Page 5 of 16
PA33.1-3 | Skin Cancers: BCC, SCC & Melanoma — Summary & Reflection
REFLECT
Before you move to the summary, take two minutes to connect the dots across these three tumours:
- Pathogenesis comparison: BCC uses the Hedgehog/PTCH pathway. SCC uses TP53. Melanoma uses BRAF/RAS/MAPK. Why does this matter clinically? (Hint: it determines which targeted therapies work.)
- Metastatic behaviour: BCC never metastasises, SCC occasionally does, melanoma frequently does. What is it about melanocytes that makes them so prone to metastasis compared to keratinocytes? (Think about melanocytes' normal embryological origin — they are derived from the neural crest and are inherently migratory cells.)
- Acral lentiginous melanoma in Indian patients: This subtype is disproportionately common in people with darker skin, yet it arises in non-UV-exposed sites (palms, soles, subungual). What does this tell you about the aetiology? (It is not UV-driven — c-KIT mutations, mechanical trauma, and other factors are implicated.) How does this change your clinical approach?
- Practical skill: The ABCDE criteria are not perfect — nodular melanoma may be small and symmetric early on (it scores poorly on A, B, D). The 'Evolution' (E) criterion and 'ugly duckling' sign are therefore the most critical. How would you counsel a patient with multiple moles about what to watch for?
KEY TAKEAWAYS
Skin Cancers: BCC, SCC & Melanoma — Core Takeaways
Actinic Keratosis:
• Premalignant precursor to SCC; rough erythematous plaques on sun-exposed skin
• Histology: lower-layer atypia + solar elastosis + intact basement membrane
Squamous Cell Carcinoma (PA33.1):
• Risk: chronic UV, immunosuppression, HPV (16/18), chronic inflammation (Marjolin's ulcer)
• Pathogenesis: TP53 mutation (UV-induced pyrimidine dimers)
• Histology: keratin pearls, atypical squamous cells invading through basement membrane
• Bowen's disease = SCC in situ (full-thickness atypia, intact BM)
• Natural history: low metastatic rate (2–5%) — higher in high-risk features; lymph nodes first
Basal Cell Carcinoma (PA33.2):
• Most common human malignancy; risk: UV, fair skin, Gorlin syndrome
• Pathogenesis: PTCH1 inactivation → constitutive Hedgehog/SMO/GLI signalling
• Histology: basaloid nests, peripheral palisading, retraction cleft; morphoeic = desmoplastic cords
• Gross: pearly nodule, rolled edges, telangiectasias, central ulceration ('rodent ulcer')
• Natural history: locally destructive; metastasis <0.1% — targeted by vismodegib (SMO inhibitor)
Naevus vs Melanoma (PA33.3) — ABCDE:
• A = Asymmetry; B = Border irregular; C = Colour variation; D = Diameter >6 mm; E = Evolution (the most critical)
Melanoma (PA33.3):
• Risk: UV (intermittent/intense) + dysplastic naevi; darker populations → acral lentiginous subtype
• Pathogenesis: BRAF V600E (~50%) or NRAS → constitutive MAPK signalling
• Growth phases: radial (good prognosis) → vertical (poor prognosis)
• Prognosis: Breslow depth (mm from granular layer to deepest cell) is the key measurement
• Subtypes: SSM (most common), nodular (worst prognosis/time), lentigo maligna, acral lentiginous
• IHC: S100, HMB-45, Melan-A, SOX10
• Metastasis: lymphatic first → haematogenous (lung, liver, brain)
• Treatment: BRAF + MEK inhibitors (for BRAF-mutant); anti-PD-1/CTLA-4 immunotherapy
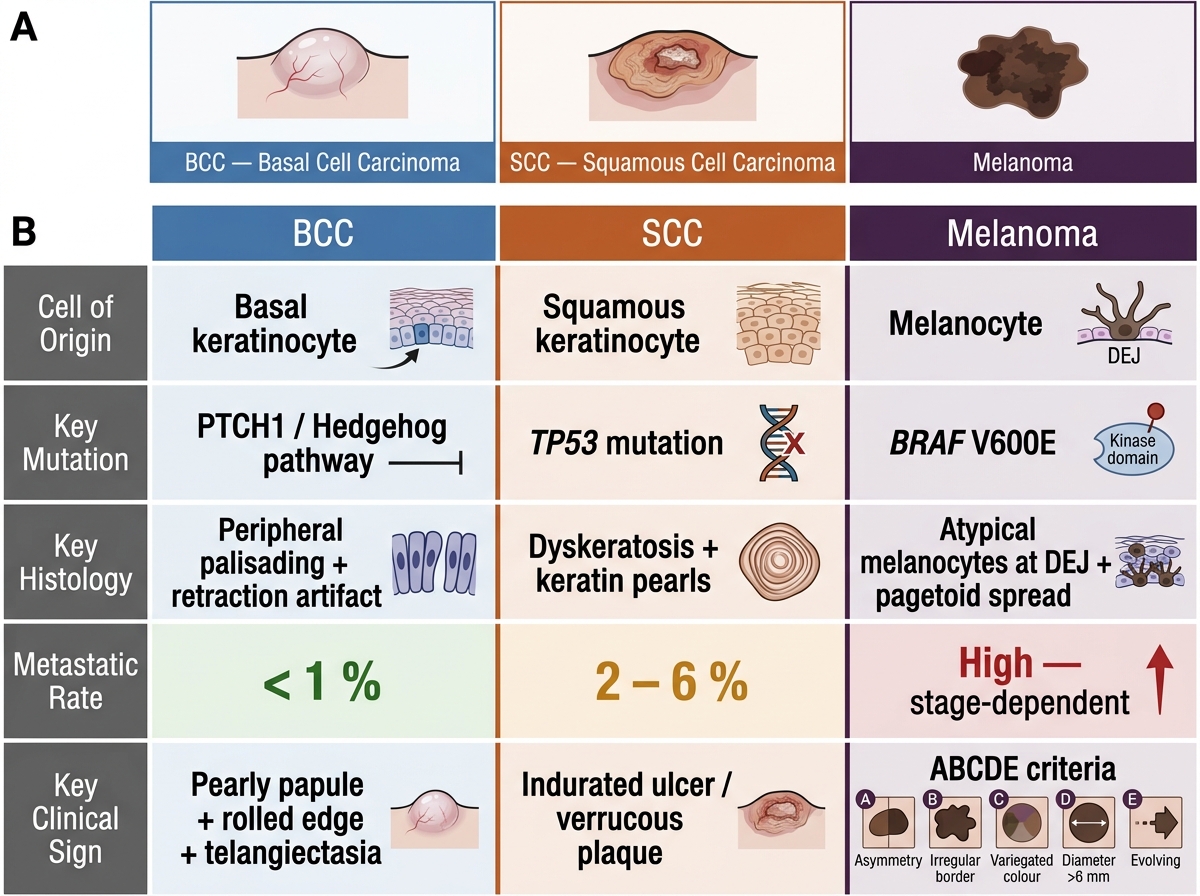
Skin Cancers at a Glance: BCC vs SCC vs Melanoma