Page 20 of 32
PA25.6 | Tumours of the Lung & Pleura — SDL Guide (Part 3)
Spread, Metastasis, and TNM Staging
Spread and TNM Staging of Lung Cancer
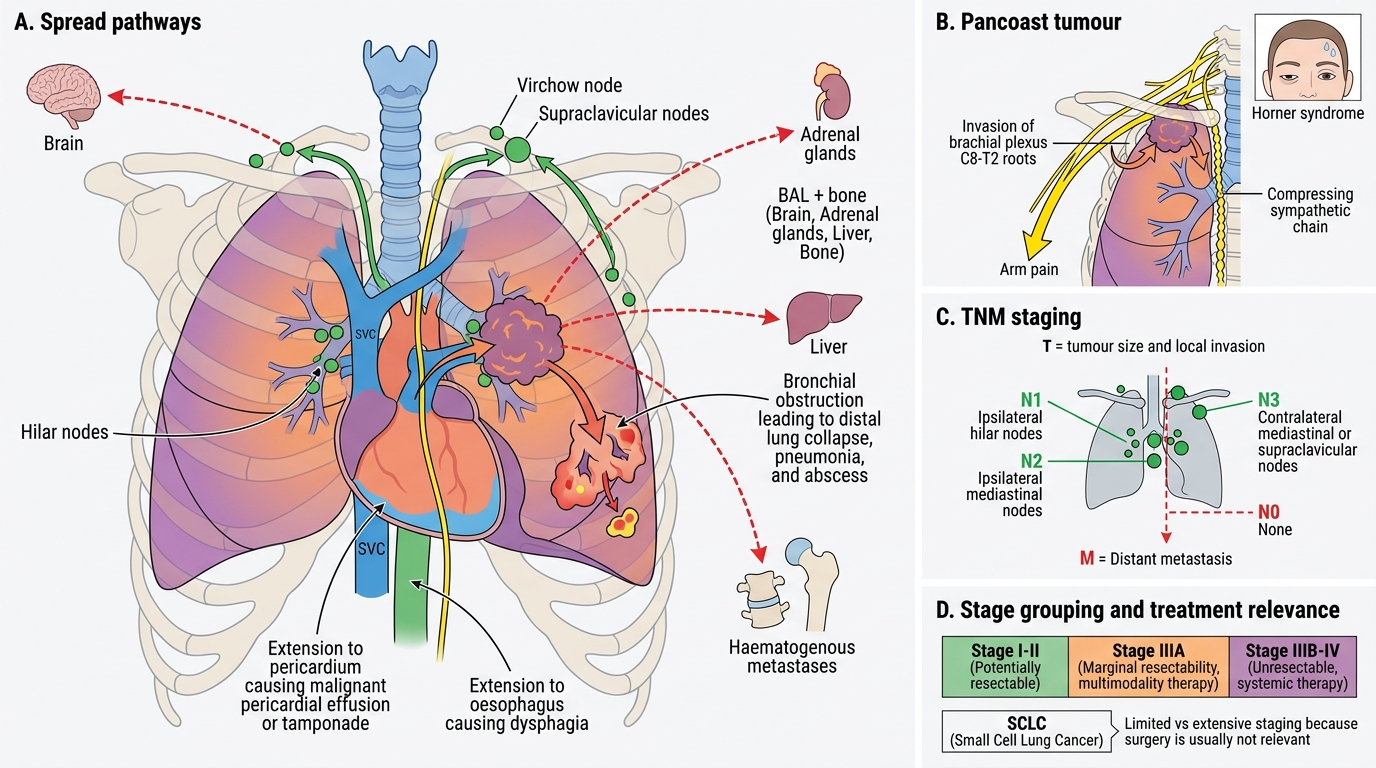
Local spread:
• Bronchial obstruction → collapse, pneumonia, abscess.
• Hilar/mediastinal spread → superior vena cava (SVC) obstruction (SVCO): facial oedema, plethora, distended neck veins; most often SCLC or central SCC.
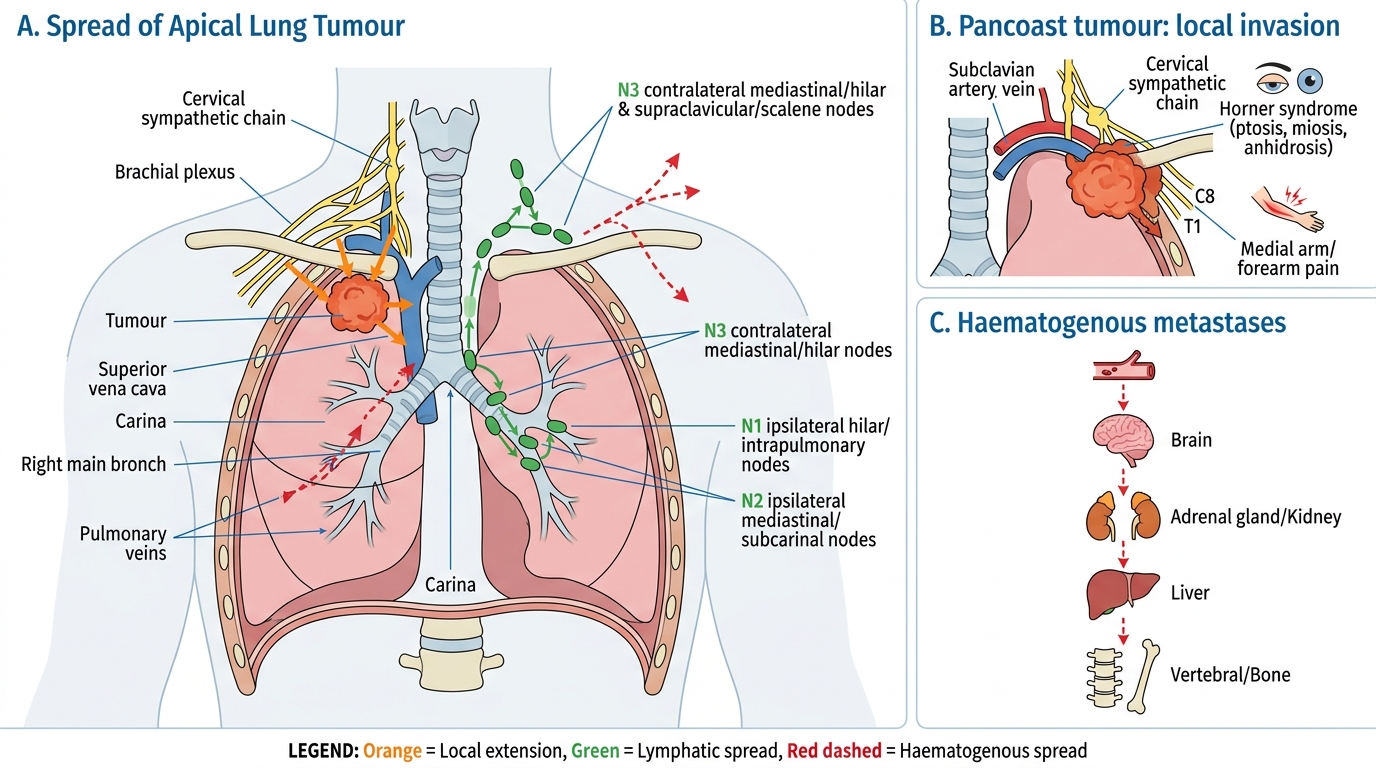
• Apical (Pancoast/superior sulcus) tumour → invades brachial plexus (C8-T2) causing arm pain + Horner syndrome (ptosis, miosis, anhidrosis) from sympathetic chain compression.
• Pericardial involvement → malignant pericardial effusion/tamponade.
• Left recurrent laryngeal nerve → hoarseness.
• Oesophagus → dysphagia.
Lymphatic spread: Hilar nodes → mediastinal nodes → supraclavicular (Virchow) nodes.
Haematogenous metastases — the "BAL" mnemonic: Brain, Adrenal, Liver, bone (also — adrenal metastases are almost always bilateral and cortex-derived; rarely cause Addison's clinically).
TNM Staging (8th edition, IASLC):
• T = tumour size and extent of local invasion.
• N = nodal involvement (N0 = none; N1 = ipsilateral hilar; N2 = ipsilateral mediastinal; N3 = contralateral or supraclavicular).
• M = distant metastasis.
• Stage I–II: potentially resectable.
• Stage IIIA: marginal resectability (multimodality).
• Stage IIIB–IV: unresectable (systemic therapy).
• SCLC uses a simpler limited vs extensive staging because surgery is not relevant.
Pathways of Lung Cancer Spread
SELF-CHECK
A 62-year-old male with a right upper lobe mass develops ptosis and miosis of the right eye, along with pain radiating down the inner aspect of the right arm. Which of the following BEST explains these findings?
A. Haematogenous metastasis to the brain causing a third-nerve palsy
B. Apical tumour invading the cervical sympathetic chain and brachial plexus
C. SVC obstruction reducing venous return from the orbit
D. Paraneoplastic antibodies targeting the autonomic nervous system
Reveal Answer
Answer: B. Apical tumour invading the cervical sympathetic chain and brachial plexus
Pancoast (superior sulcus) tumour at the apex invades the first rib and adjoining structures. Compression of the cervical sympathetic chain (T1 sympathetic fibres) causes ipsilateral Horner syndrome (ptosis, miosis, anhidrosis). Simultaneous invasion of the lower brachial plexus (C8–T1) causes medial arm and ulnar distribution pain. This is a classical presentation of a Pancoast tumour — most often SCC or adenocarcinoma.
Paraneoplastic Syndromes — Linked to Tumour Subtype
Provided image
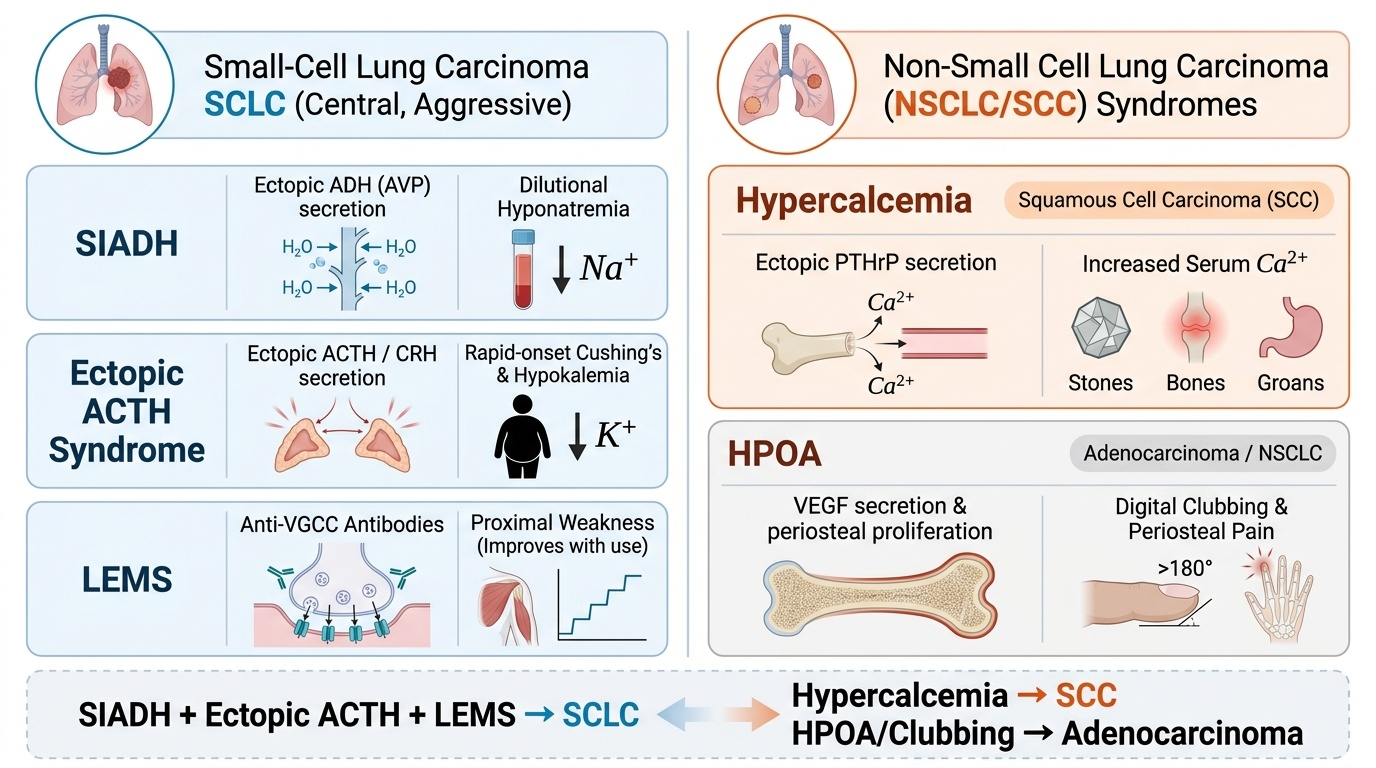
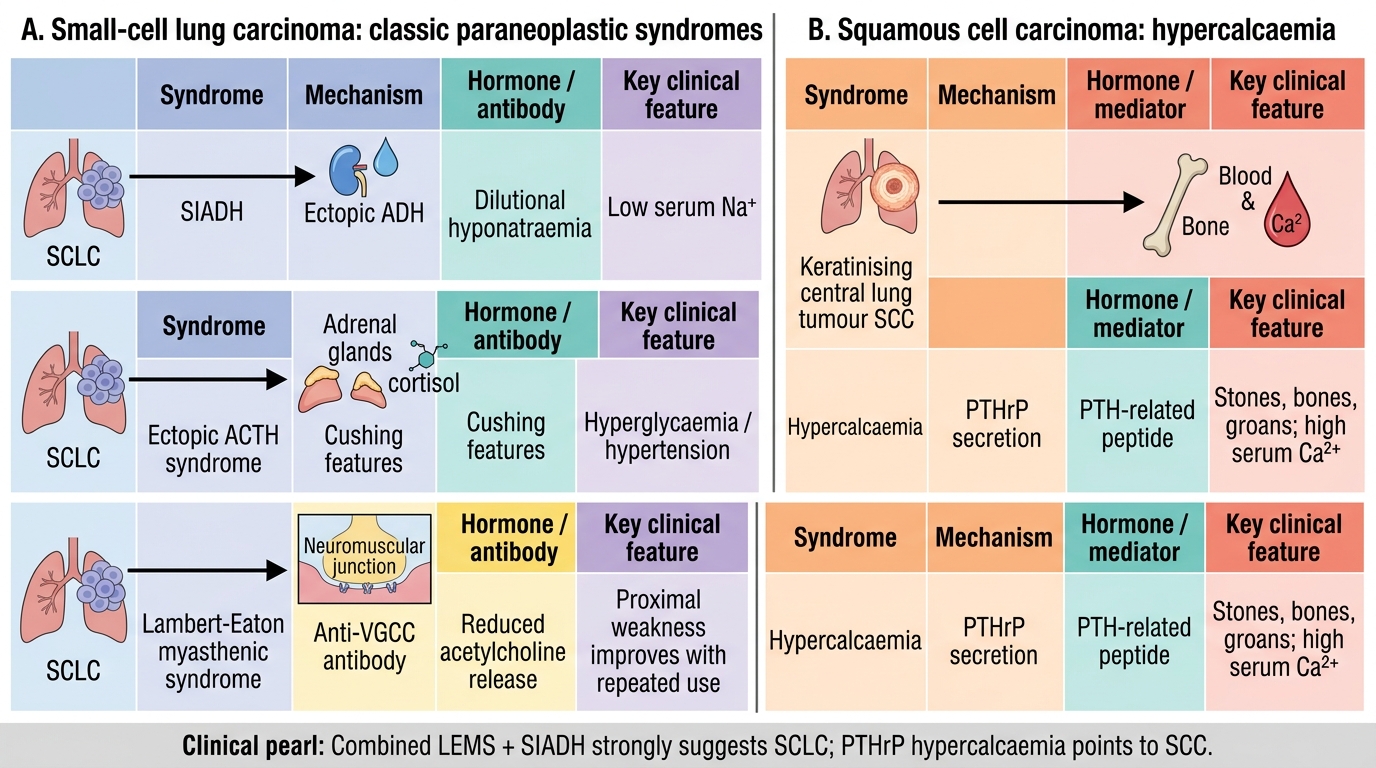
Paraneoplastic syndromes arise from tumour secretion of biologically active peptides, hormones, or induction of immune cross-reactivity — NOT from direct tumour infiltration or metastasis. Recognising them is clinically important: they may antedate the tumour diagnosis.
| Syndrome | Mechanism | Tumour subtype |
|---|---|---|
| SIADH (hyponatraemia) | Ectopic ADH (AVP) secretion | SCLC (most common cause of SIADH in cancer) |
| Ectopic ACTH syndrome (Cushing's) | Ectopic ACTH or CRH secretion | SCLC — rapid-onset Cushing's, hypokalaemic alkalosis |
| Lambert-Eaton myasthenic syndrome (LEMS) | Anti-VGCC antibodies (autoimmune) | SCLC — proximal limb weakness, preserved reflexes that improve with repetitive stimulation |
| Hypercalcaemia | Ectopic PTHrP | Squamous cell carcinoma |
| Hypertrophic pulmonary osteoarthropathy (HPOA) | Periosteal proliferation; VEGF? | NSCLC (all subtypes, especially adenocarcinoma) — clubbing + periosteal pain + X-ray periostitis |
| Carcinoid syndrome | Serotonin | Carcinoid tumour (not lung carcinoma) — flushing, diarrhoea |
Key exam differentiator: SIADH + ectopic ACTH + LEMS → SCLC. Hypercalcaemia → SCC.
Paraneoplastic Syndromes in Lung Cancer
SELF-CHECK
A patient with lung cancer develops proximal muscle weakness that paradoxically IMPROVES with repeated use. Serum sodium is 128 mEq/L. Which tumour type and mechanism BEST explains the combined picture?
A. Squamous cell carcinoma secreting PTHrP
B. Adenocarcinoma with ALK rearrangement causing neuropathy
C. Small-cell carcinoma causing LEMS (anti-VGCC) and SIADH (ectopic ADH)
D. Large cell carcinoma with hypercalcaemia and myopathy
Reveal Answer
Answer: C. Small-cell carcinoma causing LEMS (anti-VGCC) and SIADH (ectopic ADH)
Lambert-Eaton myasthenic syndrome (LEMS) causes proximal weakness that characteristically improves with repetitive stimulation (unlike true myasthenia gravis), because brief repeated activity transiently increases calcium influx through the partially blocked VGCC. SIADH from ectopic ADH secretion causes hyponatraemia. Both are classic paraneoplastic syndromes of SCLC. PTHrP-mediated hypercalcaemia is the hallmark of SCC, not SCLC.
Malignant Mesothelioma — Pleural Tumour
Malignant Pleural Mesothelioma
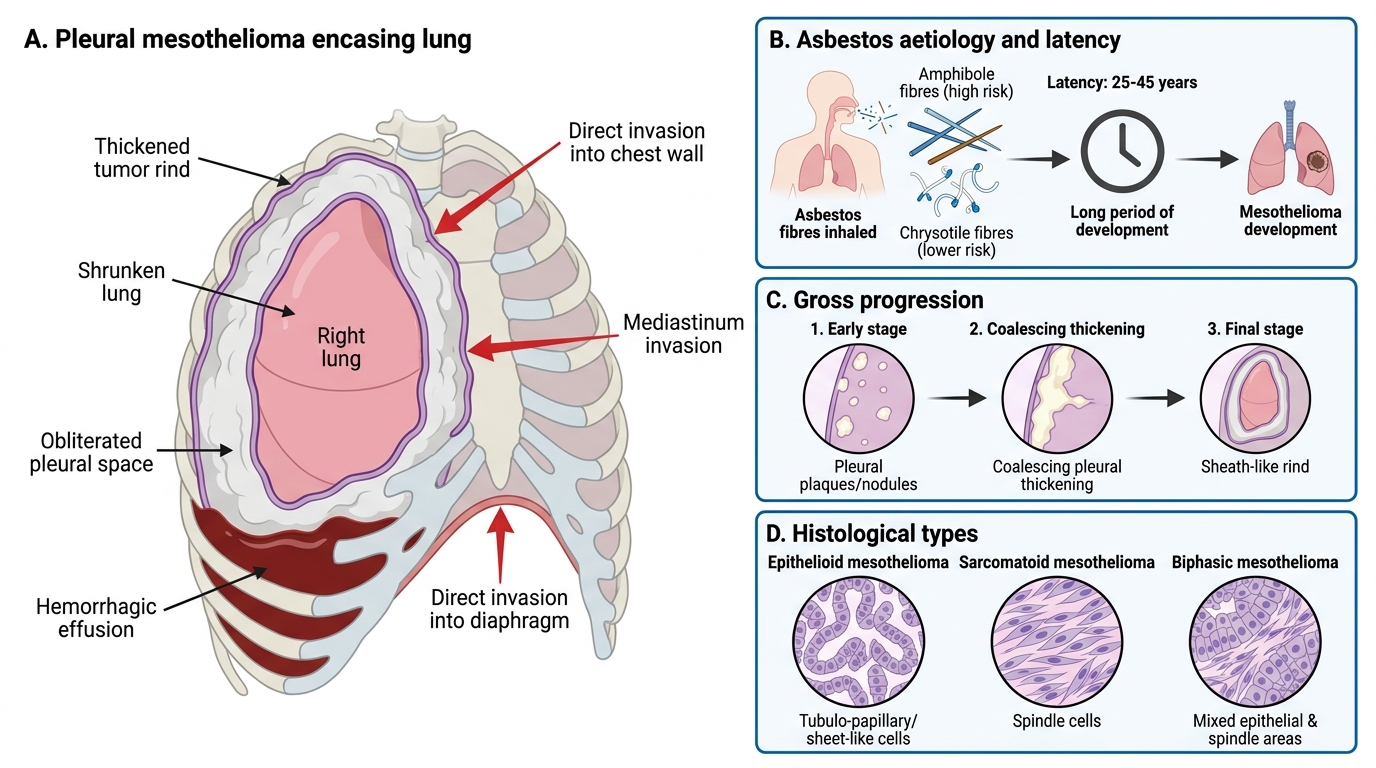
Malignant mesothelioma is a primary pleural malignancy arising from mesothelial cells lining the pleura (less commonly the peritoneum or pericardium).
Aetiology — asbestos is the dominant cause:
• ~80% of cases are attributable to asbestos exposure.
• Latency is characteristically long: 25–45 years after first exposure — important medico-legal and epidemiological point.
• Asbestos fibre type matters: amphibole fibres (crocidolite = blue asbestos; amosite = brown) carry far higher mesothelioma risk than chrysotile (white asbestos) due to their needle-like shape and lung-persistent biopersistence.
• Mesothelioma from asbestos does NOT require cigarette smoking co-exposure (unlike asbestos-associated lung carcinoma).
• BAP1 germline mutation increases susceptibility.
Gross pathology: Mesothelioma does not form a discrete mass. Instead:
• Starts as small pleural plaques or nodules.
• Progresses to a thick, sheath-like rind of tumour that encases the lung entirely — the lung shrinks within a cage of tumour.
• Obliterates the pleural space; massive exudative pleural effusion (haemorrhagic).
• Invades chest wall, mediastinum, diaphragm — direct invasion rather than haematogenous spread.
Histological types:
• Epithelioid (~60%) — tubulo-papillary or sheet-like; best prognosis among the three.
• Sarcomatoid (~20%) — spindle cells; worst prognosis.
• Biphasic (~20%) — mixed; intermediate prognosis.
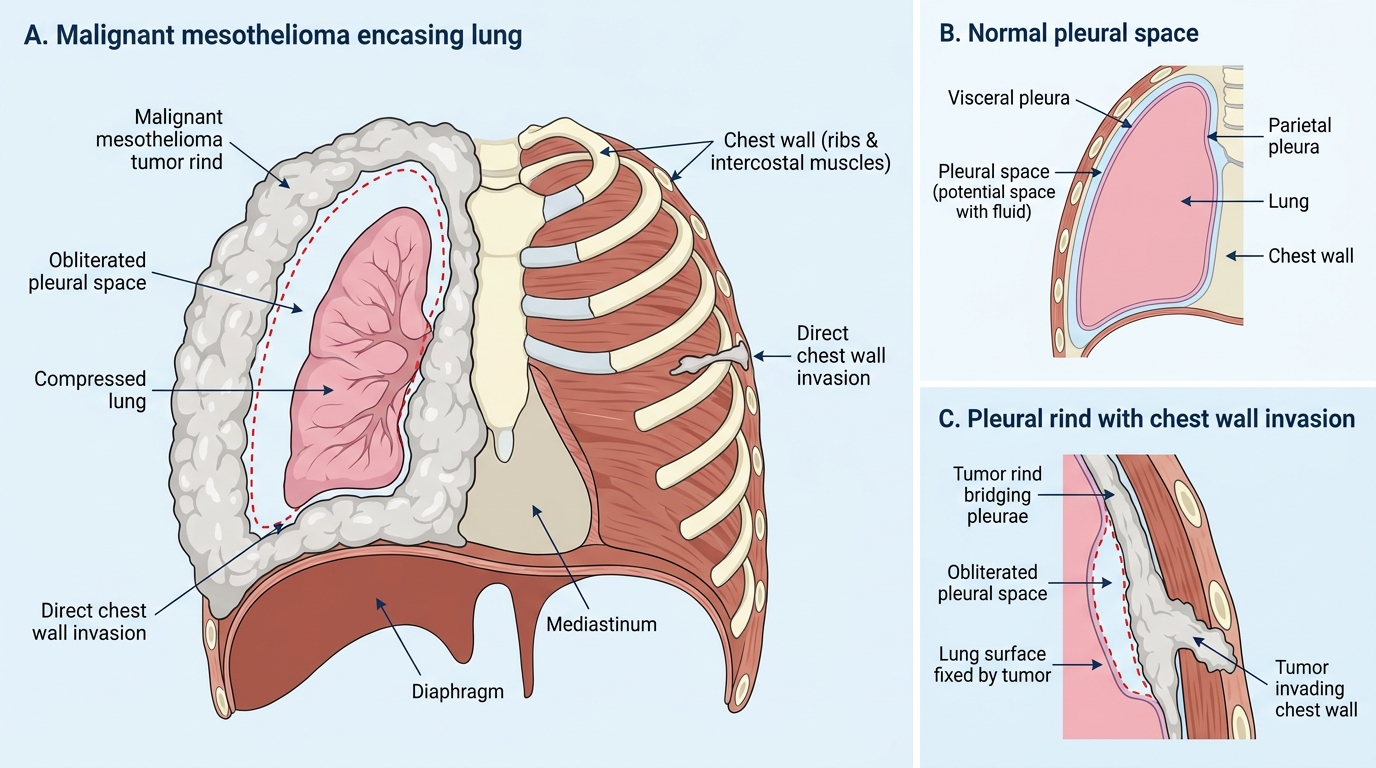
Malignant Mesothelioma Encasing the Lung