Page 3 of 16
PA33.1-3 | Skin Cancers: BCC, SCC & Melanoma — SDL Guide (Part 3)
Naevus vs Melanoma — The ABCDE Criteria (PA33.3)
The ABCDE criteria are the clinical tool for distinguishing a benign naevus from a melanoma or high-risk lesion requiring biopsy. This is a direct NMC 2024 competency (PA33.3).
| Letter | Criterion | Benign Naevus | Melanoma (Red Flag) |
|---|---|---|---|
| A | Asymmetry | Symmetric — one half mirrors the other | Asymmetric — halves do not match |
| B | Border | Regular, smooth, well-defined | Irregular, notched, scalloped, ill-defined |
| C | Colour | Uniform tan or brown | Multiple colours — tan, brown, black, red, white, blue |
| D | Diameter | Usually <6 mm | Usually >6 mm (size of a pencil eraser) |
| E | Evolution | Stable over years | Changing in size, shape, colour, or new symptom (bleeding, itching) |
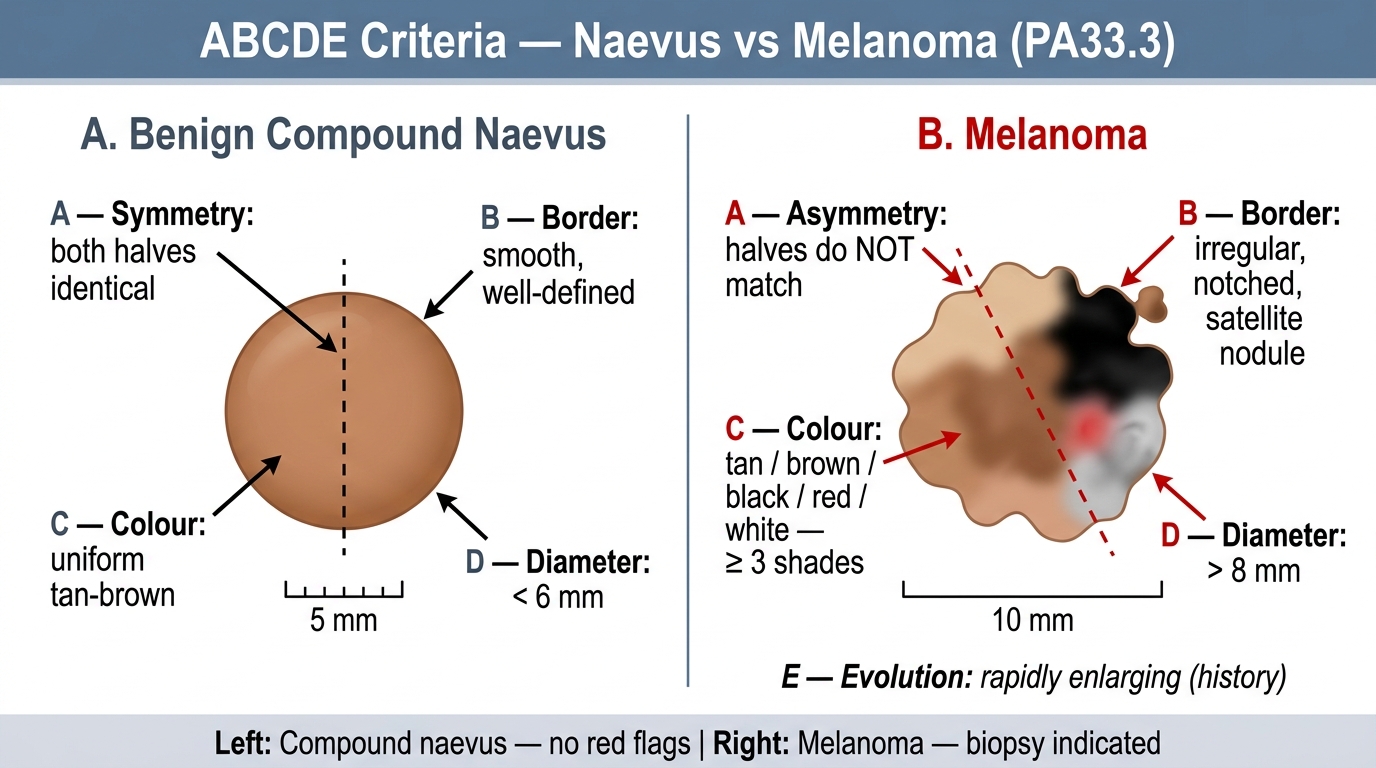
ABCDE Criteria — Benign Compound Naevus vs Melanoma
Additional clinical flags:
• 'Ugly duckling' sign — a lesion that looks different from all the patient's other moles should be biopsied
• Dermoscopy extends clinical assessment: the 7-point checklist or pattern analysis can detect features invisible to the naked eye
The 'E' (Evolution) criterion is arguably the most important — a lesion that is CHANGING must be biopsied, regardless of the other criteria. This is the cardinal principle.
Practical rule for Indian clinical practice: Acral lentiginous melanoma (see below) occurs on the palms, soles, and subungual areas — sites where doctors may not think to look. A pigmented streak under a nail (subungual melanoma) causing Hutchinson's sign (pigment extending onto the nail fold) is an emergency.
Melanoma — Aetiology, Pathogenesis, and Molecular Biology (PA33.3)
Melanoma is a malignant tumour of melanocytes — the pigment-producing cells of the basal layer of the epidermis. Despite accounting for only ~5% of skin cancers, melanoma causes >75% of skin cancer deaths due to its high metastatic potential.
Aetiology and risk factors:
| Risk Factor | Detail |
|---|---|
| UV radiation (UVA + UVB) | Especially intermittent intense exposure with sunburn in childhood/adolescence — different pattern from SCC/BCC (which require cumulative chronic exposure) |
| Dysplastic naevus syndrome | >50 atypical naevi; family history → extremely high lifetime risk |
| Family history / genetics | CDKN2A germline mutations (familial melanoma); rare |
| Fair skin (Fitzpatrick I–II) | Less melanin → less UV protection |
| Giant congenital naevus | >20 cm naevus → ~5% lifetime risk |
| Immunosuppression | HIV, transplant patients |
| Xeroderma pigmentosum | DNA repair defect → UV damage unchecked |
Molecular pathogenesis — the MAPK pathway:
The central signalling cascade in melanoma is the RAS–RAF–MEK–ERK (MAPK) pathway, which drives cell proliferation.
- BRAF V600E mutation — present in ~50% of cutaneous melanomas; a single valine-to-glutamate substitution at codon 600 of the BRAF kinase domain creates constitutive, ligand-independent BRAF kinase activity → perpetual ERK signalling → cell proliferation and survival
- NRAS mutation — present in ~20% of melanomas; activates both MAPK and PI3K–AKT pathways
- NF1 loss — ~15%; NF1 is a RAS-GAP (inactivates RAS) — loss = constitutive RAS activation
- CDKN2A (p16) loss — prevents Rb inactivation; accelerates cell cycle entry
- c-KIT mutation — acral lentiginous and mucosal melanomas; targeted by imatinib
Clinical importance: BRAF V600E is the target of vemurafenib and dabrafenib (BRAF inhibitors) + trametinib (MEK inhibitor) — combination targeted therapy that has transformed metastatic melanoma treatment. BRAF mutation testing is now mandatory before systemic therapy.
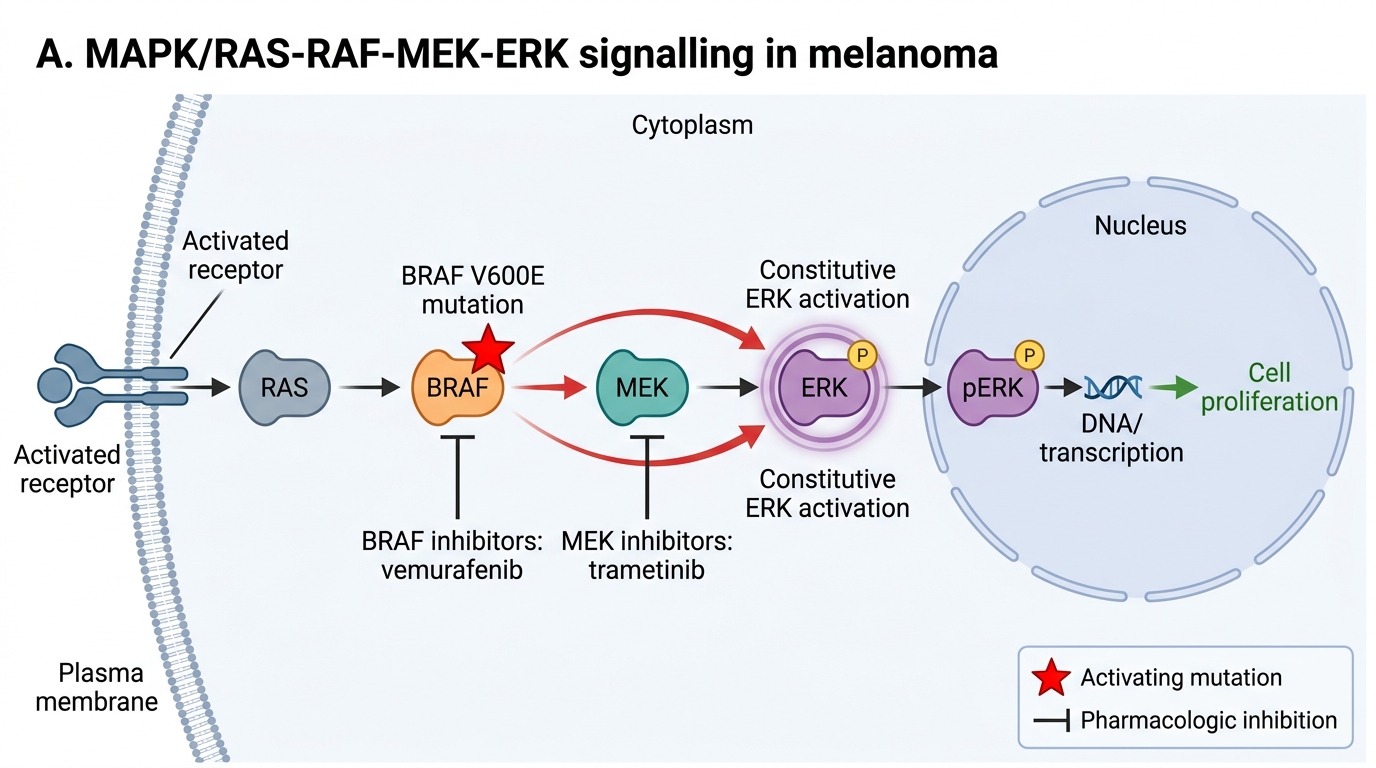
MAPK Pathway Activation in BRAF V600E Melanoma
Melanoma — Growth Phases, Subtypes, and Prognostic Staging (PA33.3)
Growth phases of melanoma — understanding these is fundamental to prognosis:
Radial growth phase (RGP):
• Melanoma cells spread horizontally within the epidermis and superficial dermis
• Cells grow parallel to the skin surface
• Excellent prognosis — tumour cells in RGP do not have the capacity to metastasise
• Corresponds to early, superficial tumour
Vertical growth phase (VGP):
• Tumour cells begin to invade downward into the dermis
• Cells acquire metastatic potential (develop survival signals independent of the primary tumour microenvironment)
• Poor prognosis — VGP is the critical transition
• Breslow depth and Clark level measure the extent of VGP
Breslow depth (the primary prognostic measurement):
| Breslow Thickness | T stage | 5-yr Survival (approx.) |
|---|---|---|
| ≤1.0 mm | T1 | ~95% |
| 1.01–2.0 mm | T2 | ~80% |
| 2.01–4.0 mm | T3 | ~70% |
| >4.0 mm | T4 | ~50% |
Breslow depth is measured from the granular layer of the epidermis to the deepest tumour cell in the dermis. It is measured by the pathologist using an ocular micrometer on H&E sections — this is why a melanoma diagnosis is incomplete without an adequately oriented biopsy.
Clark level (anatomical level of invasion — now less used, Breslow preferred):
• Level I: confined to epidermis (in situ)
• Level II: papillary dermis
• Level III: filling papillary dermis
• Level IV: reticular dermis
• Level V: subcutaneous fat
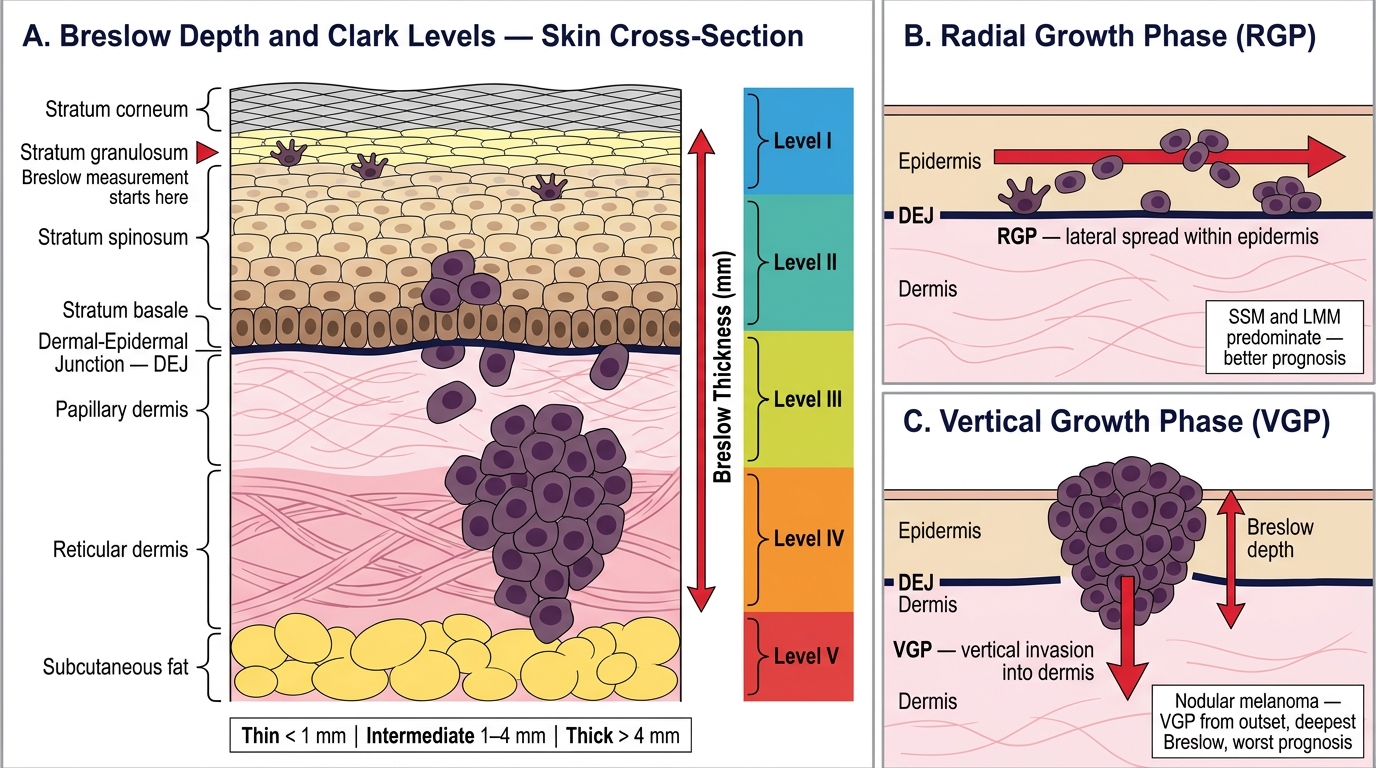
Melanoma Depth Measurement: Breslow Thickness, Clark Levels I–V, and Growth Phases (RGP vs VGP)
Histological subtypes of melanoma:
(1) Superficial spreading melanoma (SSM) — most common (~70%):
• Arises on any skin site; back in men, legs in women
• Pagetoid spread — malignant melanocytes spread upward through the epidermis as single cells (Paget cells — large atypical cells in an epithelium)
• Nests of atypical melanocytes at all levels of the epidermis
• RGP predominates early; later VGP
(2) Nodular melanoma (~15%):
• VGP from the outset — no radial growth phase; invades deeply immediately
• Presents as rapidly growing dark nodule, often ulcerated
• Worst prognosis per unit time — high Breslow depths at diagnosis
(3) Lentigo maligna melanoma (~10%):
• Arises in lentigo maligna (Hutchinson's freckle) — a flat, slowly growing in situ lesion on chronically sun-damaged skin of elderly patients
• Site: face, especially cheeks, nose
• Long RGP (years to decades) before VGP; relatively better prognosis
• Histology: atypical single melanocytes along the DEJ, solar elastosis in dermis
(4) Acral lentiginous melanoma (~5–10% in Caucasians; up to 70% in Asians and Africans):
• Sites: palms, soles, subungual (under nails) — NOT sun-exposed skin
• Most common melanoma subtype in dark-skinned populations including Indians
• Often diagnosed late → higher Breslow depths
• Subungual melanoma: pigmented band in nail with Hutchinson's sign (pigment onto nail fold)
• c-KIT mutations common (not BRAF)
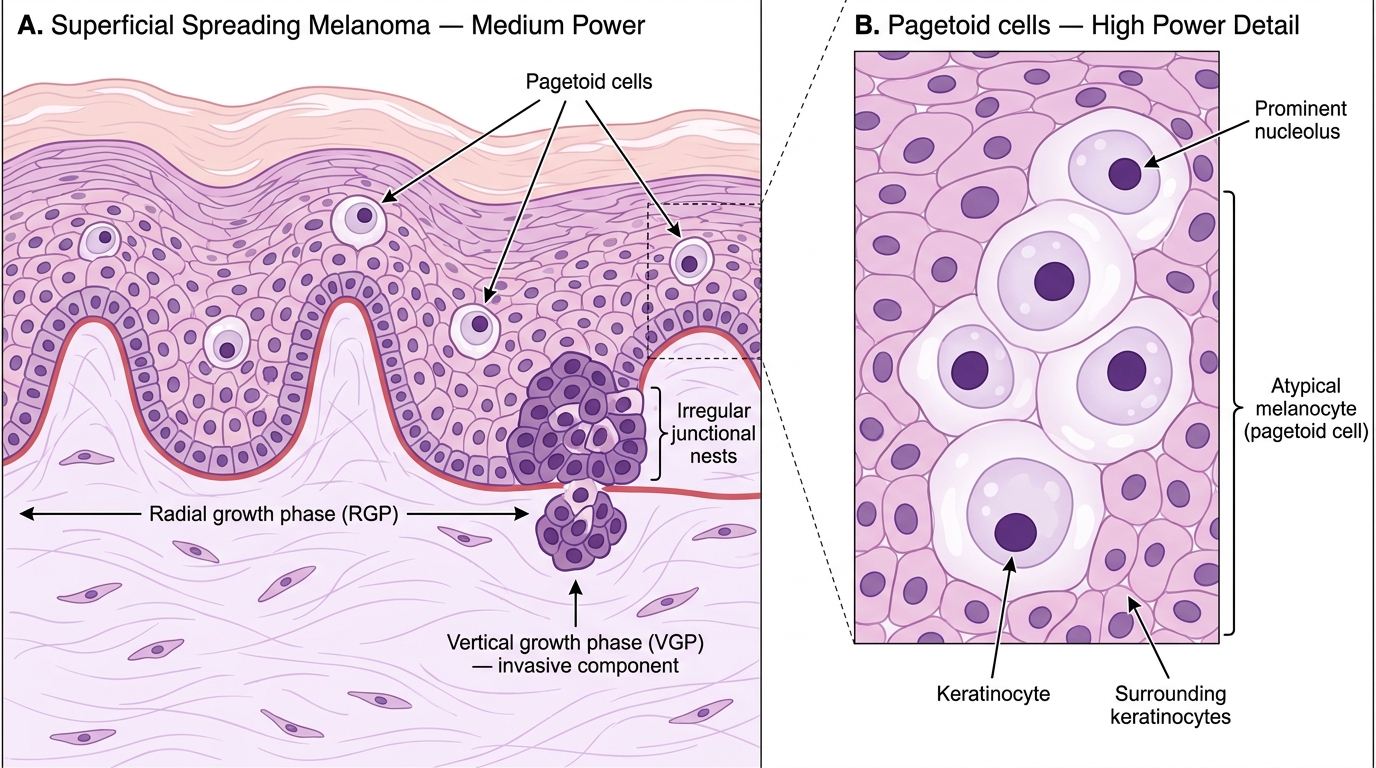
Histology of Superficial Spreading Melanoma: Pagetoid Spread, Growth Phases, and Junctional Nests
Immunohistochemistry (IHC) of melanoma:
| Marker | Sensitivity | Notes |
|---|---|---|
| S100 | ~97% | Most sensitive; also marks nerves, Langerhans cells — not specific; loss in dedifferentiated melanoma |
| HMB-45 (anti-gp100) | ~80% | More specific than S100; positive in naevi too but stronger in melanoma |
| Melan-A (MART-1) | ~85% | Specific; not expressed in spindle cell melanoma |
| SOX10 | ~98% | Nuclear; excellent sensitivity including spindle cell variants |
For diagnosing metastatic deposits: a panel of S100 + HMB-45 + Melan-A (positive) with cytokeratin (negative, to exclude carcinoma) is standard.
CLINICAL PEARL
Breslow depth is the single most important prognostic factor in primary melanoma — more important than Clark level, subtype, or even lymph node status for thin melanomas. The pathologist's measurement of Breslow depth determines the required surgical excision margin and the recommendation for sentinel lymph node biopsy (SLNB). Tumours >0.8 mm (or >0.75 mm with ulceration) qualify for SLNB. This is why a superficial shave biopsy that does not include the base of a melanoma is inadequate — it renders Breslow depth unmeasurable and prevents proper staging. Always insist on excisional biopsy or at minimum a punch biopsy through the thickest part when melanoma is suspected.