Page 8 of 16
PA33.4 | Common Skin Tumors & Morphology — SDL Guide (Part 3)
Squamous Cell Carcinoma
Squamous cell carcinoma (SCC) of the skin is the second most common skin cancer. Unlike BCC, it has real metastatic potential (5–10% overall, higher for lesions arising in scars, chronic ulcers, or mucosae). It arises from epidermal keratinocytes.
Pathogenesis: UV-induced TP53 mutation (also HPV in genital/mucosal SCC). Sequence: normal skin → AK (SCC in situ/Bowen) → invasive SCC.
Clinical features: Firm, fleshy, erythematous papule or plaque that may ulcerate, crust, or form a cutaneous horn. Sun-exposed sites (lip, ear, dorsum of hand) are classic. Marjolin's ulcer = SCC arising in a chronic scar or burn — higher metastatic risk.
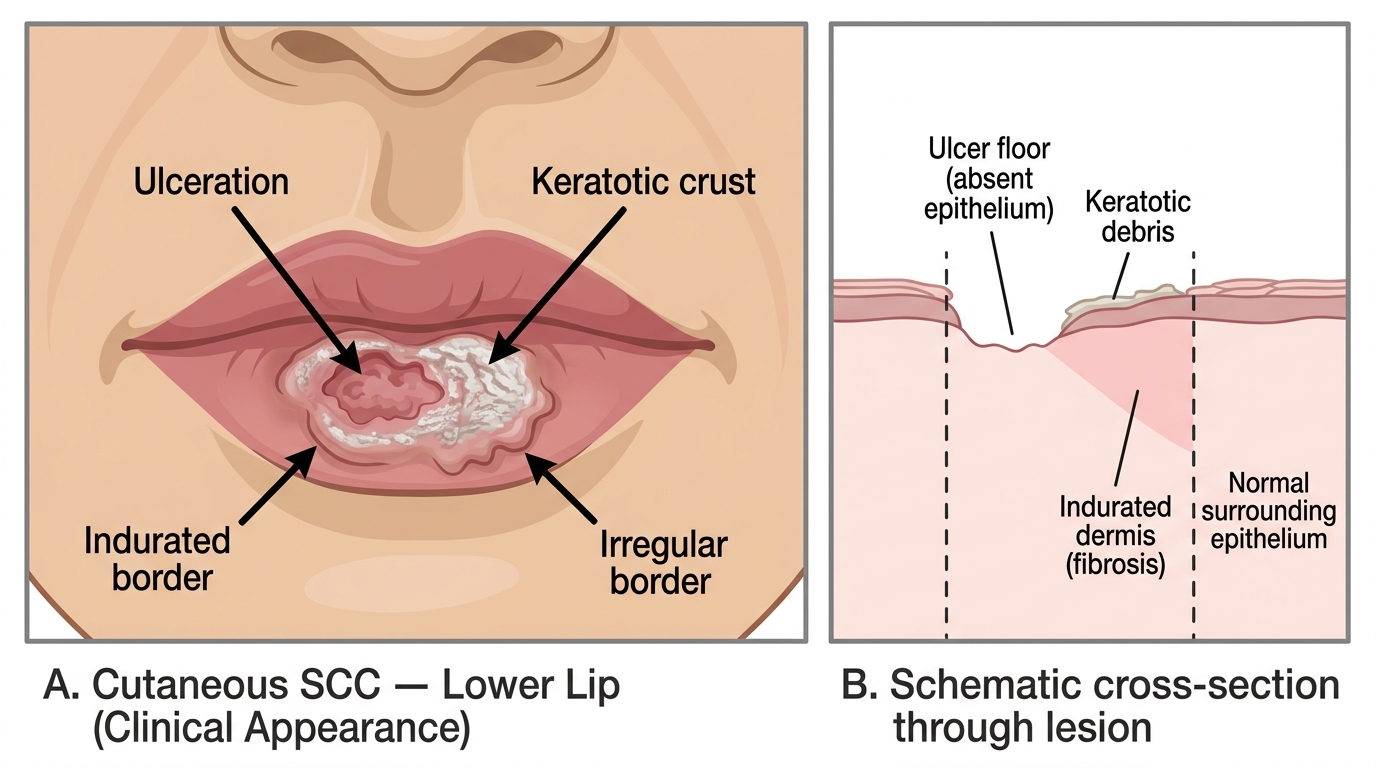
Cutaneous SCC of the Lower Lip — Clinical Features and Lesion Cross-Section
Histological features:
1. Invasive nests and cords of atypical squamous cells breaching the basement membrane into the dermis (this breach defines invasion; contrast with Bowen disease).
2. Dyskeratosis: individual cell keratinization (eosinophilic cells with dense cytoplasm).
3. Keratin pearls (squamous eddies): concentric whorls of keratinizing cells — the hallmark of well-differentiated SCC.
4. Intercellular bridges (desmosomes) visible between cells.
5. Mitoses, including atypical mitoses.
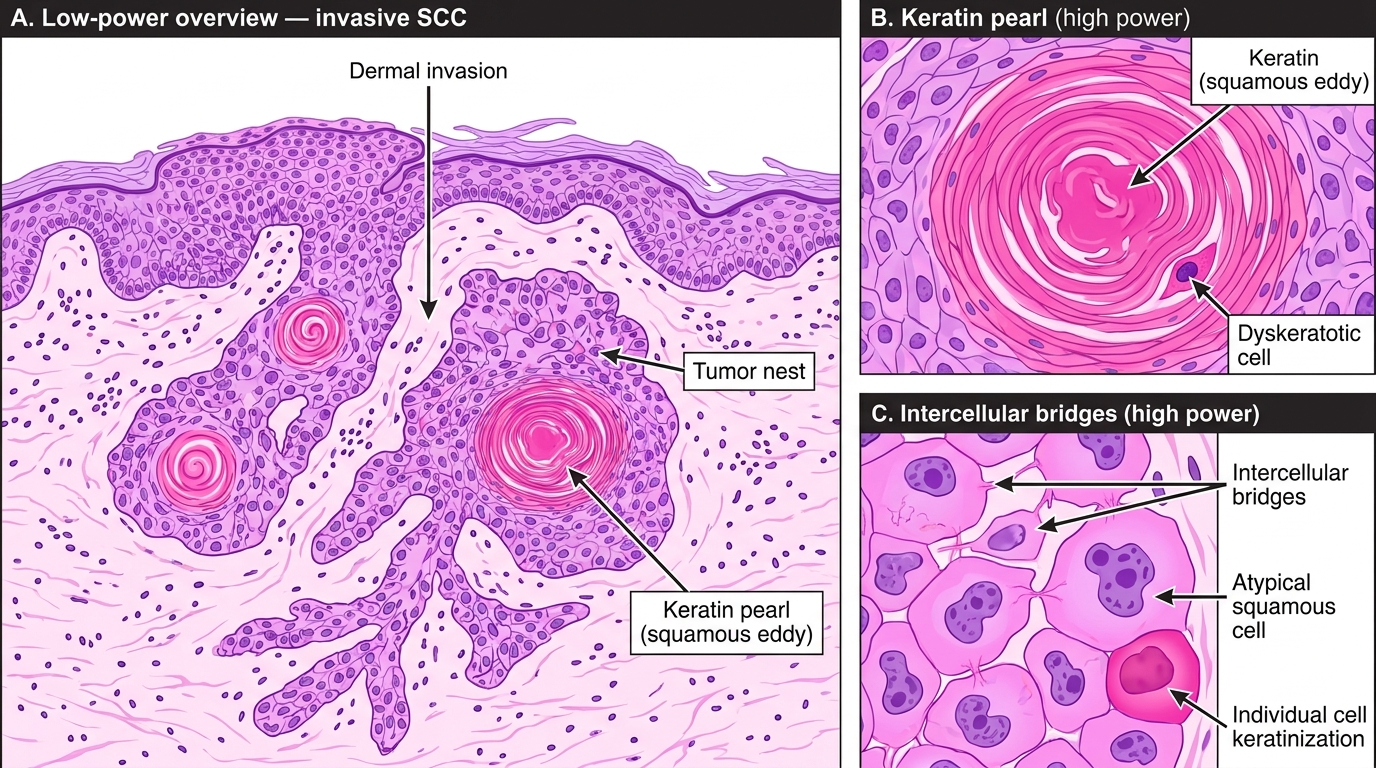
Histology of Well-Differentiated Squamous Cell Carcinoma (H&E)
Grading: Well-differentiated = prominent keratin pearls; moderately differentiated = some keratinization; poorly differentiated = minimal keratinization, marked pleomorphism.
Melanoma
Melanoma is the most dangerous skin tumor — despite representing only 4% of skin cancers, it accounts for >75% of skin cancer deaths. It arises from melanocytes and has high metastatic potential.
Pathogenesis: UV-driven BRAF mutation (in ~60% of cases, the V600E hotspot) is the initiating event for most cutaneous melanomas. Loss of CDKN2A (p16) drives progression. Dysplastic nevi are precursors in a subset.
Clinical recognition (ABCDE rule):
- Asymmetry
- Border — irregular, notched
- Color — variegated (multiple shades of brown, black, red, white, blue)
- Diameter — >6 mm
- Evolution — changing lesion
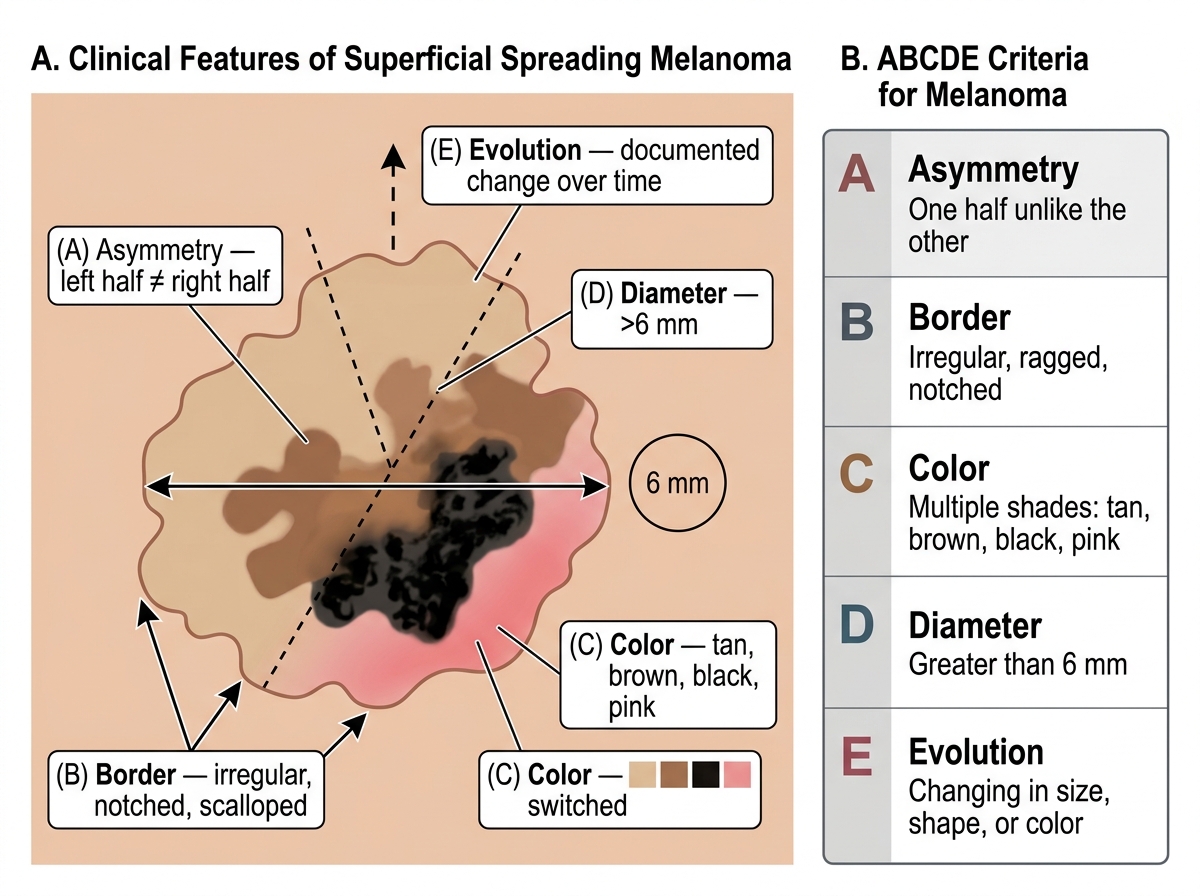
ABCDE Features of Superficial Spreading Melanoma
Major subtypes:
- Superficial spreading melanoma (70%): most common; radial growth phase before vertical growth.
- Nodular melanoma (15–30%): predominantly vertical growth from the start; worst prognosis.
- Lentigo maligna melanoma: on sun-damaged facial skin of elderly; slow radial growth phase.
- Acral lentiginous melanoma: palms, soles, subungual; most common in dark-skinned populations.
Histological features:
1. Atypical melanocytes at the DEJ and ascending into the epidermis (pagetoid spread — single cells or nests within the upper epidermis).
2. Vertical growth phase: invasion into the dermis with large, pleomorphic melanocytes and prominent nucleoli.
3. Loss of maturation in the deep component (deep cells remain large).
4. Mitoses in the dermis.
5. Tumour-infiltrating lymphocytes (TILs) brisk or absent.
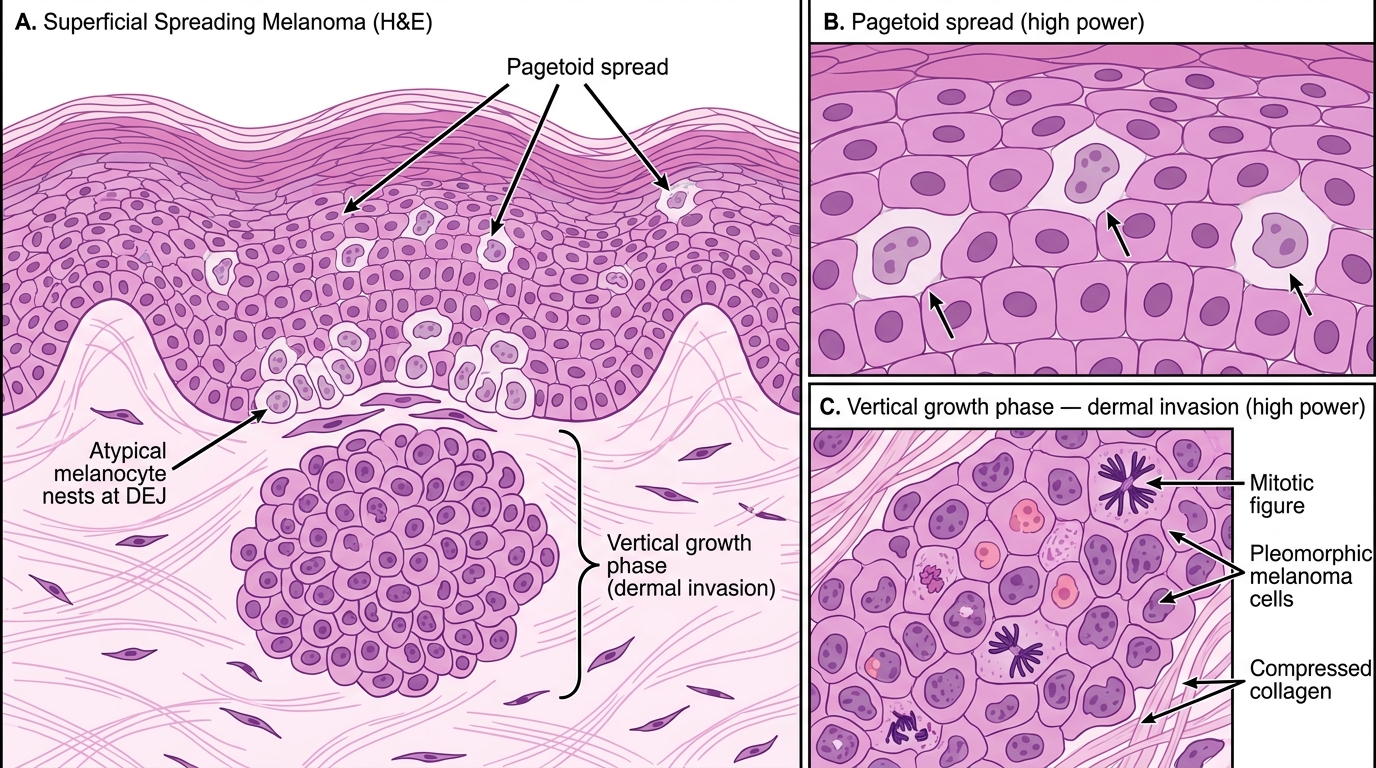
Histology of Superficial Spreading Melanoma (H&E)
Breslow thickness: The single most important prognostic factor — measured in millimeters from the top of the granular layer to the deepest invasive cell. ≤1 mm = excellent prognosis; >4 mm = high risk of systemic spread.
CLINICAL PEARL
BCC vs SCC vs Melanoma — the three-question shortcut for the practical exam:
- Is there peripheral palisading + retraction cleft? → BCC.
- Are there keratin pearls + intercellular bridges + basement membrane breach? → SCC.
- Is there pagetoid spread + pleomorphic melanocytes + loss of maturation? → Melanoma.
Never forget: BCC almost never metastasizes; SCC metastasizes in ~5–10%; Melanoma is highly aggressive. Getting the diagnosis right changes management entirely.
Dermatofibroma and Cutaneous Metastases
Dermatofibroma (fibrous histiocytoma) is a common, benign dermal nodule found predominantly on the lower legs of young to middle-aged women. Its exact nature (reactive vs neoplastic) is debated.
Clinical features: Firm, tan-brown, slightly raised nodule that dimples inward on lateral compression (Fitzpatrick's dimple sign) — a useful bedside test.
Histological features:
1. Proliferation of spindle cells (fibroblasts and histiocytes) in the dermis, arranged in a storiform (cartwheel) pattern.
2. The overlying epidermis is hyperplastic with downward extension into the dermis ("induction" of the overlying epidermis).
3. Siderophages (hemosiderin-laden macrophages) are often present.
4. The lesion is poorly circumscribed and blends with surrounding dermal collagen (trapping of collagen bundles at the periphery).
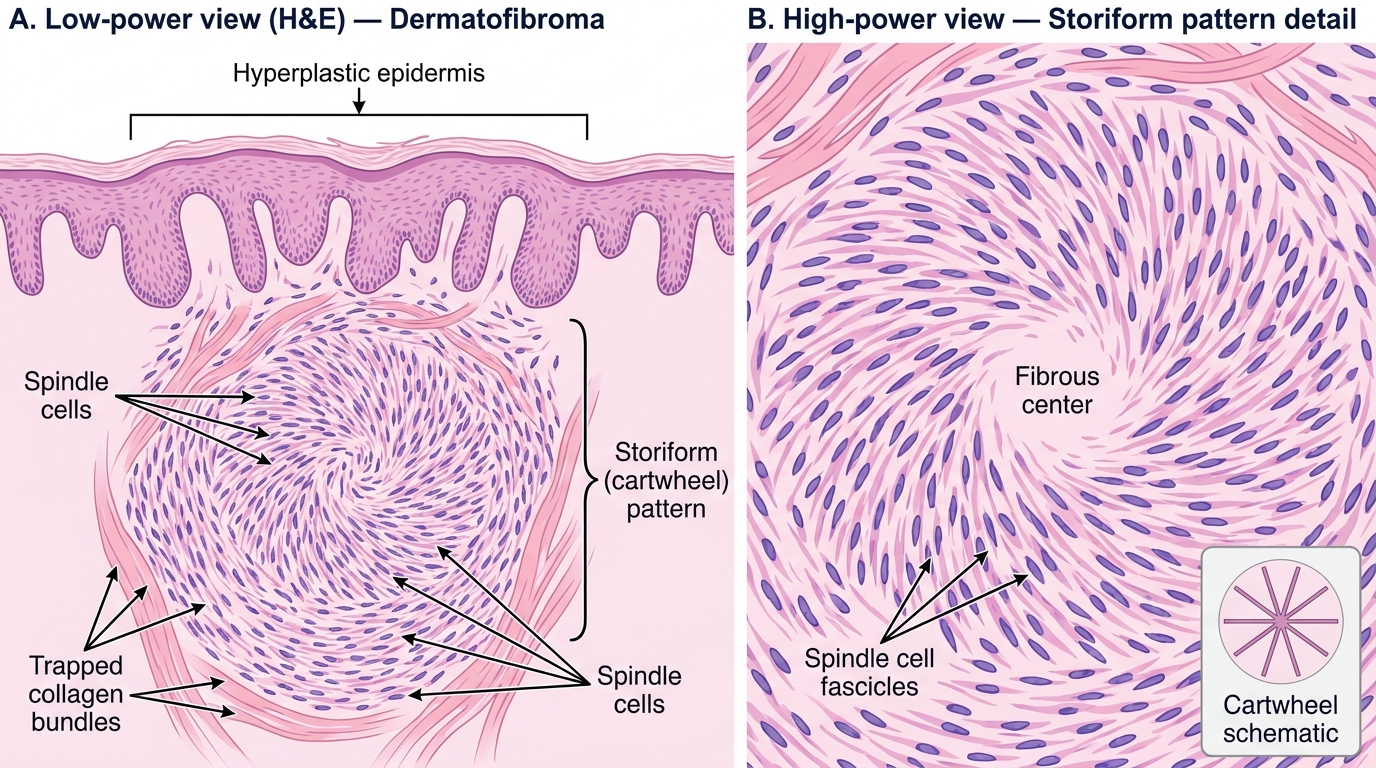
Dermatofibroma (Fibrous Histiocytoma) — H&E Histology: Storiform Pattern
Cutaneous metastases are skin deposits from internal malignancies. They appear as firm, non-tender, rapidly growing dermal or subcutaneous nodules, often multiple.
Common primary sources:
- Women: breast (most common), colon, ovary
- Men: lung (most common), colon, kidney
Special patterns:
- Sister Mary Joseph nodule: umbilical metastasis from GI or pelvic cancer — an ominous sign of peritoneal spread.
- Carcinoma en cuirasse: diffuse skin induration from breast cancer permeating the dermal lymphatics — resembles a leather breastplate.
Histology: The skin biopsy shows adenocarcinoma cells (or whatever the primary histotype) in the dermis, without connection to the overlying epidermis — this epidermal sparing distinguishes metastasis from a primary skin adnexal tumor.