Page 21 of 32
PA25.6 | Tumours of the Lung & Pleura — SDL Guide (Part 4)
Mesothelioma vs Metastatic Adenocarcinoma — IHC Distinction
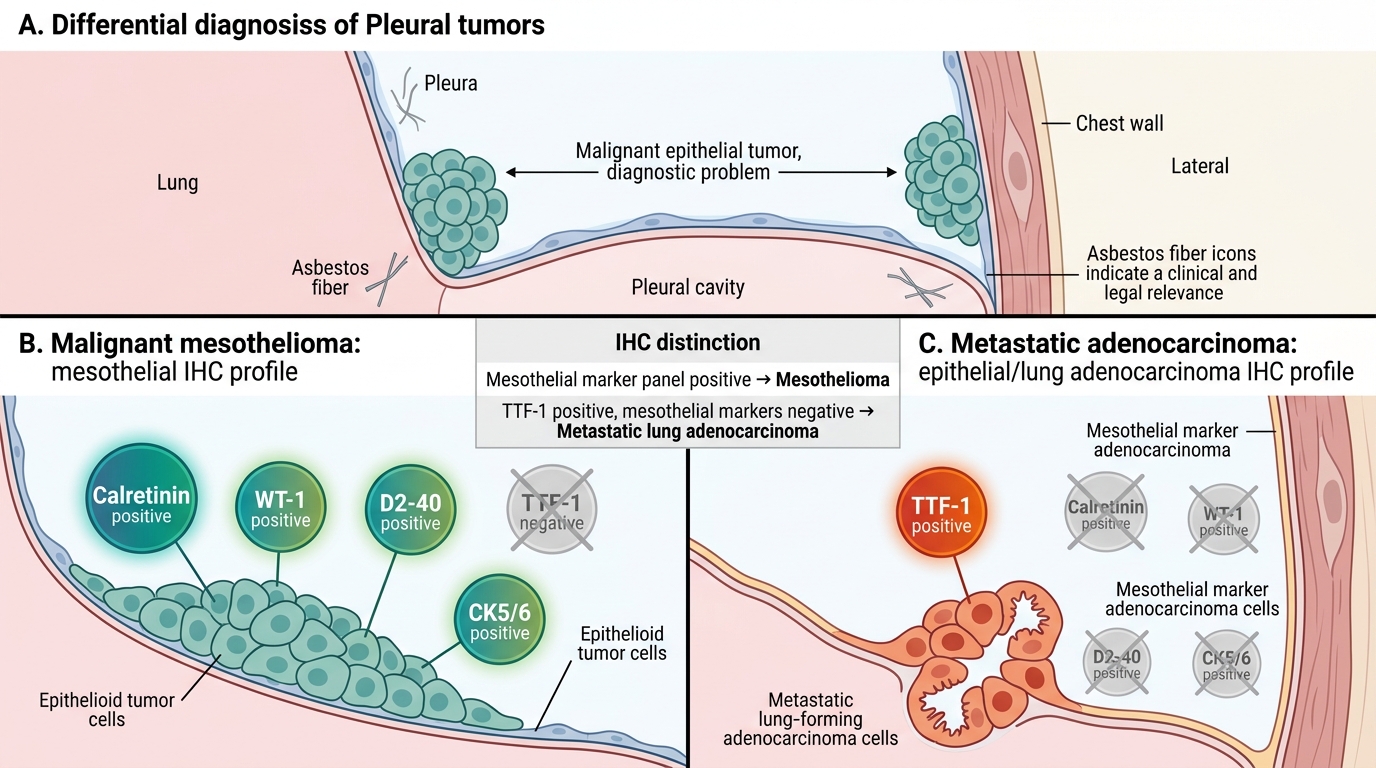
Mesothelioma vs Metastatic Adenocarcinoma: IHC Distinction
A critical diagnostic challenge: malignant mesothelioma (especially epithelioid type) mimics metastatic adenocarcinoma in the pleural space. The distinction is clinically vital because management and legal implications (asbestos compensation) differ entirely.
The IHC panel:
| Marker | Mesothelioma | Metastatic Adenocarcinoma |
|---|---|---|
| Calretinin | ✓ Positive | Negative |
| WT-1 | ✓ Positive | Negative |
| D2-40 (podoplanin) | ✓ Positive | Negative |
| CK5/6 | ✓ Positive | Negative (or focal) |
| TTF-1 | Negative | ✓ Positive (lung adeno) |
| CEA | Negative | ✓ Positive |
| MOC-31 | Negative | ✓ Positive |
Memory aid: "Calretinin, WT-1, D2-40 = MESothelioma"; TTF-1/CEA/MOC-31 = adenoCarcinoma.
Note: PAS-positive mucin vacuoles → adenocarcinoma. Long microvilli (EM) → mesothelioma.
Pleural effusion cytology alone is often insufficient; pleural biopsy with IHC panel is usually required for definitive diagnosis.
Other Pleural Tumours and Pleural Metastases
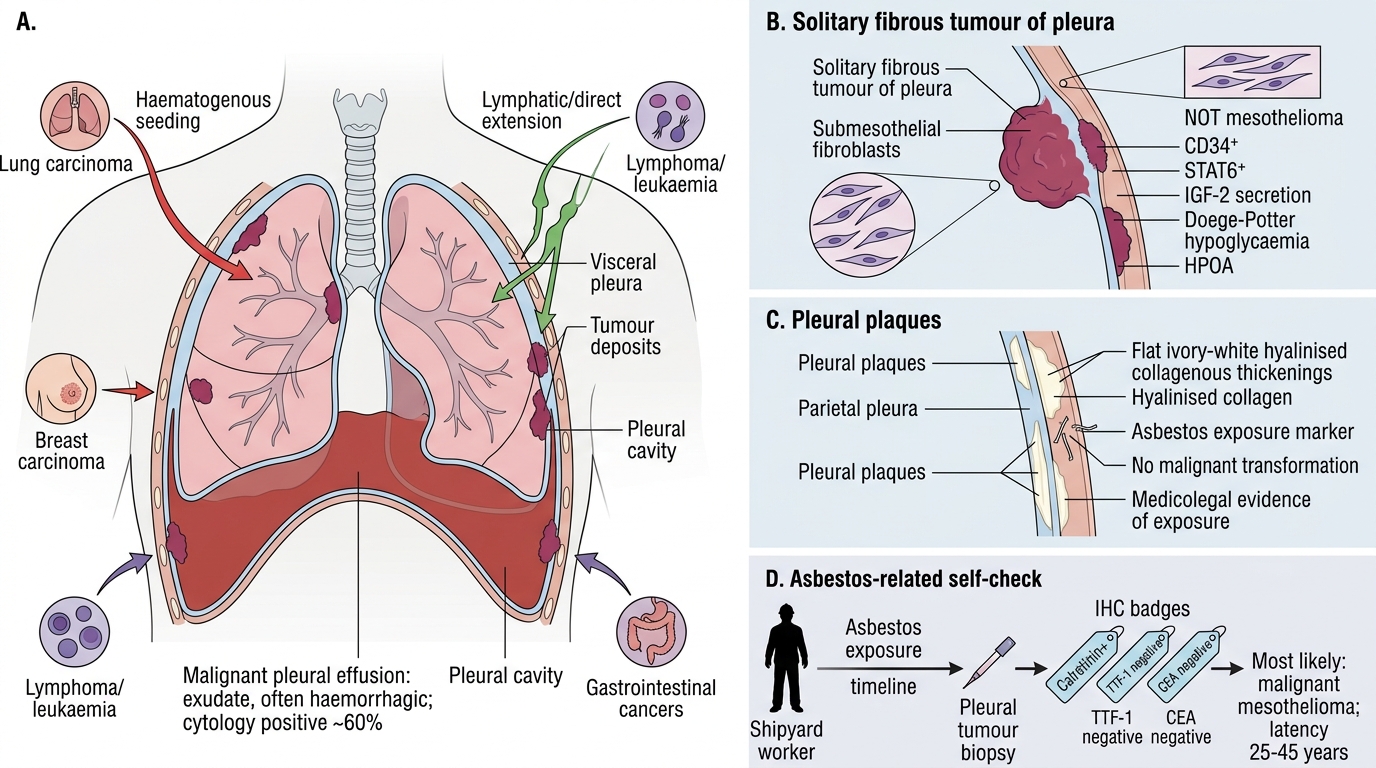
Other Pleural Tumours and Pleural Metastases
Pleural metastases — the commonest pleural malignancy:
• Secondary involvement of the pleura is far more common than primary mesothelioma.
• Commonest primary sources: lung carcinoma (any subtype), breast carcinoma, lymphoma/leukaemia, gastrointestinal cancers.
• Mechanism: haematogenous seeding of visceral pleura or direct lymphatic extension to parietal pleura.
• Results in malignant pleural effusion — exudate (Light's criteria), often haemorrhagic; cytology positive in ~60%.
Solitary fibrous tumour of the pleura (SFTP):
• Rare; arises from submesothelial fibroblasts (NOT mesothelial cells — hence NOT a mesothelioma).
• Usually benign; pedunculated; CD34-positive, STAT6-positive on IHC.
• Associated with hypoglycaemia (Doege-Potter syndrome — IGF-2 secretion) and HPOA.
Pleural plaques:
• Hyalinised collagenous thickenings on parietal pleura; asbestos exposure marker.
• Do NOT undergo malignant transformation; do NOT cause mesothelioma directly.
• Important as medicolegal evidence of exposure in compensation claims.
SELF-CHECK
Pleural biopsy from a 65-year-old shipyard worker (30 years' asbestos exposure; no smoking) shows a tumour. IHC: calretinin-positive, TTF-1 negative, CEA negative. What is the MOST LIKELY diagnosis and its typical latency from exposure?
A. Metastatic lung adenocarcinoma; 5–10 year latency
B. Malignant mesothelioma; 25–45 year latency
C. Squamous cell carcinoma; 20–25 year latency
D. Solitary fibrous tumour; no asbestos association
Reveal Answer
Answer: B. Malignant mesothelioma; 25–45 year latency
Calretinin-positive, TTF-1-negative, CEA-negative IHC profile is characteristic of malignant mesothelioma. Asbestos (especially amphibole fibres) is the dominant aetiological factor, and the hallmark of mesothelioma is its long latency of 25–45 years from first exposure. Metastatic adenocarcinoma would be TTF-1/CEA-positive. Squamous cell carcinoma typically arises centrally in the bronchus, not the pleura. SFTP has no asbestos association and is usually benign.