Page 18 of 32
PA25.6 | Tumours of the Lung & Pleura — SDL Guide
Learning Objectives
- Identify the major aetiological factors for lung carcinoma, with emphasis on tobacco smoke and its dose-response relationship
- Distinguish small-cell lung carcinoma (SCLC) from non-small-cell lung carcinoma (NSCLC) on the basis of histology, location, molecular profile, and clinical behaviour
- Describe the gross and microscopic features of the four principal lung carcinoma subtypes
- Explain the routes and sites of metastatic spread and apply TNM staging principles
- Enumerate paraneoplastic syndromes and link each to the causative tumour subtype
- Outline the pathology of malignant mesothelioma — its asbestos aetiology, macroscopy, histological variants, and immunohistochemical distinction from metastatic adenocarcinoma
INSTRUCTIONS
Lung cancer is the leading cause of cancer death worldwide in both sexes. As a Year-2 student you have encountered general tumour biology; this module builds on that foundation to give you the specific clinico-pathological framework you will use in clinical years to interpret radiology reports, understand surgical staging, and correlate paraneoplastic presentations with tumour type. The SCLC-vs-NSCLC distinction is not merely academic — it determines chemotherapy versus surgical management from the moment of diagnosis.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch. 15 — The Lung (textbook)
- Harsh Mohan: Textbook of Pathology, 8th ed., Ch. 16 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 58-year-old male smoker (40 pack-years) presents to the emergency department with facial puffiness, distended neck veins, and difficulty breathing while lying flat. His chest X-ray shows a right hilar mass. The registrar says: "Classic superior vena cava syndrome — probably small-cell." How does a tumour arising in the airway cause the face to swell? And how would the answer change management entirely compared to a peripheral lung nodule in a non-smoking woman? By the end of this module you will answer both questions with confidence.
WHY THIS MATTERS
Lung cancer accounts for more deaths than breast, colorectal, and prostate cancers combined. In India it is the commonest cancer in men and rising rapidly in women. As a clinician you will order staging CTs, interpret pleural fluid cytology reports, and counsel patients — all tasks that require you to know which subtype you are dealing with, because SCLC is treated with chemotherapy while NSCLC subtypes may be surgically resected or targeted with kinase inhibitors. The pathologist's report that lands in your outpatient folder will use the same vocabulary you are building today.
RECALL
Before proceeding, recall from Year-1 Pathology:
- Metaplasia — reversible change of one differentiated cell type to another; bronchial squamous metaplasia in smokers is a precursor lesion.
- Dysplasia → carcinoma in situ → invasive carcinoma — the stepwise progression underpinned by accumulating mutations.
- Proto-oncogenes (RAS, MYC) and tumour suppressor genes (TP53, RB1) — their roles in cell-cycle control.
- Paraneoplastic syndrome — symptoms caused by tumour secretion of hormones or immune cross-reactivity, not by direct tumour mass.
- Neuroendocrine cells — APUD cells present in bronchial epithelium; form the cell of origin for SCLC.
Aetiology and Risk Factors
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
Aetiology and Risk Factors for Lung Carcinoma
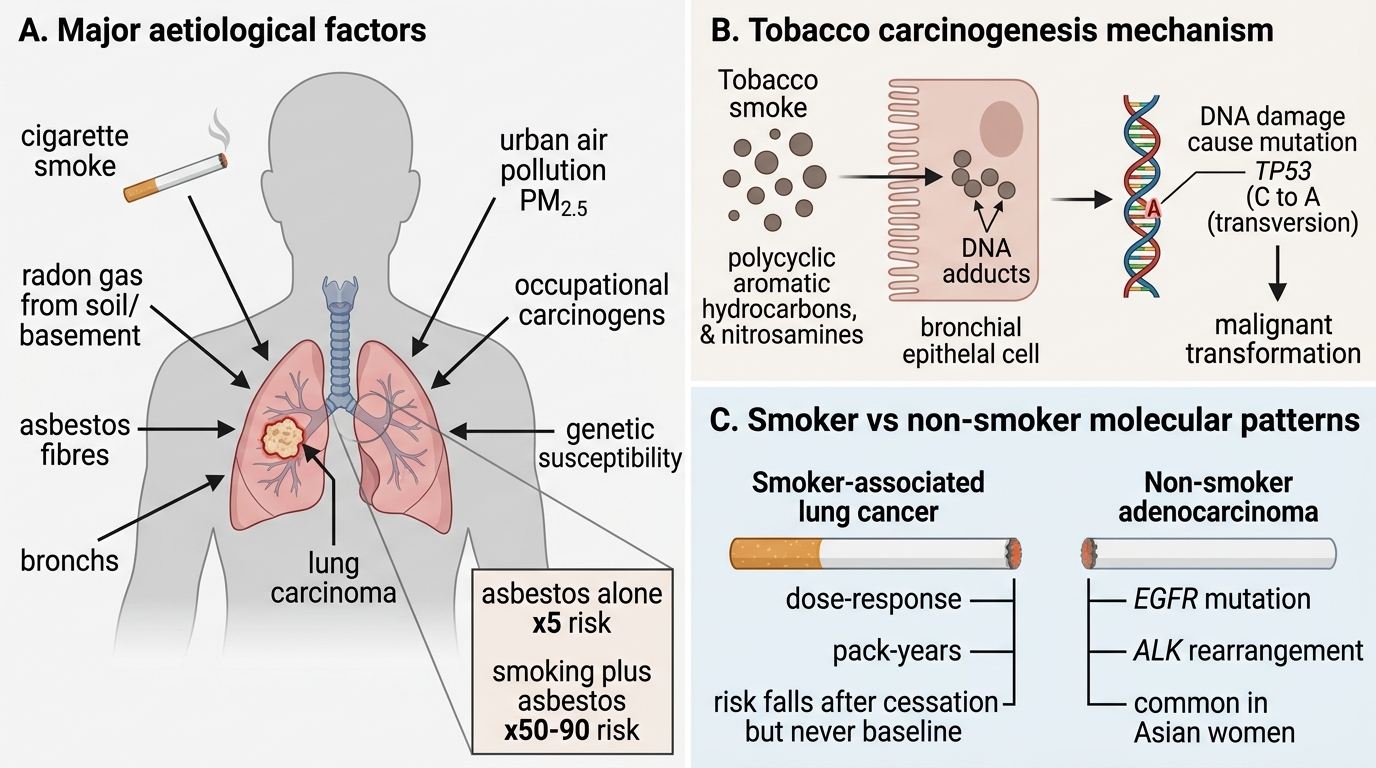
Cigarette smoking is the dominant cause, responsible for approximately 85% of all lung carcinomas. The relationship is dose-response: risk rises with pack-years and falls (but never returns to baseline) after cessation. Tobacco smoke contains polycyclic aromatic hydrocarbons and nitrosamines that form DNA adducts, causing characteristic C→A transversions in TP53.
Other aetiological factors:
- Radon gas — radioactive decay product of uranium in soil; second leading cause of lung cancer; important in uranium miners and in poorly ventilated homes.
- Asbestos — synergistic with smoking (risk × 50–90 in smokers vs × 5 alone); predominantly causes mesothelioma but also lung adenocarcinoma.
- Air pollution — urban particulate matter (PM2.5) and polycyclic hydrocarbons; contributes to rising adenocarcinoma rates in non-smokers.
- Occupational exposures — arsenic, chromium, nickel, bis(chloromethyl) ether, ionising radiation.
- Genetic susceptibility — first-degree relatives of lung cancer patients have 2–3× higher risk; polymorphisms in carcinogen-metabolising enzymes (CYP1A1, GSTM1).
Non-smoker lung cancer (predominantly adenocarcinoma) is linked to EGFR mutations (common in Asian women) and ALK rearrangements rather than tobacco-associated mutations.
The Fundamental Clinical Division: SCLC vs NSCLC
SCLC vs NSCLC: Fundamental Clinical Division
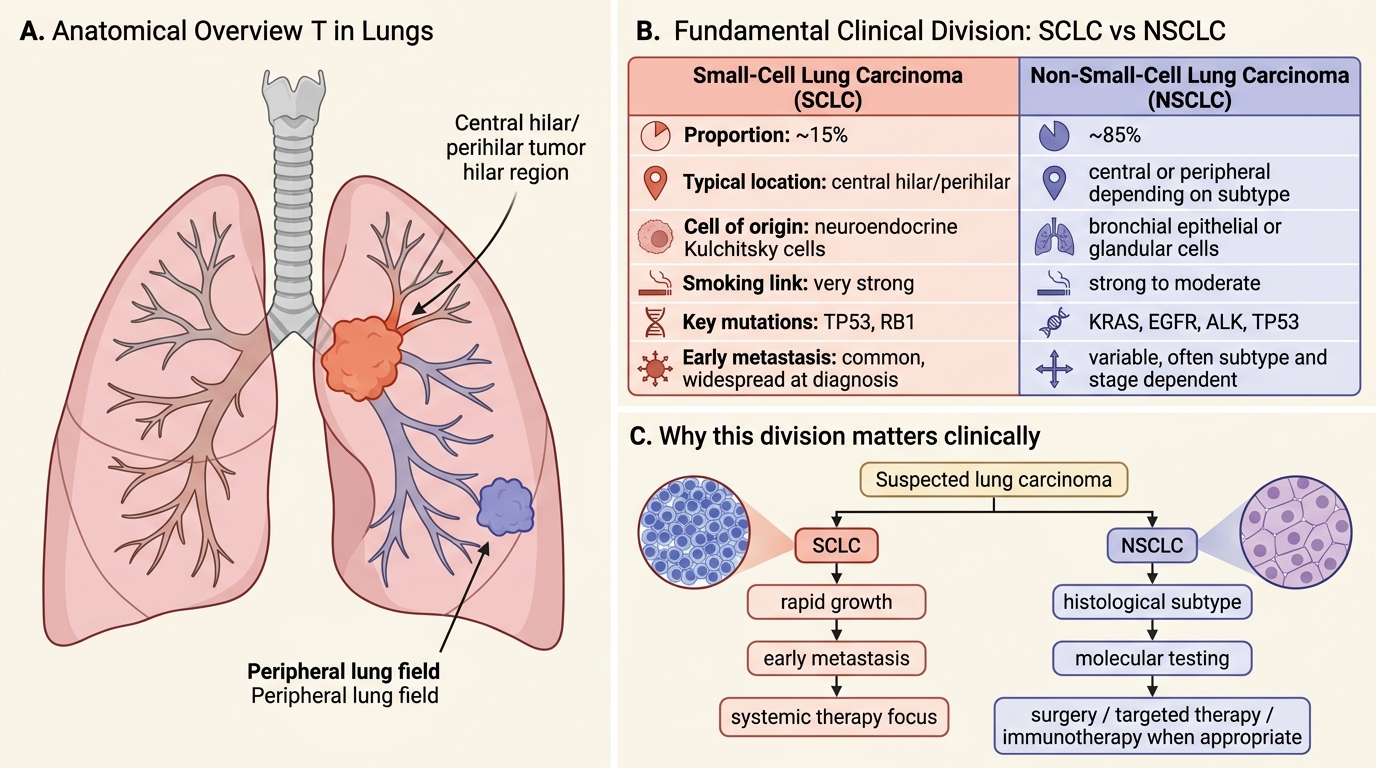
All lung carcinomas are first divided into two broad categories that determine management strategy before histological subtyping is even finalised.
| Feature | Small-Cell Lung Carcinoma (SCLC) | Non-Small-Cell Lung Carcinoma (NSCLC) |
|---|---|---|
| Proportion | ~15% | ~85% |
| Location | Central (hilar/perihilar) | Central or peripheral depending on subtype |
| Cell of origin | Neuroendocrine (Kulchitsky) cells | Bronchial epithelial or glandular cells |
| Smoking link | Very strong | Strong (SCC, LCC) to moderate (adeno) |
| Key mutations | TP53, RB1 | KRAS, EGFR, ALK, TP53 (subtype-specific) |
| Early metastasis | Yes — widespread at diagnosis | Less common at presentation |
| Surgery | NOT surgical — disseminated | Potentially resectable (stages I–IIIa) |
| Primary treatment | Chemotherapy ± radiotherapy | Surgery, targeted therapy, immunotherapy, or chemo |
| Paraneoplastic | Frequent, distinctive | Less frequent |
This table is the diagnostic anchor of the entire module. Burn it in.
SCLC vs NSCLC: Location and Key Pathological Features
Small-Cell Lung Carcinoma (SCLC) — Pathology
Small-Cell Lung Carcinoma: Pathology Overview
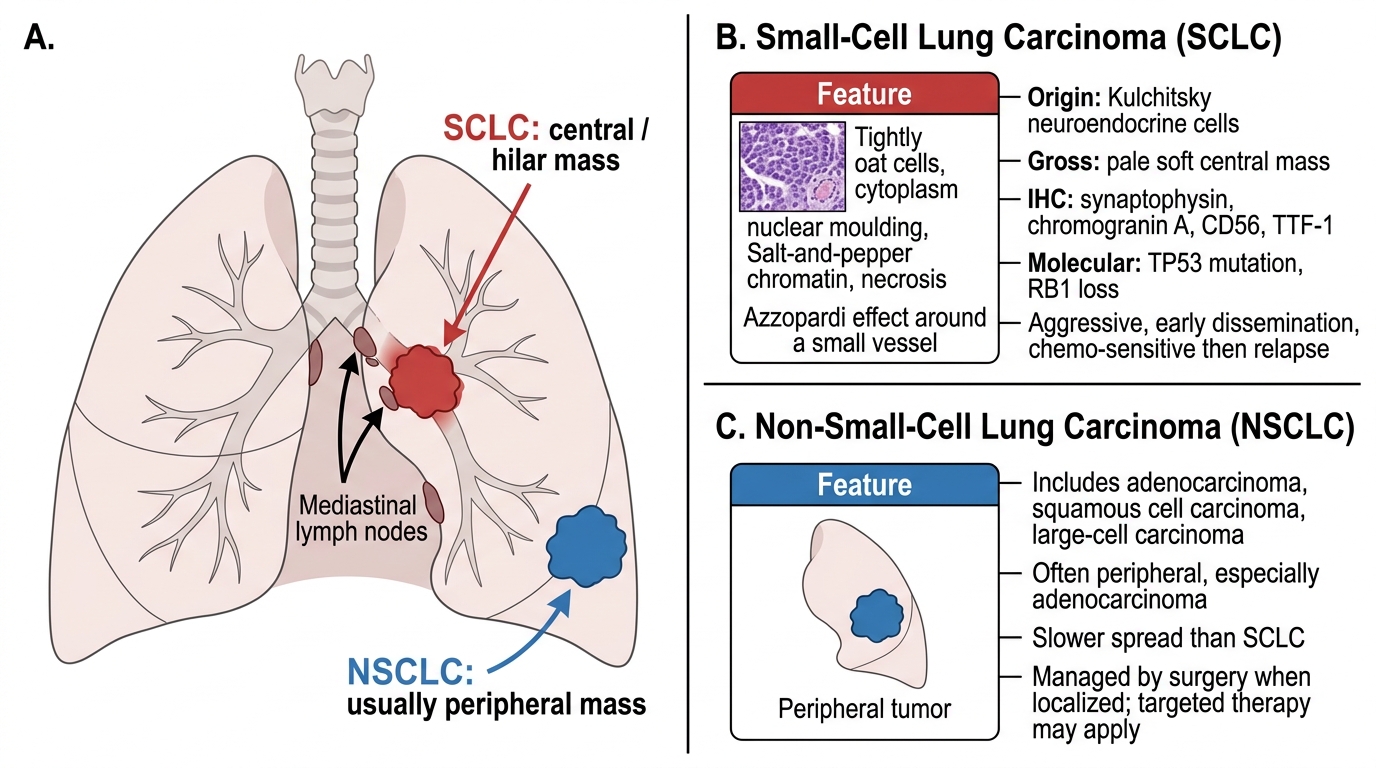
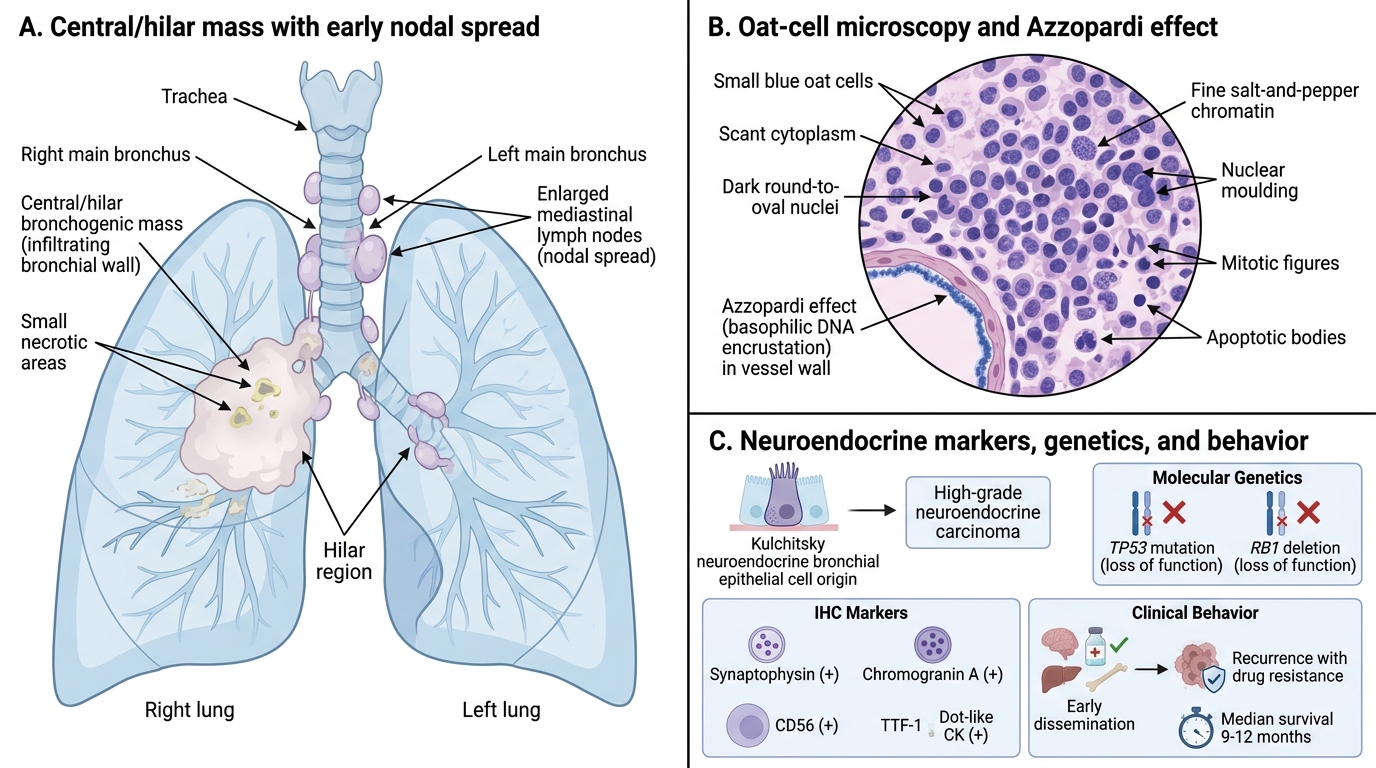
SCLC arises from Kulchitsky cells (neuroendocrine cells) of the bronchial epithelium, classifying it as a high-grade neuroendocrine carcinoma.
Gross morphology: Pale, soft, central/hilar mass that infiltrates bronchial walls early. Necrosis is prominent. Almost always associated with mediastinal nodal disease at presentation.
Microscopy — the oat cell:
• Small cells with scant cytoplasm, dark round-to-oval nuclei, fine "salt-and-pepper" chromatin (neuroendocrine pattern).
• Cells are roughly twice the size of a lymphocyte — the classic oat cell appearance.
• Nuclear moulding (cells indent each other).
• Azzopardi effect — DNA encrustation of vessel walls from necrotic tumour cells (pathognomonic of SCLC).
• Mitoses and apoptotic bodies are abundant.
IHC markers: synaptophysin, chromogranin A, CD56 (neuroendocrine); TTF-1 positive; CK positive in a dot-like pattern.
Molecular: TP53 mutation in >90%; RB1 deletion almost universal — both suppress the neuroendocrine differentiation restraint.
Behaviour: Extremely aggressive. Already disseminated in ~60–70% at diagnosis. Paradoxically, initially chemo-sensitive (responds to platinum-etoposide), but almost invariably recurs as drug-resistant disease within 12–18 months. Median survival ~9–12 months.
SELF-CHECK
A bronchial biopsy shows small cells with scant cytoplasm, nuclear moulding, and DNA encrustation of vessel walls. IHC is synaptophysin-positive, TTF-1 positive. Which statement about this tumour is CORRECT?
A. Surgical resection is the first-line treatment
B. It arises from type II pneumocytes
C. RB1 deletion is present in nearly all cases
D. It is more common in non-smoking women with EGFR mutations
Reveal Answer
Answer: C. RB1 deletion is present in nearly all cases
The features describe small-cell lung carcinoma. RB1 deletion is found in ~90% of SCLC cases alongside TP53 mutation, reflecting its neuroendocrine origin. SCLC is NOT resected (it is almost always disseminated at diagnosis); it arises from Kulchitsky (neuroendocrine) cells, not type II pneumocytes; and EGFR-mutant, non-smoking profile is characteristic of peripheral adenocarcinoma.