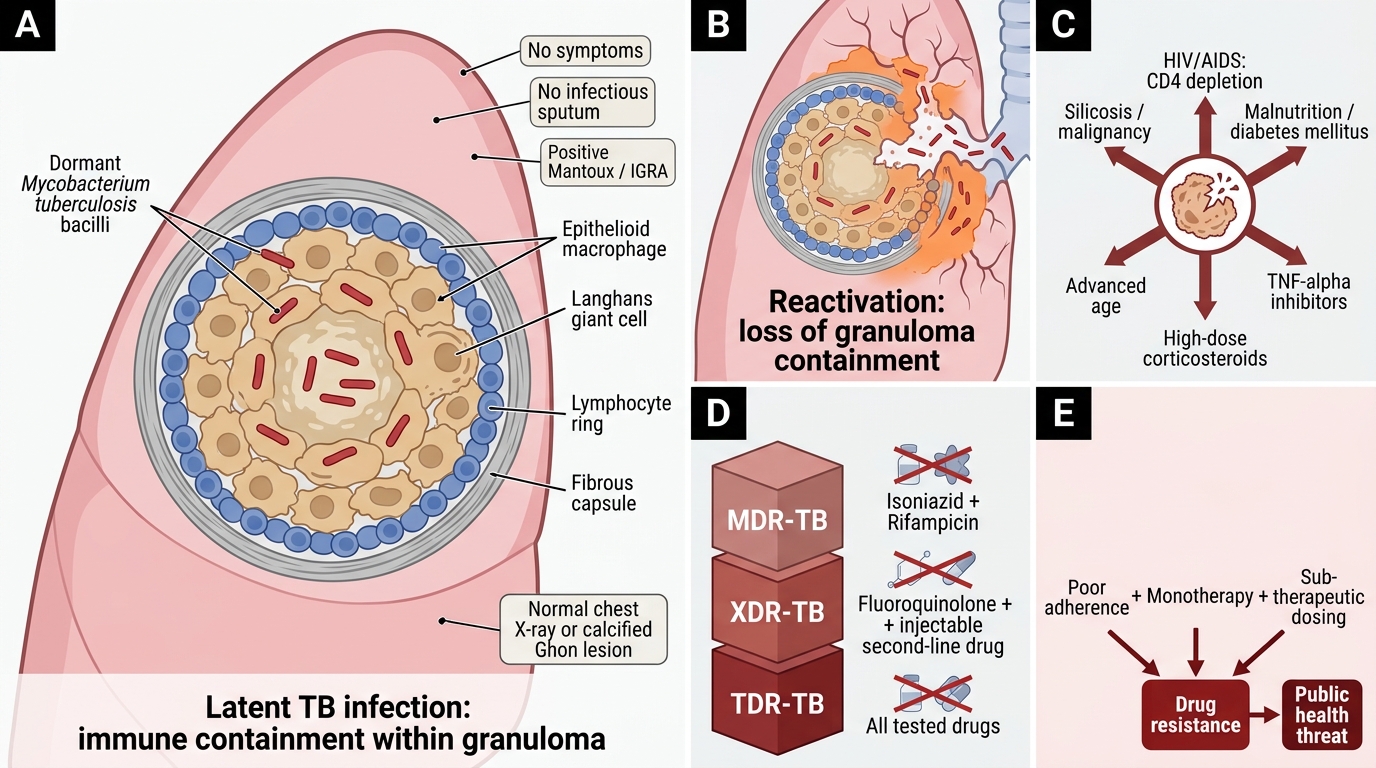
Latent TB infection (LTBI): ~1.8 billion people worldwide harbour viable but dormant M. tuberculosis within granulomas. In LTBI: no symptoms, no infectious sputum, positive Mantoux/IGRA (evidence of prior sensitisation), normal chest X-ray (or only calcified Ghon lesion). Bacilli persist within macrophages in a metabolically slowed state.
Reactivation triggers (break the granuloma's immune containment):
• HIV/AIDS (most powerful — CD4 depletion destroys the immunological scaffold of the granuloma)
• Malnutrition / diabetes mellitus
• TNF-α inhibitors (used in RA, IBD) — block macrophage activation
• High-dose corticosteroids
• Advanced age
• Silicosis (silicotuberculosis)
• Haematological malignancies
Drug-resistant TB:
• MDR-TB (multidrug-resistant): resistant to at least isoniazid + rifampicin (the two most potent first-line drugs).
• XDR-TB (extensively drug-resistant): MDR-TB + resistance to any fluoroquinolone + at least one injectable second-line drug.
• TDR-TB (totally drug-resistant): resistant to all tested drugs — a clinical and public health catastrophe.
• India has among the highest MDR-TB burdens globally. Inadequate treatment (poor adherence, monotherapy, sub-therapeutic dosing) drives resistance.
Diagnosis summary:
| Test | Detects | Notes |
|---|---|---|
| Sputum AFB smear (ZN) | Bacilli in sputum | Fast, cheap; low sensitivity (~50–60%) |
| Sputum culture (LJ/MGIT) | Viable bacilli + DST | Gold standard; 2–8 weeks |
| GeneXpert MTB/RIF (CBNAAT) | MTB DNA + rifampicin resistance | 2 hours; sensitivity ~85–90%; RNTCP/NTEP first-line |
| Mantoux (TST) | Prior sensitisation (CMI) | Positive in latent + active; false-negative in immunosuppressed |
| IGRA (QuantiFERON) | IFN-γ release (CMI) | Preferred in BCG-vaccinated populations |
| HRCT chest | Structural disease | Cavities, miliary, adenopathy, bronchiectasis |
Cavitary TB — Gross Pathology Summary
Cavitary Tuberculosis: Gross Pathology
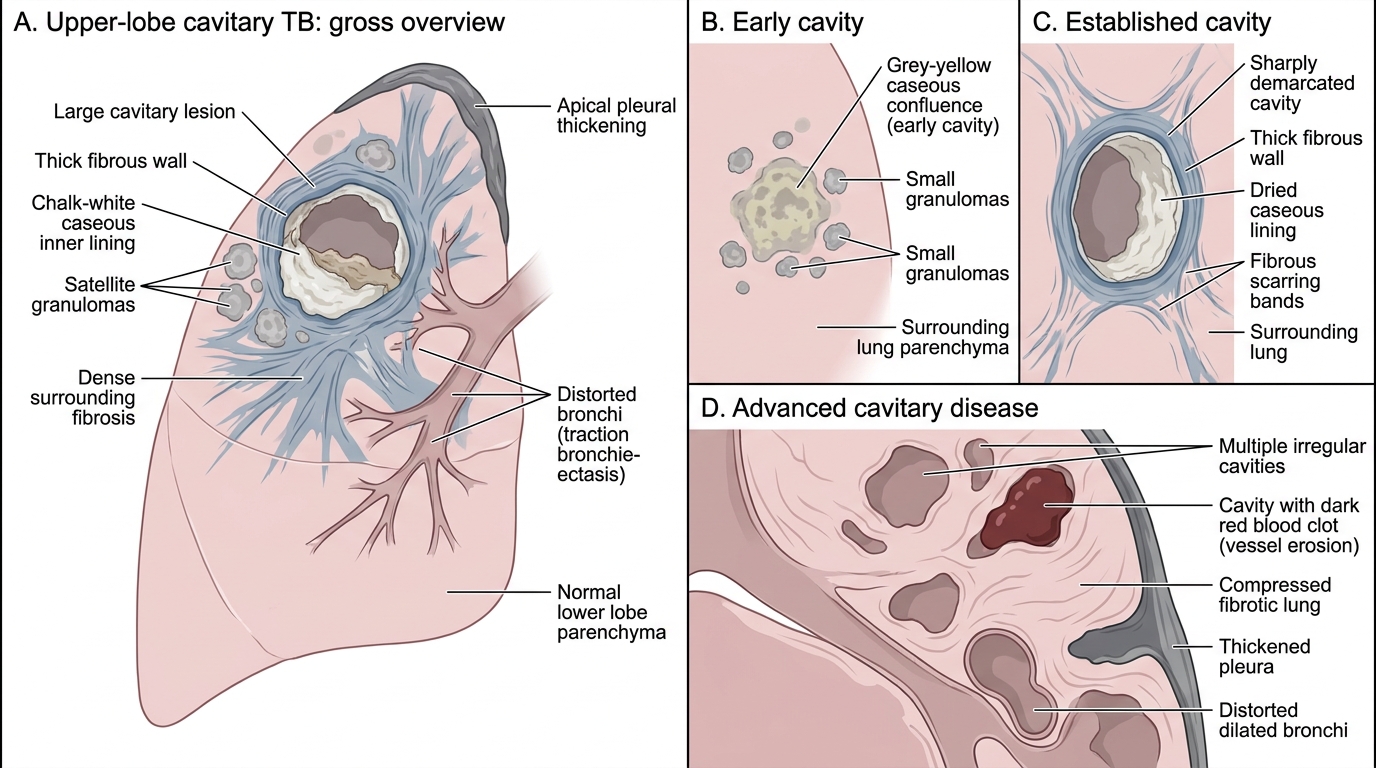
The cavitary TB lung is a stark illustration of disease progression:
- Early cavity: grey-yellow caseous material filling a zone of confluence; no defined wall; surrounding granulomas visible as grey nodules in the parenchyma.
- Established cavity: well-defined cavity with a thick fibrous wall; inner surface lined with dried caseous material (may appear chalk-white or grey); surrounding lung shows dense fibrous bands (old scarring from healed prior disease).
- Advanced disease: multiple cavities, varying size; some contain blood clot (from vessel erosion); surrounding lung compressed and fibrotic; pleura thickened; bronchi distorted (traction bronchiectasis).
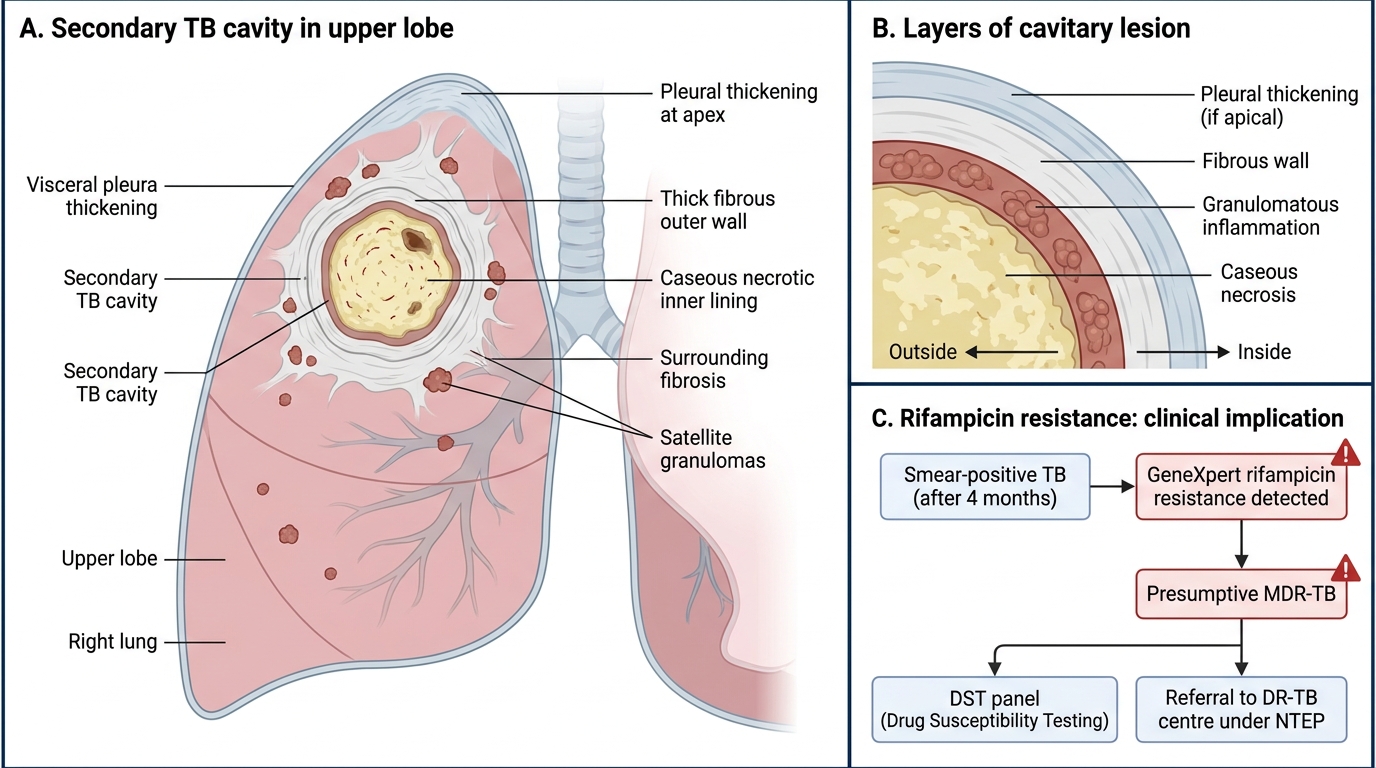
Secondary Tuberculosis Cavitary Lesion in Upper Lobe
SELF-CHECK
A 45-year-old male with smear-positive TB on RNTCP treatment for 4 months is found to have persistent AFB on sputum smear. GeneXpert detects rifampicin resistance. What is the correct classification?
A. XDR-TB — because he has failed all first-line drugs
B. Latent TB — because smear positivity after 4 months indicates dormant bacilli
C. MDR-TB — resistance to at least isoniazid and rifampicin confirmed
D. Drug-susceptible TB — rifampicin resistance alone is not sufficient for MDR classification
Reveal Answer
Answer: C. MDR-TB — resistance to at least isoniazid and rifampicin confirmed
MDR-TB is defined as resistance to at least isoniazid AND rifampicin. GeneXpert detects rifampicin resistance as a proxy for MDR-TB (because rifampicin resistance almost never occurs in isolation without concurrent isoniazid resistance in clinical practice). XDR-TB additionally requires resistance to fluoroquinolones and injectable second-line drugs. This patient needs a Drug Susceptibility Test panel and referral to a DR-TB centre under NTEP.