Page 9 of 16
PA33.4 | Common Skin Tumors & Morphology — SDL Guide (Part 4)
Master Recognition Table — Skin Tumors
Use this table as your final revision checklist before the practical exam.
| Tumor | Clinical Clue | Key Histology | Behavior |
|---|---|---|---|
| Seborrheic keratosis | Stuck-on, warty, dark plaque | Basaloid cells + horn cysts + flat lower border | Benign |
| Acrochordon | Soft, pedunculated, flesh-coloured neck papule | Fibrovascular core + normal squamous epithelium | Benign |
| Epidermal inclusion cyst | Smooth cyst with punctum; rupture → inflammation | Squamous epithelium with granular layer + laminated keratin | Benign |
| Acanthosis nigricans | Velvety, dark flexural skin | Papillomatosis + mild hyperkeratosis | Marker; rule out internal malignancy |
| Cylindroma | Scalp ('turban tumor' if multiple) | Jigsaw-puzzle basaloid nests with hyaline sheaths | Benign |
| Syringoma | Multiple eyelid papules | Tadpole (comma-shaped) ducts in fibrous stroma | Benign |
| Pilomatricoma | Firm, calcified nodule in children | Basaloid + ghost cells + calcification | Benign |
| Junctional nevus | Flat, uniformly pigmented macule | Nests at DEJ only | Benign |
| Compound nevus | Slightly raised pigmented papule | Nests at DEJ + dermis; maturation present | Benign |
| Intradermal nevus | Dome-shaped, flesh-coloured papule | Nests in dermis only; maturation present | Benign |
| Dysplastic nevus | >6 mm, variegated, irregular border | Bridging nests, lentiginous growth, lamellar fibroplasia | Potential precursor |
| Actinic keratosis | Sandpaper plaque, sun-exposed skin | Basal dysplasia only; solar elastosis | Premalignant |
| Bowen disease | Scaly erythematous plaque | Full-thickness atypia; intact BM | Premalignant (SCC in situ) |
| BCC | Pearly nodule, rolled border, telangiectasia | Basaloid nests + peripheral palisading + retraction cleft | Locally destructive; rare mets |
| SCC | Firm ulcerated plaque, sun-exposed | Keratin pearls + intercellular bridges + dermal invasion | Malignant; 5–10% mets |
| Melanoma | ABCDE; variegated color | Pagetoid spread + atypical melanocytes + loss of maturation | Highly malignant |
| Dermatofibroma | Firm brown nodule, lower leg; dimple sign | Storiform spindle cells + epidermal hyperplasia + trapped collagen | Benign |
| Cutaneous metastasis | Firm dermal nodule(s), no epidermal connection | Primary histotype in dermis, epidermis spared | Malignant (secondary) |
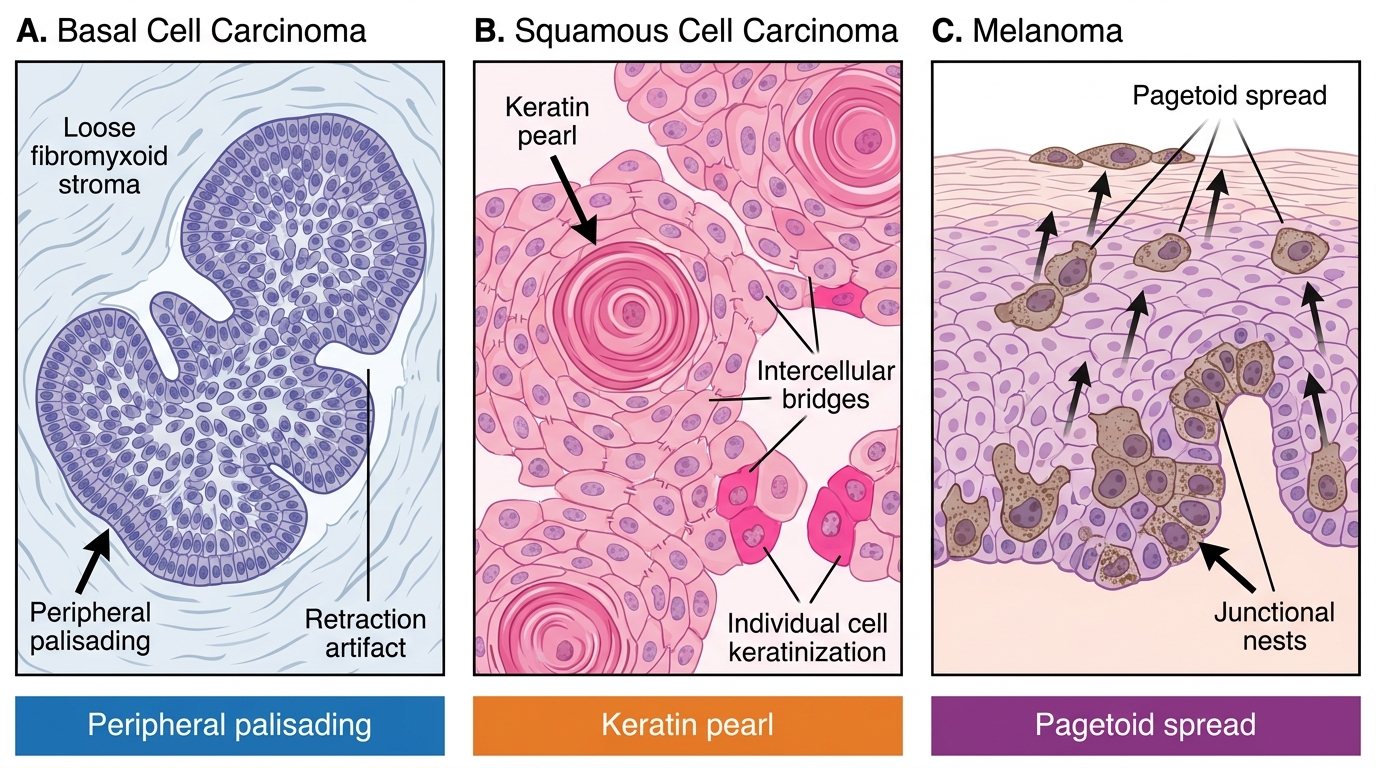
Histological Hallmarks of Common Skin Malignancies: BCC, SCC, and Melanoma
SELF-CHECK
A 45-year-old woman has a 1 cm firm brown nodule on her right leg. Lateral pressure on the nodule causes it to dimple inward. Biopsy shows spindle cells in a storiform pattern with overlying epidermal hyperplasia. The BEST diagnosis is:
A. Nodular melanoma
B. Dermatofibroma
C. Squamous cell carcinoma
D. Epidermal inclusion cyst
Reveal Answer
Answer: B. Dermatofibroma
The 'dimple sign' (Fitzpatrick's sign) on lateral compression is the classic clinical feature of dermatofibroma. Histologically, storiform spindle cells + overlying epidermal hyperplasia + trapped collagen confirms the diagnosis. Melanoma shows atypical melanocytes with pagetoid spread; SCC shows keratin pearls; epidermal cyst shows a cystic space lined by squamous epithelium.