Page 6 of 16
PA33.4 | Common Skin Tumors & Morphology — SDL Guide
Learning Objectives
- Identify and describe the gross and histological features of common benign epithelial skin tumors: seborrheic keratosis, acanthosis nigricans, acrochordon, and epidermal inclusion cyst.
- Describe the key histological features of selected adnexal tumors: cylindroma, syringoma, and pilomatricoma.
- Classify melanocytic nevi (junctional, compound, intradermal) and describe the distinguishing features of dysplastic nevi.
- Identify and distinguish the morphological features of premalignant and malignant skin lesions: actinic keratosis, Bowen disease, basal cell carcinoma, squamous cell carcinoma, and melanoma.
- Recognize dermatofibroma and explain its characteristic histological findings.
- Apply a systematic pattern-recognition approach to unknown skin biopsy slides in the practical examination.
INSTRUCTIONS
This SDL is your morphology practical companion. Work through each tumor group systematically — for every entity, study the clinical image first (what does the clinician see?), then the histological image (what does the pathologist see?). Build mental 'snapshots' of each pattern. Use the Master Recognition Table at the end to consolidate before your practical exam. Estimated reading time: 33 minutes.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch. 25 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 60-year-old retired farmer walks into your dermatology OPD. He has a warty, dark, 'stuck-on' plaque on his cheek (seborrheic keratosis), a pearly nodule on his nose (BCC), a dark irregular lesion on his forearm (melanoma until proven otherwise), and what looks like a flesh-coloured skin tag on his neck. Same organ — four completely different lesions. Your job in the practical exam is to distinguish them in seconds. This SDL builds exactly that skill.
WHY THIS MATTERS
Skin tumors appear in two high-stakes settings for you as a Year-2 student: (1) the practical exam slide or specimen tray, where you must name and describe the lesion within minutes; (2) the clinical wards, where missing a melanoma or mislabeling a BCC as a seborrheic keratosis has real consequences. NMC competency PA33.4 explicitly requires you to identify, distinguish, and describe — that three-word mandate structures this entire SDL.
RECALL
Before we begin, refresh your memory on three concepts from SDL1 (Skin Diseases — General Pathology):
- Epidermis layers: stratum basale → spinosum → granulosum → corneum. Tumors arise from specific layers.
- Melanocytes sit in the basal layer and are derived from neural crest; nevi and melanoma arise from them.
- UV radiation is the dominant environmental carcinogen for skin: causes cyclobutane pyrimidine dimers in DNA, drives AK → SCC and BCC.
If any of these feel unfamiliar, re-read SDL1 section on normal skin histology before continuing.
Benign Epithelial Tumors — Seborrheic Keratosis
Seborrheic keratosis (SK) is the most common benign epidermal tumor in adults over 50, and a perennial practical-exam slide. Despite the name it has no relationship to sebaceous glands or true keratosis; the term is entirely historical.
Clinical features: Well-circumscribed, tan-to-dark-brown, velvety or verrucous plaque with a characteristic 'stuck-on' appearance — as if you could peel it off with a fingernail. Predilection for the face, trunk, and extremities. Multiple lesions may erupt suddenly (sign of Leser-Trélat) in association with internal malignancy, though isolated SK is entirely benign.
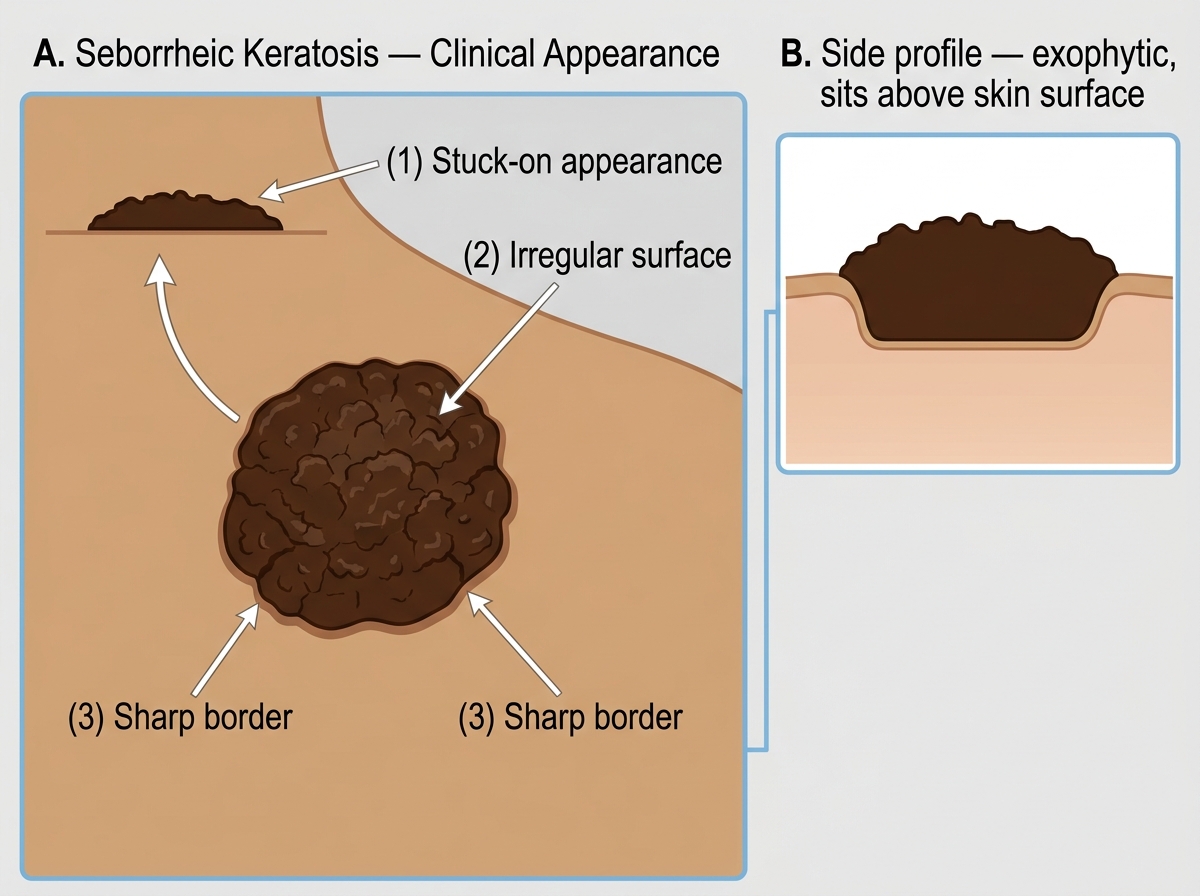
Seborrheic Keratosis — Clinical Features
Histological features (the high-yield pattern):
- Exophytic proliferation of bland basaloid keratinocytes — the cells look like stratum basale cells, with no atypia.
- Hyperkeratosis and acanthosis (thickened epidermis).
- Horn cysts (fully formed keratin pearls within the tumor mass) and pseudo-horn cysts (keratin-filled invaginations from the surface).
- A flat, sharp lower border (the lesion sits above a horizontal line).
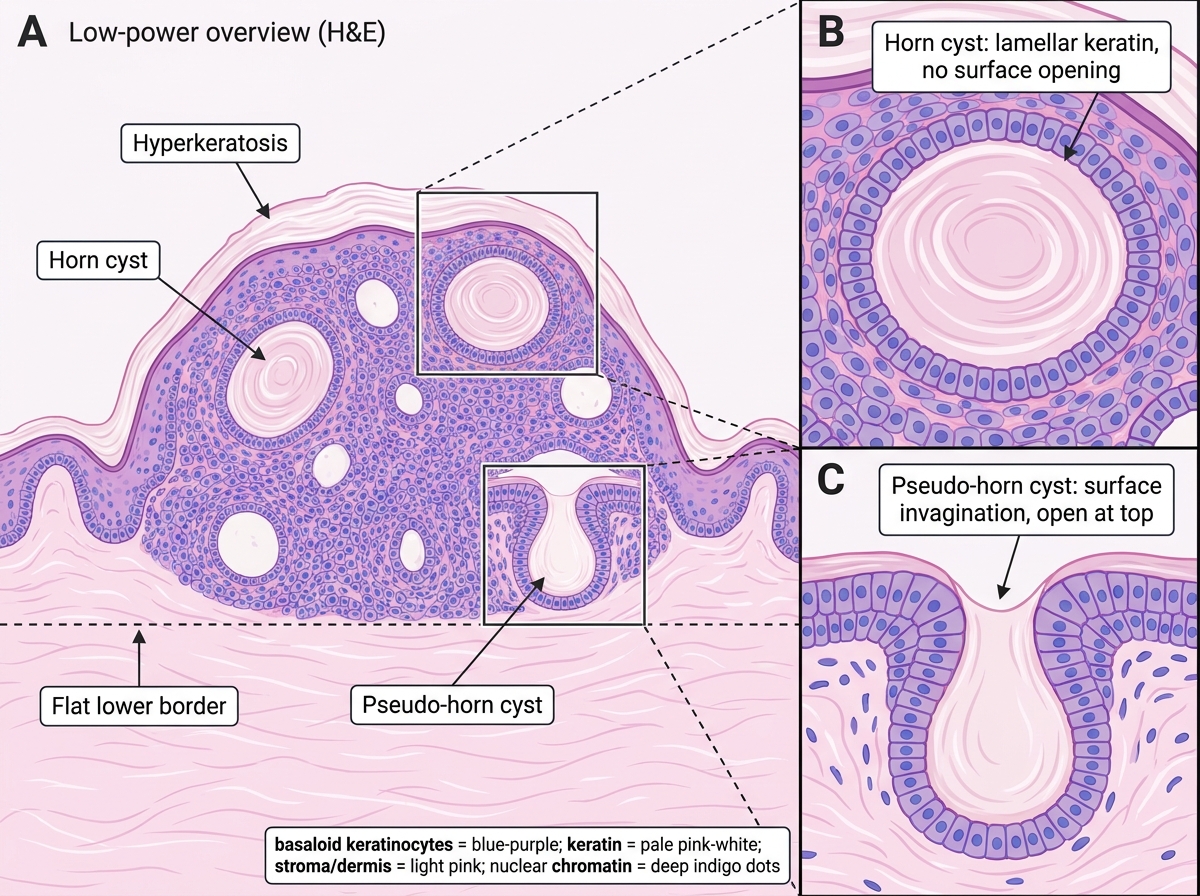
Seborrheic Keratosis — H&E Histology: Architectural and Cellular Features
Memory hook: SKs are stuck-on, basaloid, and full of horn cysts.
Benign Epithelial Tumors — Acanthosis Nigricans, Acrochordon, and Epidermal Inclusion Cyst
Acanthosis nigricans (AN) presents as velvety, hyperpigmented, thickened skin in flexural areas (axillae, neck, groin). Histology shows papillomatosis and mild hyperkeratosis — but minimal true acanthosis despite the name. Its significance is as a marker rather than a primary tumor: it is associated with insulin resistance/type 2 diabetes, obesity, and (in adults over 40) occult internal malignancy (especially gastric adenocarcinoma). A brief recognition is sufficient for the practical.
Acrochordon (skin tag / fibroepithelial polyp) is a pedunculated, flesh-coloured soft papule hanging from a thin stalk, found most commonly on the neck, axillae, and eyelids. Histology is unexciting: a fibrovascular core covered by normal squamous epithelium. No malignant potential. Clinically distinguished from a melanocytic lesion by its soft, pedunculated, skin-coloured nature.
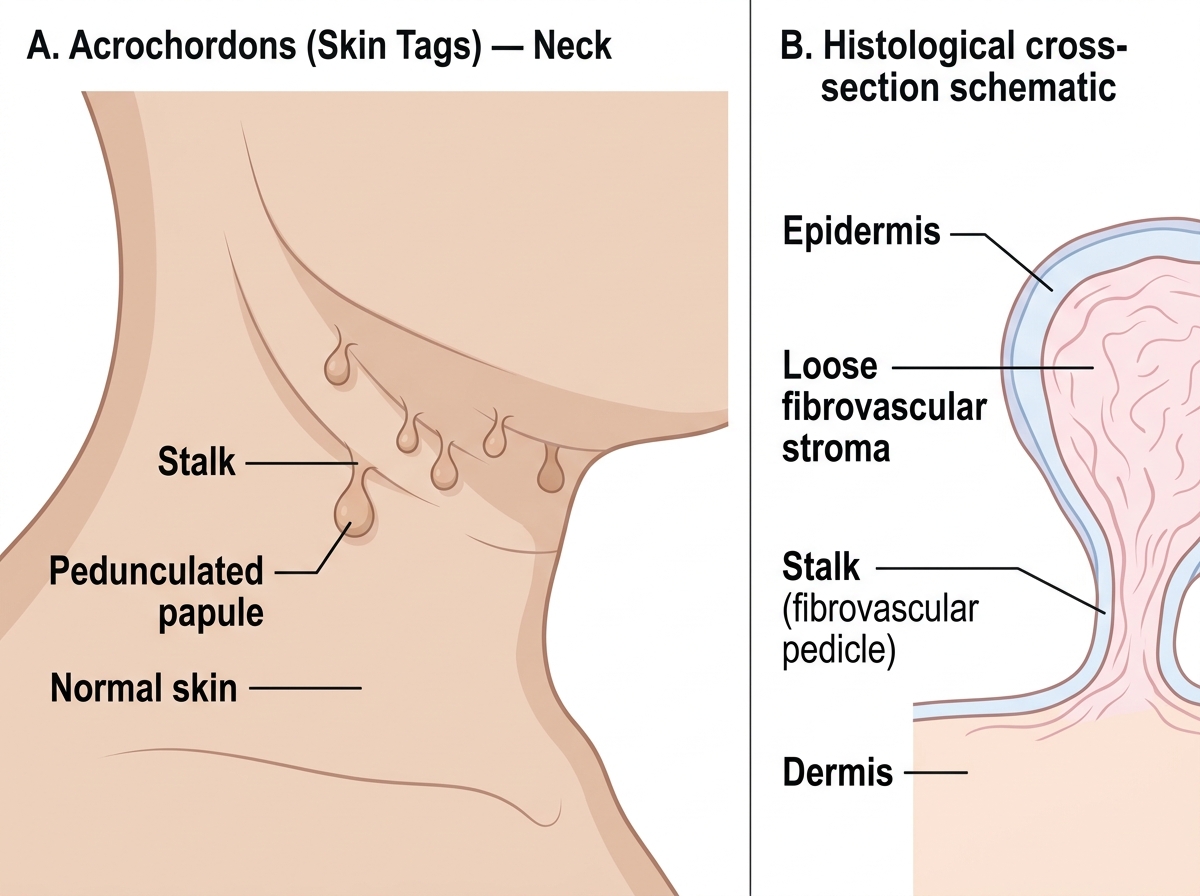
Acrochordons (Skin Tags) — Clinical Appearance and Structural Schematic
Epidermal inclusion cyst (epidermal/sebaceous cyst) is a common intradermal or subcutaneous cyst lined by true stratified squamous epithelium with a granular layer. The lumen contains laminated keratin. A central punctum is often visible clinically. On rupture, the extravasated keratin triggers a granulomatous foreign-body reaction with multinucleated giant cells — this is the source of the classic 'infected cyst' presentation.
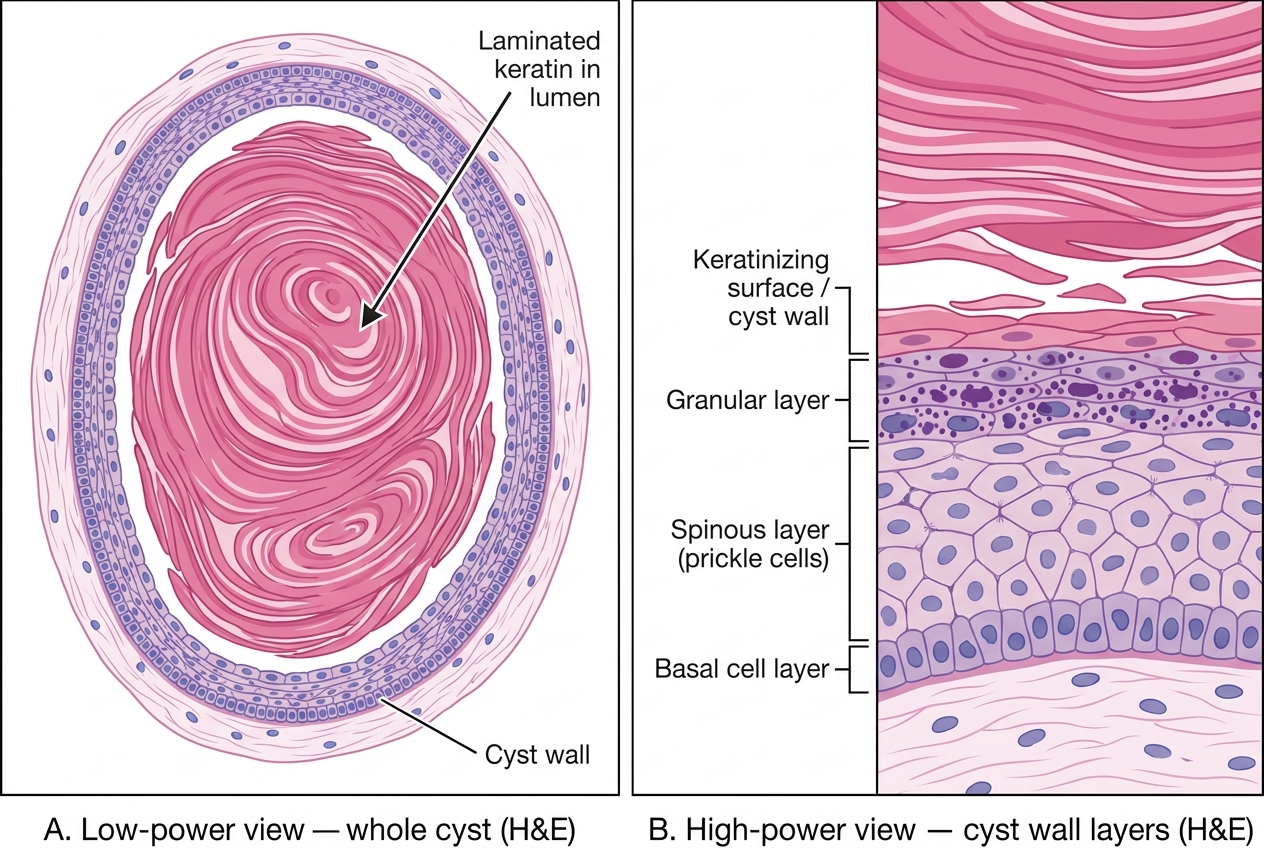
Epidermal Inclusion Cyst — H&E Histology (Low and High Power)
CLINICAL PEARL
Sign of Leser-Trélat — an abrupt eruption of multiple pruritic seborrheic keratoses is a rare paraneoplastic phenomenon; the associated tumor is most often gastric adenocarcinoma but also lymphomas. The same visceral malignancies also cause acanthosis nigricans. If you see both together on an exam MCQ, think GI malignancy.
Benign Adnexal (Appendageal) Tumors — Overview
Adnexal tumors arise from skin appendages: sweat glands (eccrine and apocrine), hair follicles, and sebaceous glands. A brief overview is sufficient at this level; detailed classification belongs to postgraduate dermatopathology.
| Tumor | Appendage of origin | Key histological clue |
|---|---|---|
| Cylindroma | Apocrine sweat gland | 'Jigsaw puzzle' islands of basaloid cells, each surrounded by a pink hyaline sheath |
| Syringoma | Eccrine sweat duct | Small ducts with a comma-shaped tail ('tadpole ducts') in a fibrous stroma |
| Pilomatricoma (calcifying epithelioma of Malherbe) | Hair follicle matrix | Basaloid cells + ghost/shadow cells + dystrophic calcification |
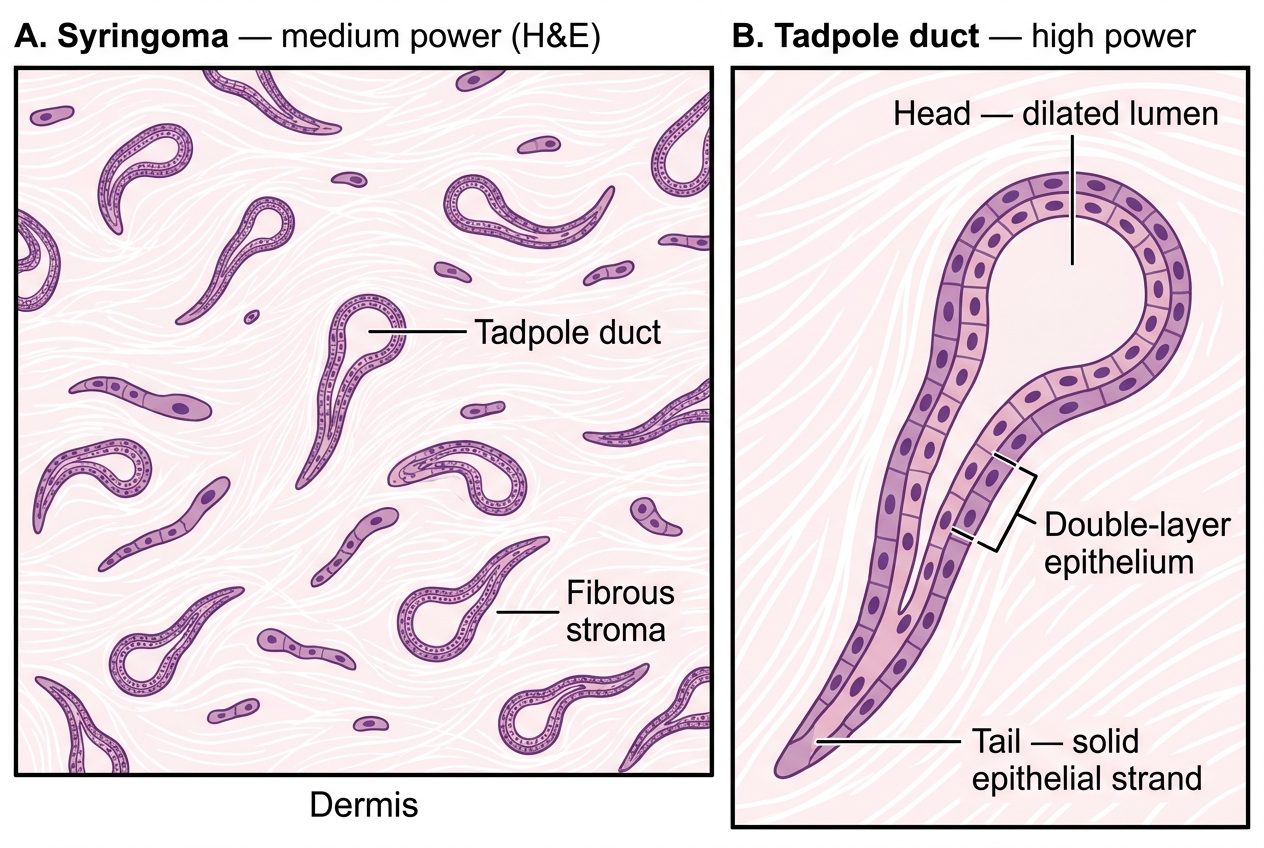
Syringoma — Histology (H&E): Tadpole Ducts in Fibrous Stroma
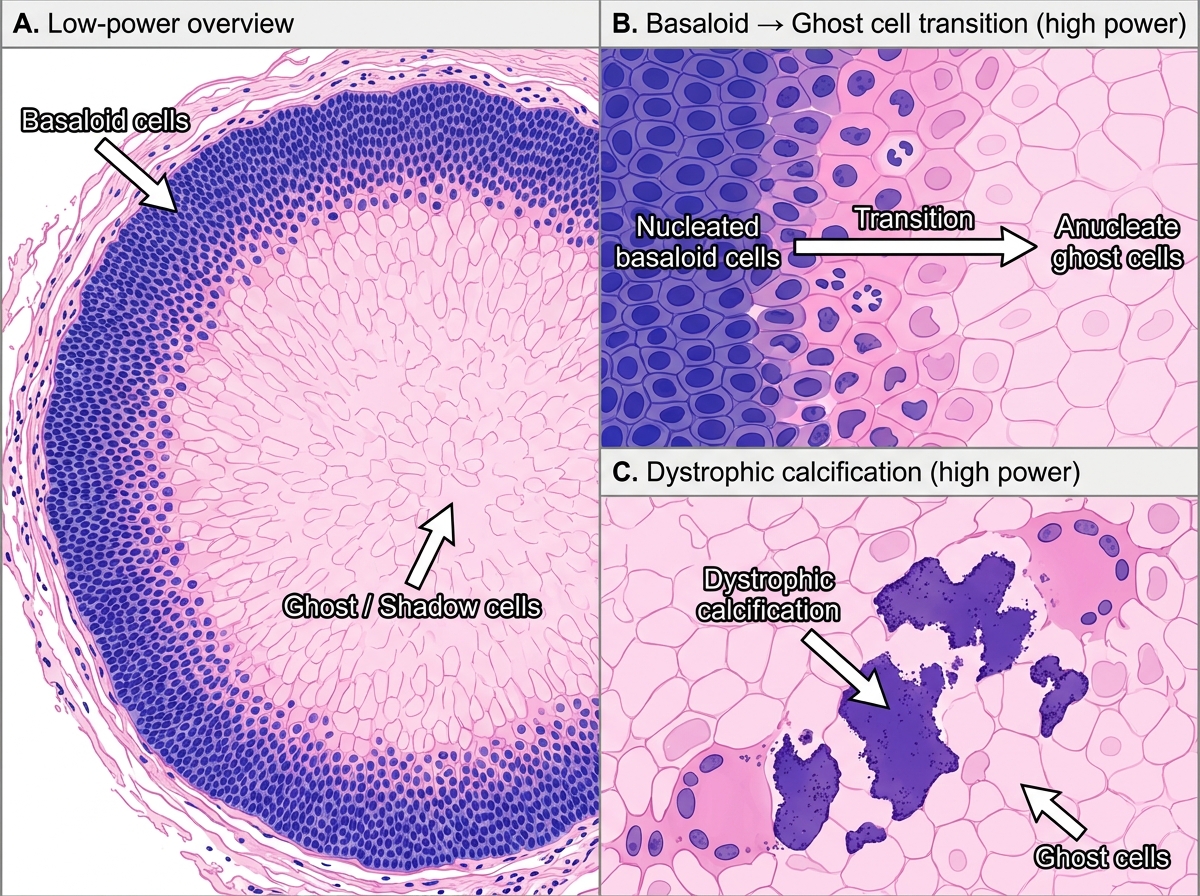
Pilomatricoma — H&E Histology: Basaloid Cells, Ghost/Shadow Cells, and Dystrophic Calcification
Practical tip: If a slide shows tadpole-shaped ductal structures → think syringoma. Jigsaw-puzzle basaloid islands with a pink rim → cylindroma. Ghost cells + calcification → pilomatricoma. These are pattern-recognition answers.
SELF-CHECK
A biopsy from a flesh-coloured eyelid papule in a 35-year-old woman shows small ductal structures with a comma-shaped tail embedded in a fibrous dermis. The most likely diagnosis is:
A. Cylindroma
B. Syringoma
C. Pilomatricoma
D. Seborrheic keratosis
Reveal Answer
Answer: B. Syringoma
Syringoma arises from eccrine sweat ducts and characteristically shows small comma-shaped ('tadpole') ducts in a fibrous dermis. It favors the lower eyelids of young women. Cylindroma shows jigsaw-puzzle basaloid islands with a hyaline sheath; pilomatricoma has ghost cells and calcification; SK has basaloid cells with horn cysts.