Page 19 of 32
PA25.6 | Tumours of the Lung & Pleura — SDL Guide (Part 2)
NSCLC Type 1 — Squamous Cell Carcinoma
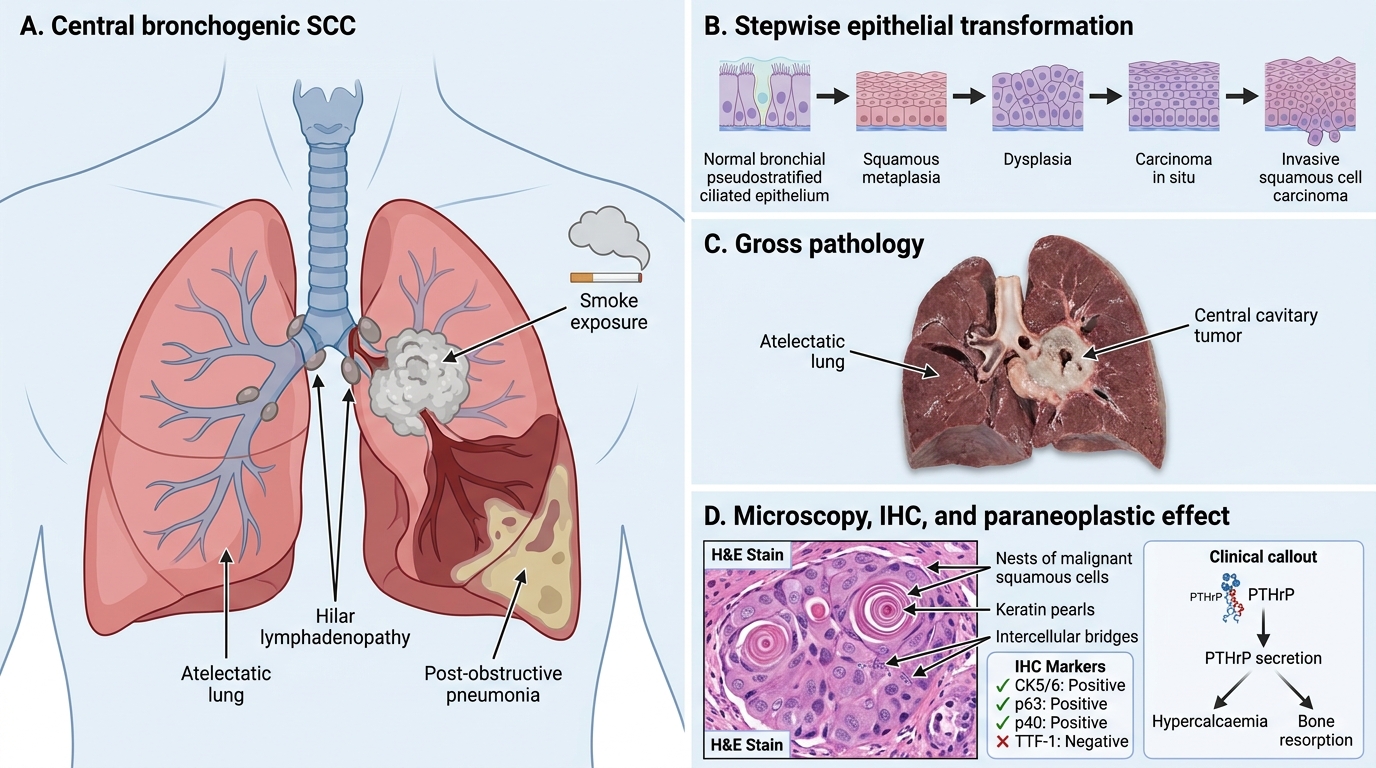
Squamous Cell Carcinoma of Lung
Squamous cell carcinoma (SCC) of the lung accounts for ~25–30% of all lung cancers and has the strongest association with heavy smoking among NSCLC subtypes.
Location: Central — arises from bronchial epithelium (preceded by squamous metaplasia → dysplasia → carcinoma in situ) in segmental or lobar bronchi. May cavitate.
Gross: Grey-white, firm, central mass. Cavitation (central necrosis) in up to 10–15%.
Microscopy:
• Keratin pearls (whorled concentrically layered squamous cells with central keratinisation) — pathognomonic.
• Intercellular bridges (desmosomes) between tumour cells.
• Well to poorly differentiated; poorly differentiated SCC may lack pearls.
IHC: CK5/6, p63, p40 positive; TTF-1 negative.
Key molecular: TP53, CDKN2A (p16) deletion; FGFR1 amplification.
Paraneoplastic: Hypercalcaemia via PTHrP (parathyroid hormone-related peptide) secretion — the most characteristic paraneoplastic of SCC.
Clinical note: Central location causes endobronchial obstruction → post-obstructive pneumonia, haemoptysis, atelectasis.
NSCLC Type 2 — Adenocarcinoma
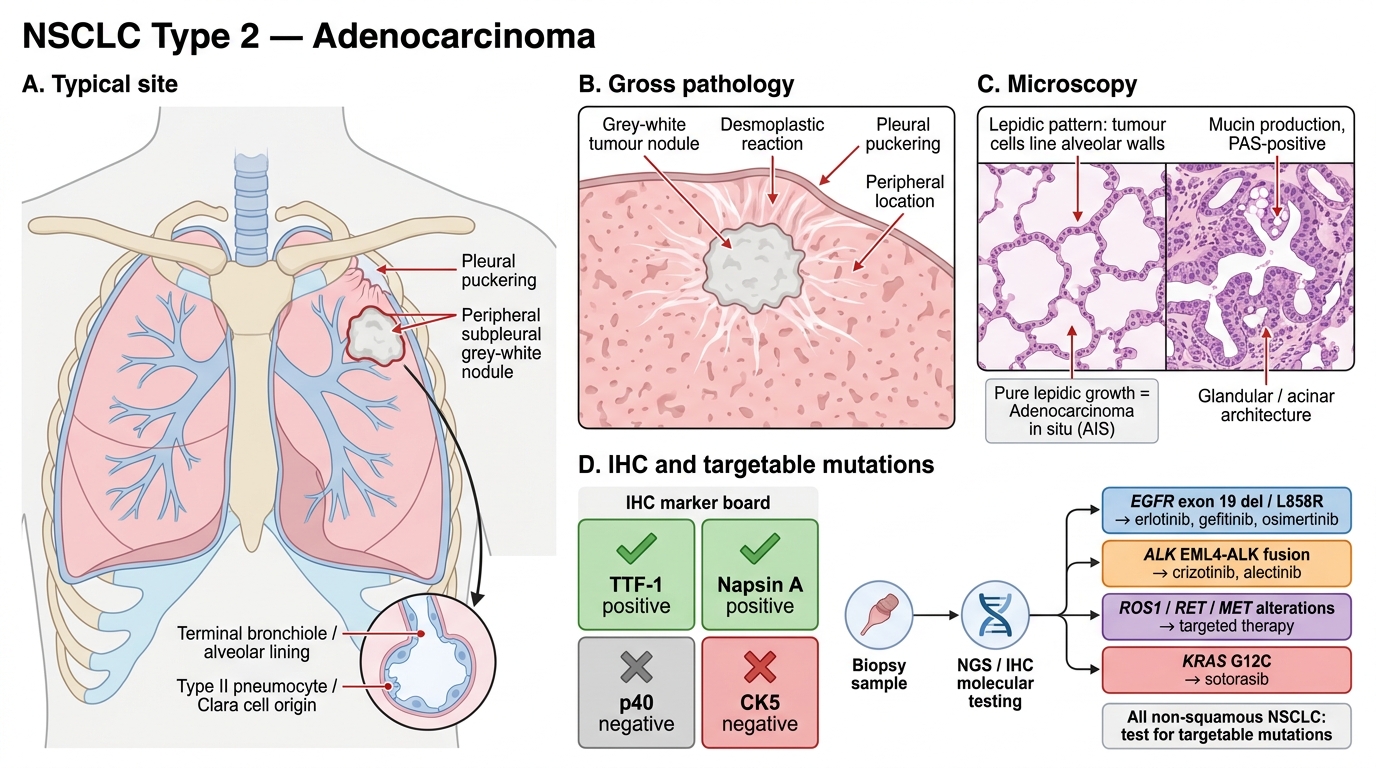
Lung Adenocarcinoma: Site, Histology, and Molecular Targets
Adenocarcinoma is now the single commonest subtype of lung cancer overall (~40%) and is the predominant type in non-smokers, women, and younger patients.
Location: Peripheral — arises from terminal bronchioles or alveolar lining (type II pneumocytes / Clara cells). Often subpleural.
Gross: Peripheral grey-white nodule, frequently with pleural puckering (desmoplastic reaction). The lepidic pattern grows along alveolar walls without destruction — this is the non-invasive precursor lesion (adenocarcinoma in situ, formerly BAC).
Microscopy:
• Glandular/tubular/papillary/acinar architecture.
• Mucin production (PAS-positive).
• Lepidic pattern — tumour cells line alveolar walls like wallpaper; purely lepidic = adenocarcinoma in situ (AIS).
IHC: TTF-1 positive (most important marker), Napsin A positive; p40/CK5 negative.
Targetable mutations — clinically critical:
• EGFR mutation (~15% Western, ~40–50% Asian; exon 19 deletion or L858R point mutation) → targeted by erlotinib, gefitinib, osimertinib.
• ALK rearrangement (~5%; EML4-ALK fusion) → targeted by crizotinib, alectinib.
• ROS1, RET, MET alterations — rarer but targetable.
• KRAS mutation — commonest driver (~30%); historically untargetable, now targeted by sotorasib (KRAS G12C).
Note: Presence of targetable mutations mandates molecular testing (NGS/IHC) on all non-squamous NSCLC — this is now standard of care.
NSCLC Type 3 — Large Cell Carcinoma and Other Subtypes
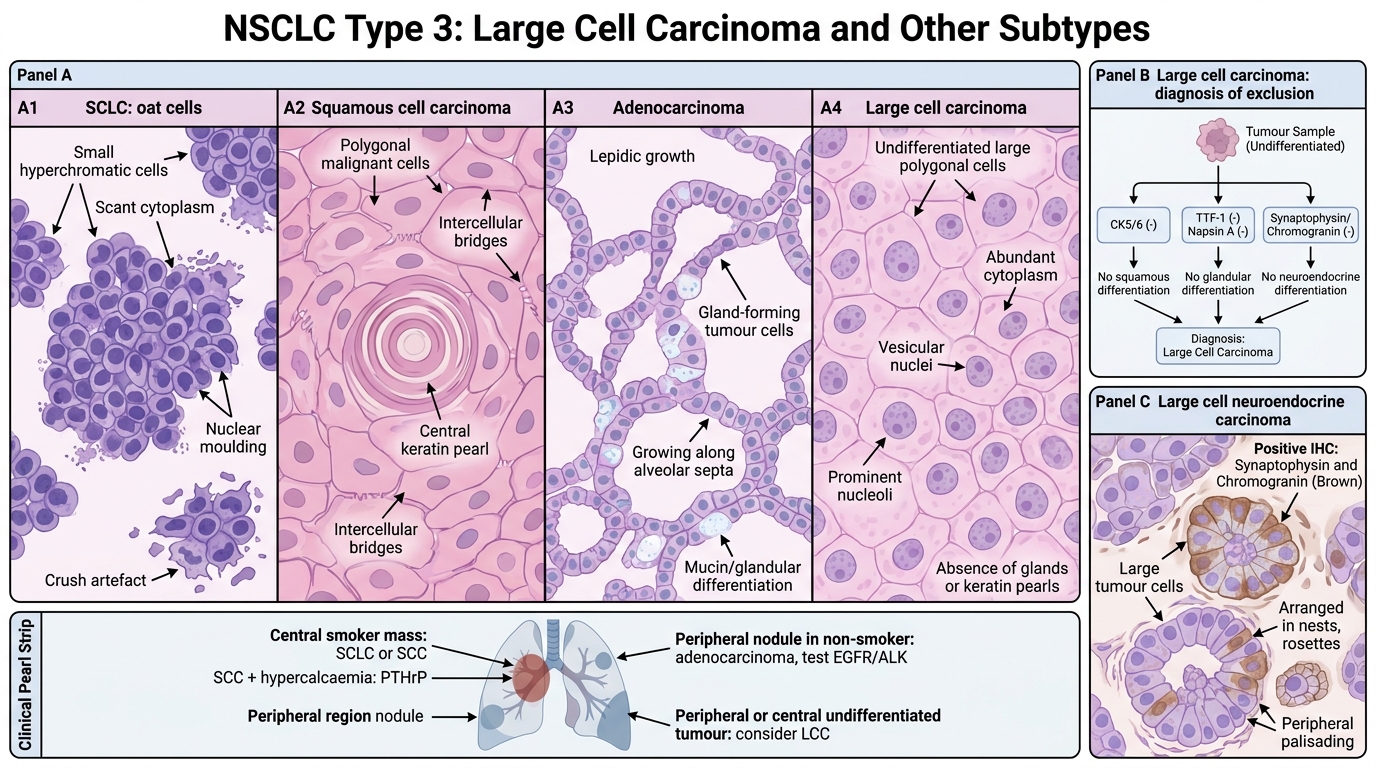
Large Cell Carcinoma and Major Lung Carcinoma Subtypes
Large cell carcinoma (LCC) is a diagnosis of exclusion (~10% of lung cancers): undifferentiated NSCLC lacking squamous, glandular, or neuroendocrine differentiation on H&E and IHC.
Microscopy: Large cells with vesicular nuclei and prominent nucleoli; no keratin pearls, no glands. IHC negative for CK5/6, TTF-1, napsin A, neuroendocrine markers.
Behaviour: Peripheral or central; poor prognosis; no targetable mutations by definition.
Large cell neuroendocrine carcinoma (LCNEC): A distinct variant — large cells with neuroendocrine architecture (nesting, rosettes, peripheral palisading) and IHC expression of synaptophysin/chromogranin. Aggressive, treated similarly to SCLC.
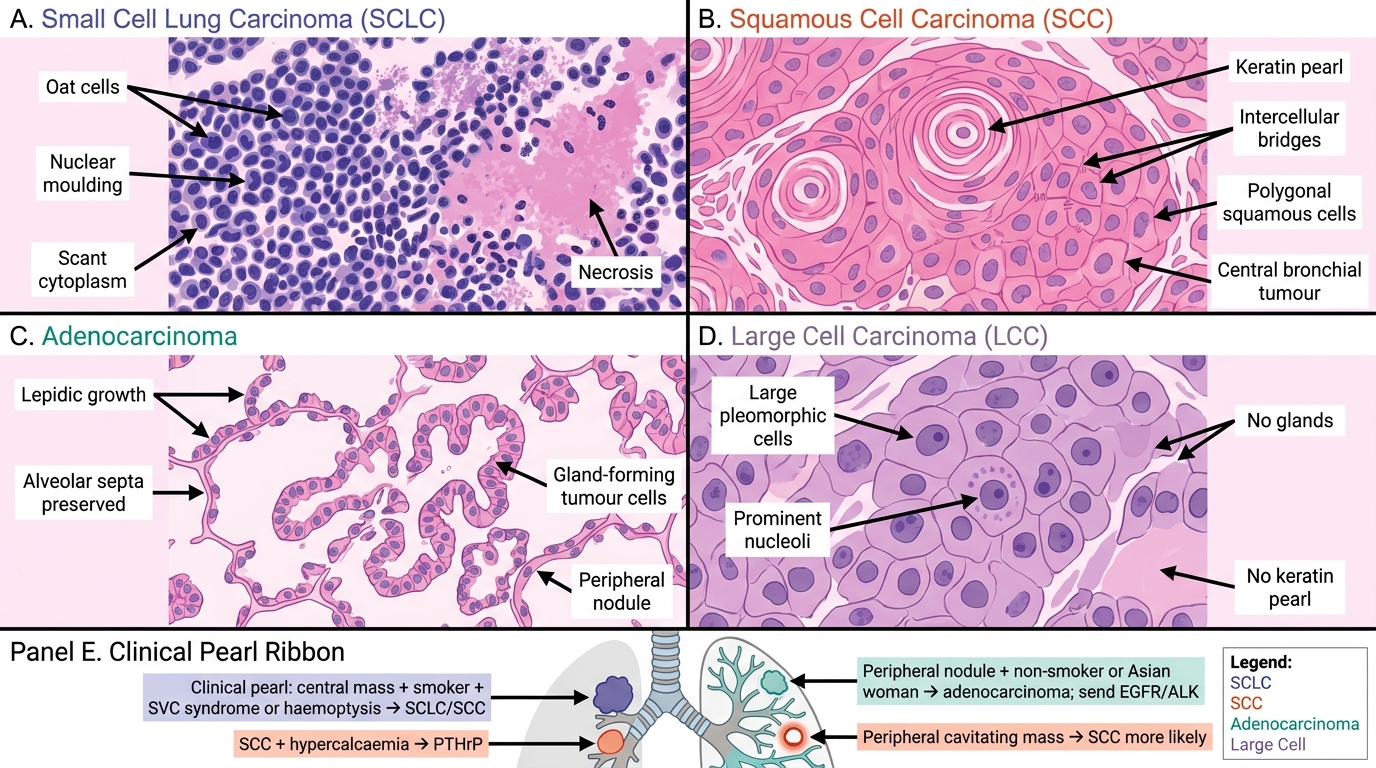
Microscopy Patterns of Major Lung Carcinoma Subtypes
CLINICAL PEARL
The periphery–centre rule for quick subtyping at the bedside:
- Central mass + smoker + SVC syndrome/haemoptysis → think SCLC or SCC.
- Central mass + SCC + hypercalcaemia → PTHrP is the mechanism (not bony metastases — confirm with normal bone scan).
- Peripheral nodule + non-smoker or Asian woman → adenocarcinoma; send EGFR/ALK regardless of clinical features.
- Peripheral cavitating mass → more likely SCC than adenocarcinoma (though abscess and fungal must be excluded).
This rule guides the initial management while awaiting the full pathology report.