Page 4 of 16
PA33.1-3 | Skin Cancers: BCC, SCC & Melanoma — SDL Guide (Part 4)
Melanoma — Metastasis and Clinical Behaviour
Melanoma is distinguished from BCC and SCC by its aggressive metastatic behaviour.
Routes of metastasis:
- Lymphatic — first and most common route: regional lymph nodes → sentinel node biopsy is the standard staging procedure for melanomas >0.8 mm Breslow depth
- Haematogenous — to any organ; classic sites: lung, liver, brain, bone, skin/subcutaneous tissue
- In-transit metastasis — deposits of melanoma cells in the lymphatics between the primary tumour and the regional nodes; appear as pigmented subcutaneous nodules
Staging:
Melanoma staging uses the AJCC TNM system:
• Stage I–II: local disease (Breslow depth + ulceration)
• Stage III: regional lymph node involvement (detected clinically or by sentinel node)
• Stage IV: distant metastases (any organ)
5-year survival:
• Stage I: ~95%
• Stage II: 50–90% (depending on Breslow)
• Stage III: 40–70%
• Stage IV (metastatic): historically <15%; now 30–40% with combination immunotherapy (anti-PD-1 + anti-CTLA-4)
Treatment advances:
• BRAF + MEK inhibition (vemurafenib + cobimetinib; dabrafenib + trametinib) — for BRAF V600E-mutant metastatic melanoma; high initial response rates but resistance develops
• Immune checkpoint inhibitors — pembrolizumab (anti-PD-1), nivolumab (anti-PD-1), ipilimumab (anti-CTLA-4); durable responses in some patients
• The combination of BRAF/MEK inhibitors and immunotherapy is transforming outcomes
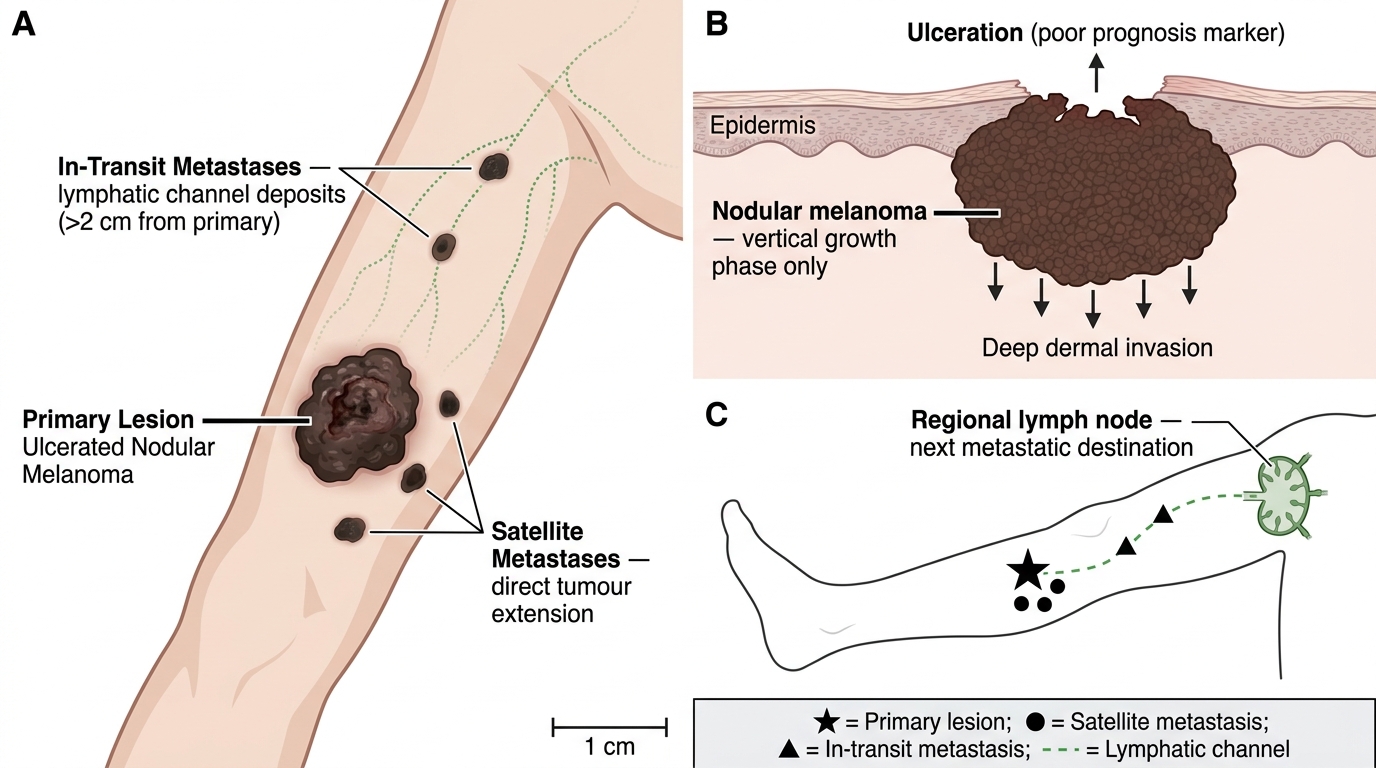
Advanced Nodular Melanoma — Primary Lesion, Satellite Metastases, and In-Transit Metastases
Special scenario — ocular melanoma:
Melanoma can arise from melanocytes in the uveal tract (choroid, ciliary body, iris) — uveal melanoma is the most common primary intraocular tumour in adults. It metastasises primarily to the liver (not lungs). GNAQ/GNA11 mutations (not BRAF). Important to distinguish from cutaneous melanoma because treatment and systemic behaviour differ.
SELF-CHECK
A 52-year-old woman presents with a 3 mm pigmented streak under her right thumbnail that has been there for several months. She reports that the pigment appears to extend slightly onto the skin at the base of the nail. This sign (pigment on the nail fold) is called:
A. Leser–Trélat sign — eruptive seborrhoeic keratoses associated with internal malignancy
B. Hutchinson's sign — pigment from subungual melanoma extending onto the proximal nail fold, indicating aggressive disease
C. Darier's sign — dermographism indicating mastocytosis
D. Nikolsky's sign — epidermal shearing indicating pemphigus
Reveal Answer
Answer: B. Hutchinson's sign — pigment from subungual melanoma extending onto the proximal nail fold, indicating aggressive disease
Hutchinson's sign refers to pigment extending from a subungual (under-nail) melanoma onto the proximal or lateral nail fold. It is a reliable clinical indicator of subungual melanoma — a form of acral lentiginous melanoma that is disproportionately common in dark-skinned populations including South Asians. It must be distinguished from benign racial melanonychia (diffuse nail pigmentation that is common in dark-skinned individuals and lacks extension onto the nail fold). Any subungual pigmented band in a single digit of an adult, especially with Hutchinson's sign, requires biopsy. Note: a 'pseudo-Hutchinson's sign' can occur in benign conditions — clinical context is essential.
SELF-CHECK
A biopsy of a skin lesion shows nests of atypical melanocytes at the dermo-epidermal junction (DEJ) as well as single atypical melanocytes scattered throughout all levels of the epidermis, including the granular layer. There is also a small cluster of melanocytes in the papillary dermis. Breslow depth is 0.9 mm. Which SINGLE feature most strongly predicts metastatic potential in this lesion?
A. Atypical melanocytes scattered throughout the epidermis (pagetoid spread) — confirms malignancy
B. Breslow depth of 0.9 mm — measurement from granular layer to deepest tumour cell, indicating T2 disease and metastatic potential
C. Presence of junctional nests — confirms in-situ component with no metastatic risk
D. Melanocytes in the papillary dermis — confirms benign intradermal naevus pattern
Reveal Answer
Answer: B. Breslow depth of 0.9 mm — measurement from granular layer to deepest tumour cell, indicating T2 disease and metastatic potential
Breslow depth is the single most important prognostic factor in primary melanoma. At 0.9 mm, this tumour is T1b (>0.8 mm or with ulceration/mitoses — AJCC 8th ed.) and qualifies for sentinel lymph node biopsy. The pagetoid spread confirms the diagnosis of melanoma (superficial spreading subtype) but does not itself predict metastasis — it is a diagnostic feature, not a prognostic one. The VGP component (dermal invasion) is what confers metastatic potential, and Breslow depth quantifies exactly how far the VGP has progressed. Melanocytes in the papillary dermis in the context of this lesion represent the vertical growth phase, not a benign intradermal naevus pattern.
CLINICAL PEARL
'Never biopsy a suspected melanoma with a shave or punch that misses the base.' The two most consequential pathologist errors in melanoma diagnosis are: (1) transecting the base — the Breslow depth becomes 'at least X mm' rather than an exact measurement, preventing accurate T staging and SLNB recommendation; (2) sampling the non-representative part — a thick nodular melanoma biopsied at its thin edge will be under-staged. The correct technique is excisional biopsy with 1–2 mm narrow margins, oriented with the long axis along the lymphatic drainage direction (allows wider re-excision if needed). For very large lesions where excision is not feasible, a punch biopsy through the thickest or most atypical area is acceptable. Dermoscopy-guided biopsy targeting the most atypical region improves accuracy.