Page 7 of 16
PA33.4 | Common Skin Tumors & Morphology — SDL Guide (Part 2)
Melanocytic Nevi — Junctional, Compound, and Intradermal
Melanocytic nevi ('moles') are benign neoplasms of nevus cells — modified melanocytes that grow in nests. The three-stage classification reflects a proposed migration of nevus cells from the epidermis into the dermis as the lesion matures.
The nevus maturation sequence:
- Junctional nevus — nevus cell nests confined to the dermo-epidermal junction (DEJ). Clinically: flat, uniformly pigmented brown macule. Histologically: nests of nevus cells at the DEJ only, without intradermal component.
- Compound nevus — nests at the DEJ and in the dermis. Clinically: slightly raised, pigmented papule. This is the most common type.
- Intradermal nevus — nests entirely within the dermis, no junctional component. Clinically: dome-shaped, flesh-coloured or lightly pigmented papule, often pedunculated. Histologically: upper dermal nests of large cells, lower dermal cells become smaller and spindled (maturation — an important feature distinguishing benign from malignant).
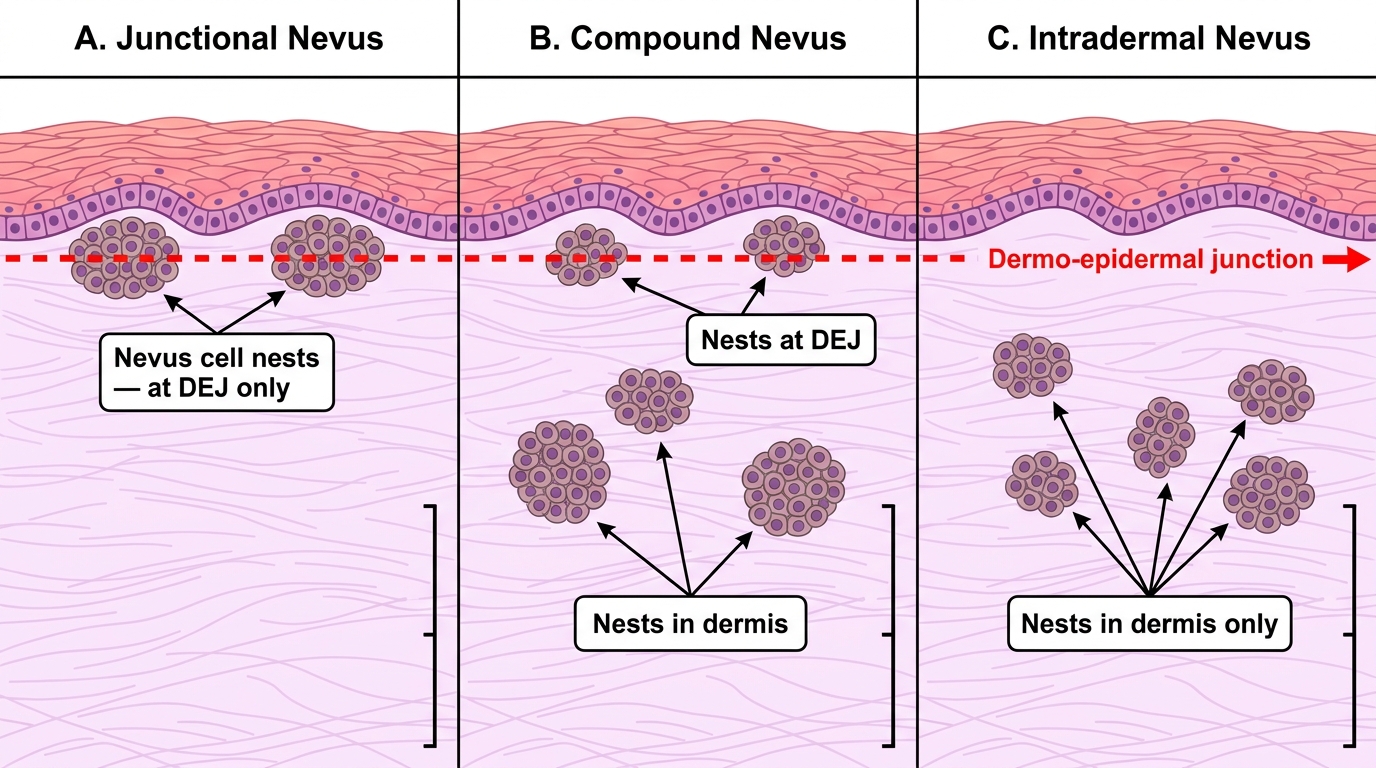
Melanocytic Nevi — Histological Classification (H&E)
Maturation is the key concept: in benign nevi, the deeper the cells go, the smaller they become (neuroid differentiation). Loss of maturation (deep cells remain large) is a feature of melanoma.
Dysplastic (atypical/Clark's) nevus is a clinically and histologically atypical nevus that may be a melanoma precursor. Clinical (ABCDE clues): Asymmetry, irregular Border, variegated Color, Diameter >6 mm, Evolution. Histologically: architectural disorder (bridging of nests, lentiginous growth), cytological atypia, a fibroplastic stroma, and a sparse lymphocytic infiltrate.
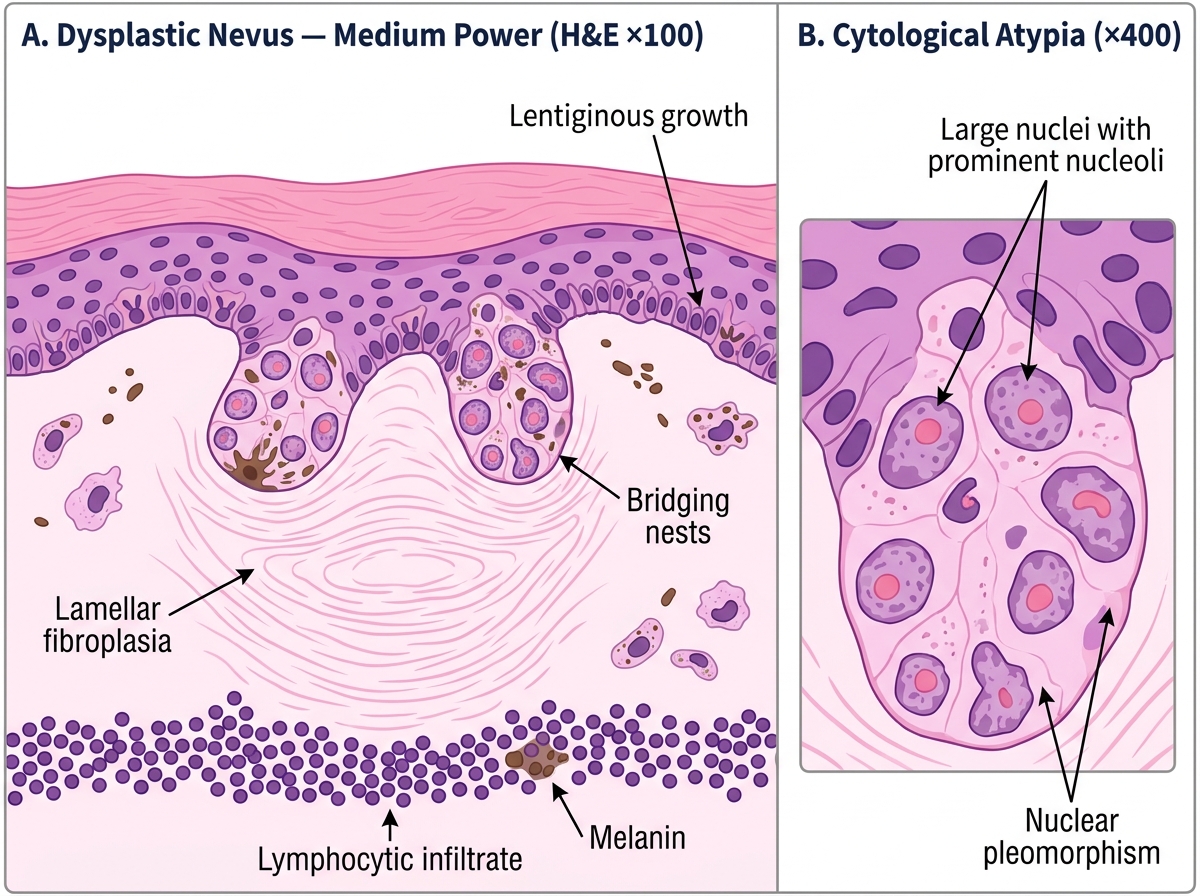
Histology of Dysplastic Nevus (H&E) — Architectural and Cytological Features
CLINICAL PEARL
Familial dysplastic nevus syndrome (FAMS/FAMM): Patients with >50 dysplastic nevi and a first-degree relative with melanoma have a lifetime melanoma risk approaching 100%. The dysplastic nevus itself rarely transforms — but it flags a genetic background (CDKN2A/p16 mutations) that makes any melanocyte in the body transform-prone. Full-body skin surveillance every 6 months is mandatory.
Premalignant Lesions — Actinic Keratosis and Bowen Disease
Actinic keratosis (AK) is a UV-induced intraepidermal dysplasia — the most common precancerous lesion of the skin. It progresses to invasive SCC in ~8–20% of cases if untreated.
Clinical features: Rough, scaly, erythematous macule or thin plaque on sun-exposed skin (face, scalp, dorsum of hands) in older, fair-skinned individuals. The 'sandpaper' texture on palpation is a useful clinical clue.
Histology:
- Dysplastic keratinocytes in the lower layers of the epidermis (sparing the upper layers and adnexal epithelium — important distinction from Bowen disease).
- Parakeratosis (nucleated cells in the stratum corneum) alternating with orthokeratosis.
- Solar elastosis in the dermis (thick, amorphous, blue-grey elastin on H&E — the hallmark of cumulative sun damage).
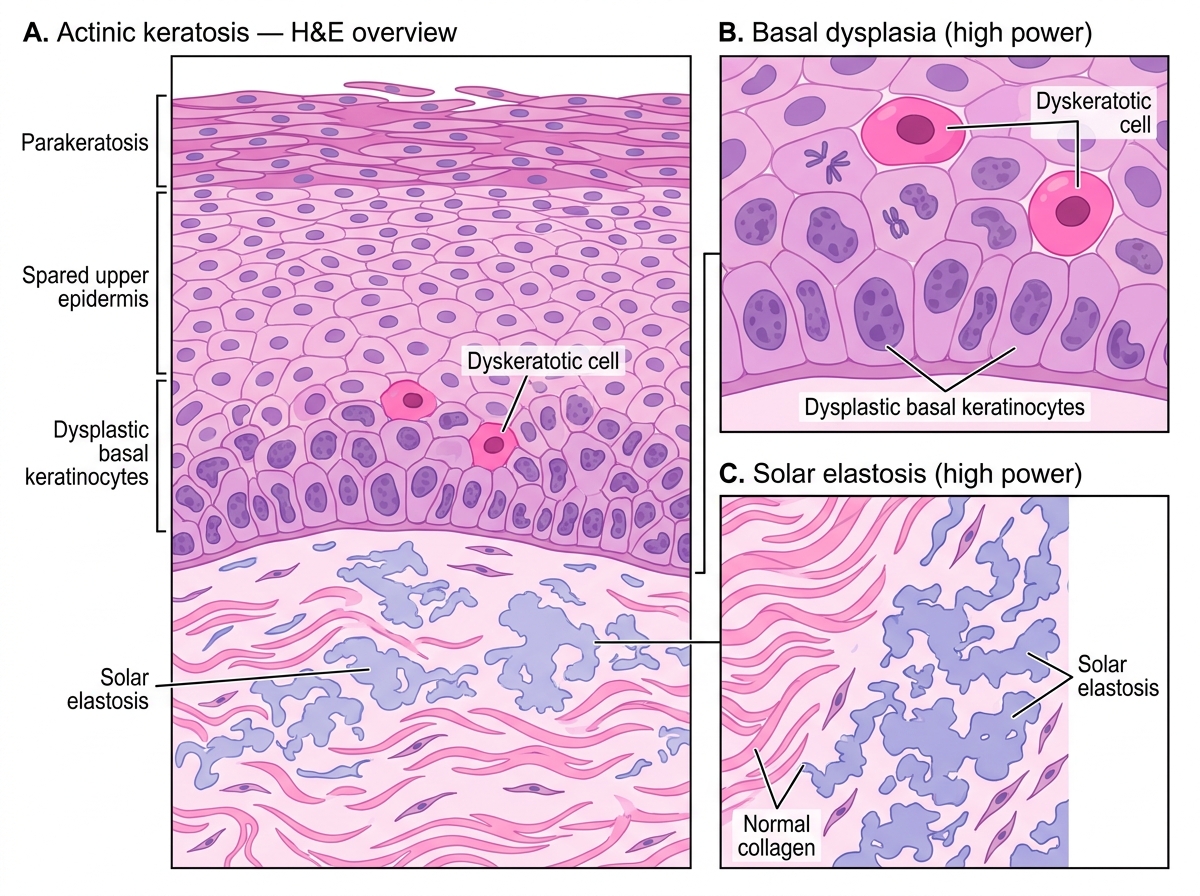
Histology of Actinic Keratosis (H&E)
Bowen disease (SCC in situ) is full-thickness epidermal dysplasia — the entire epidermis is replaced by atypical keratinocytes, but the basement membrane remains intact (no dermal invasion). Think of it as AK that has spread upward to involve the full thickness.
Clinical features: Sharply demarcated, scaly, erythematous plaque, often on the trunk or extremities, not necessarily sun-exposed.
Histology (the 'windswept' or 'wind-blown' pattern):
- Full-thickness epidermal atypia: dysplastic cells at all levels.
- Disordered maturation: loss of normal cell polarity ('windswept' appearance).
- Koilocyte-like cells and multinucleated keratinocytes possible.
- Intact basement membrane (the critical feature — invasion = SCC).
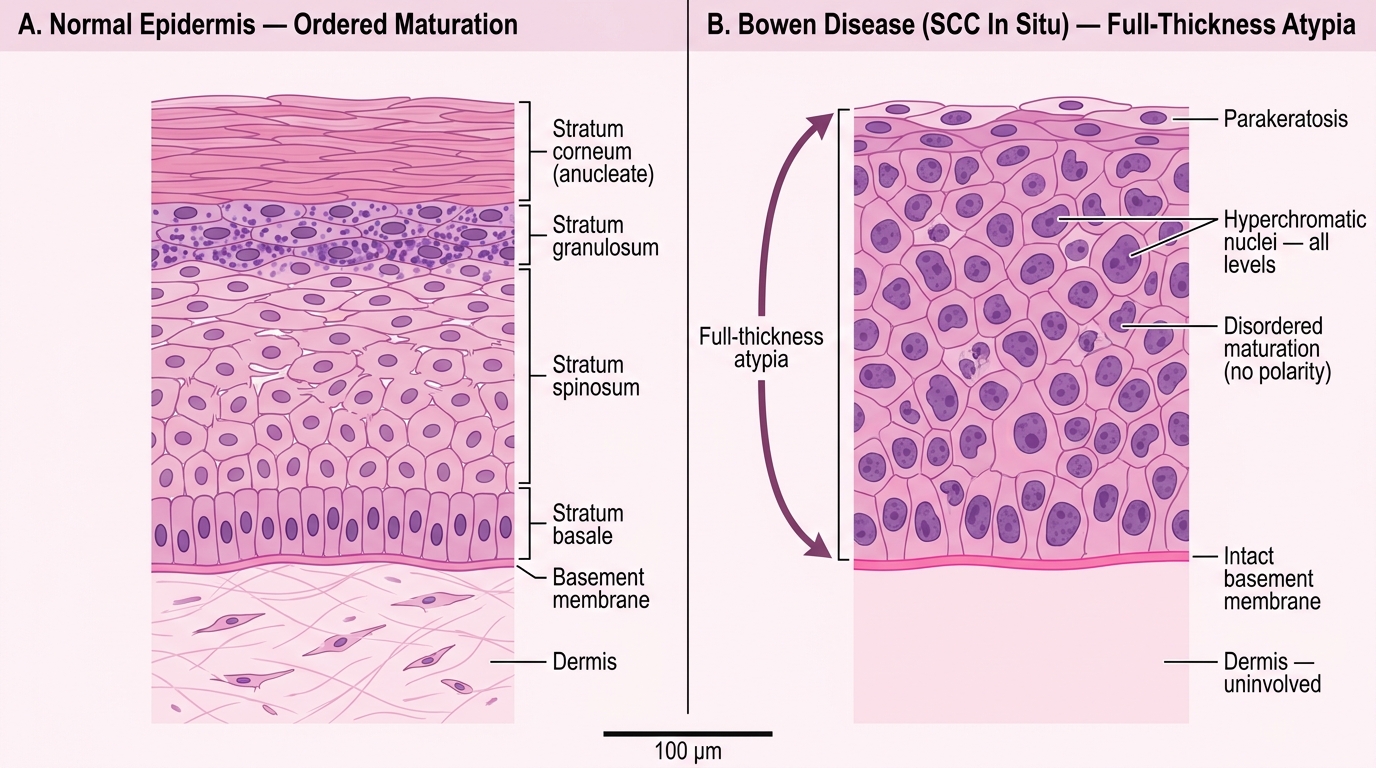
Bowen Disease (SCC In Situ): Histological Comparison with Normal Epidermis (H&E)
AK vs Bowen at a glance:
| Feature | Actinic Keratosis | Bowen Disease |
|---|---|---|
| Extent of dysplasia | Basal/parabasal layers | Full thickness |
| Adnexal epithelium | Spared | Involved |
| Sun exposure relationship | Strong | Variable |
| Progression risk to SCC | 8–20% | Higher |
Basal Cell Carcinoma
Basal cell carcinoma (BCC) is the most common cancer in humans (lifetime risk ~30% in fair-skinned populations). It arises from the basal layer of the epidermis and almost never metastasizes, but it is locally destructive.
Pathogenesis: UV-induced mutation of PTCH1 (patched-1) gene → unregulated Hedgehog signaling → sustained proliferation.
Clinical features (nodular BCC — the most common subtype): Pearly, translucent papule or nodule with telangiectatic vessels on the surface, with a rolled (everted) border and possible central ulceration ('rodent ulcer'). Almost exclusively on sun-exposed skin of the head and neck.
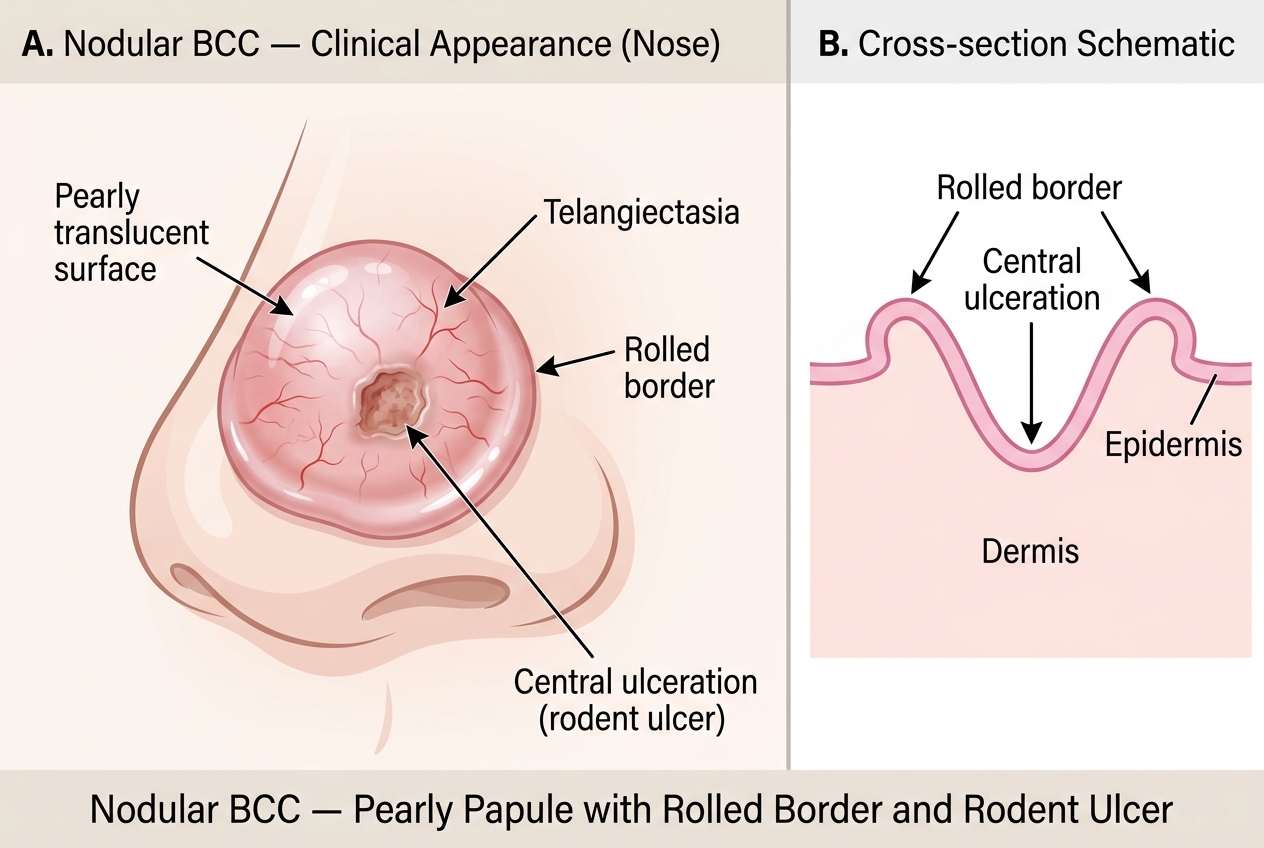
Nodular Basal Cell Carcinoma — Clinical Features and Cross-section
Histological features (key pattern):
1. Nests and cords of basaloid cells (small, dark nuclei, scant cytoplasm) extending from the epidermis into the dermis.
2. Peripheral palisading of cells at the edge of each nest (cells align like soldiers in a row).
3. Stromal retraction artifact: a cleft between the tumor nest and surrounding stroma (important — do not confuse with true invasion).
4. Myxoid/mucinous stroma.
5. Mitoses are present but apoptosis is also prominent.
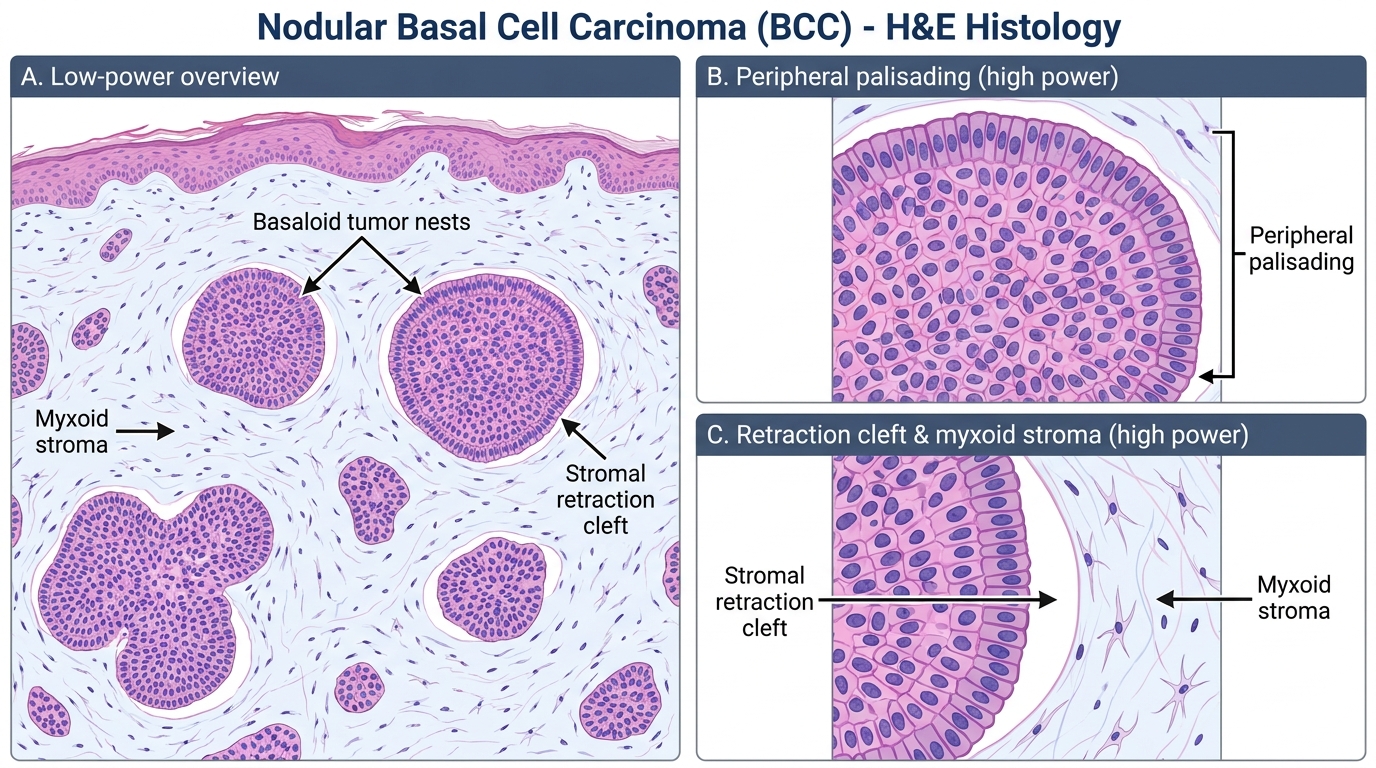
Nodular BCC — H&E Histology: Peripheral Palisading and Stromal Retraction Cleft
Subtypes in brief:
- Nodular BCC (most common): discrete nests, as above.
- Superficial BCC: buds of basaloid cells attached to the epidermis, spreading laterally.
- Morpheaform (sclerosing) BCC: thin cords of cells in a dense fibrous stroma — the most aggressive, highest recurrence rate.
SELF-CHECK
A biopsy from a pearly nodule on the nose shows nests of basaloid cells with peripheral palisading and a stromal retraction cleft. The patient is a 65-year-old farmer. The MOST likely diagnosis is:
A. Seborrheic keratosis
B. Squamous cell carcinoma
C. Basal cell carcinoma
D. Melanoma
Reveal Answer
Answer: C. Basal cell carcinoma
The triad of basaloid cells + peripheral palisading + stromal retraction cleft is pathognomonic for BCC. The clinical description (pearly nodule on sun-exposed skin, older patient) is classic nodular BCC. SK shows basaloid cells with horn cysts but no palisading; SCC shows keratinization and intercellular bridges; melanoma involves melanocytes.