Page 2 of 16
PA33.1-3 | Skin Cancers: BCC, SCC & Melanoma — SDL Guide (Part 2)
Basal Cell Carcinoma (BCC) — Pathogenesis and Pathology (PA33.2)
Basal cell carcinoma (BCC) is the most common malignant tumour in humans — accounting for approximately 75–80% of all skin cancers. It arises from the pluripotent basal keratinocytes (or the outer root sheath of hair follicles).
Risk factors:
| Risk Factor | Notes |
|---|---|
| UV/sun exposure | Most important — especially intermittent intense exposure |
| Fitzpatrick type I–II | Fair skin, blue eyes, burns easily |
| Gorlin syndrome (naevoid BCC syndrome) | Autosomal dominant; PTCH1 germline mutation; hundreds of BCCs from childhood |
| Immunosuppression | 10× increased risk |
| Arsenic exposure | Produces multiple superficial BCCs |
| Prior radiation therapy | BCCs arise in the radiation field after a latency of years |
Pathogenesis — the Hedgehog pathway:
This is one of the most clearly understood carcinogenic pathways in oncology.
The normal Hedgehog (Hh) signalling pathway:
1. PTCH1 (Patched 1) — a membrane receptor that normally inhibits Smoothened (SMO)
2. When the Hedgehog ligand binds PTCH1, the inhibition of SMO is relieved
3. SMO activates transcription factors GLI1/GLI2 → gene expression promoting cell proliferation
In BCC:
• UV-induced inactivating mutation in PTCH1 (the tumour suppressor) → PTCH1 cannot suppress SMO → constitutive, ligand-independent activation of Hh signalling → uncontrolled GLI-driven proliferation
• Less commonly: activating mutation in SMO itself
• Clinical importance: Vismodegib and sonidegib are small-molecule SMO inhibitors — FDA-approved targeted therapy for locally advanced or metastatic BCC (rare but exists)
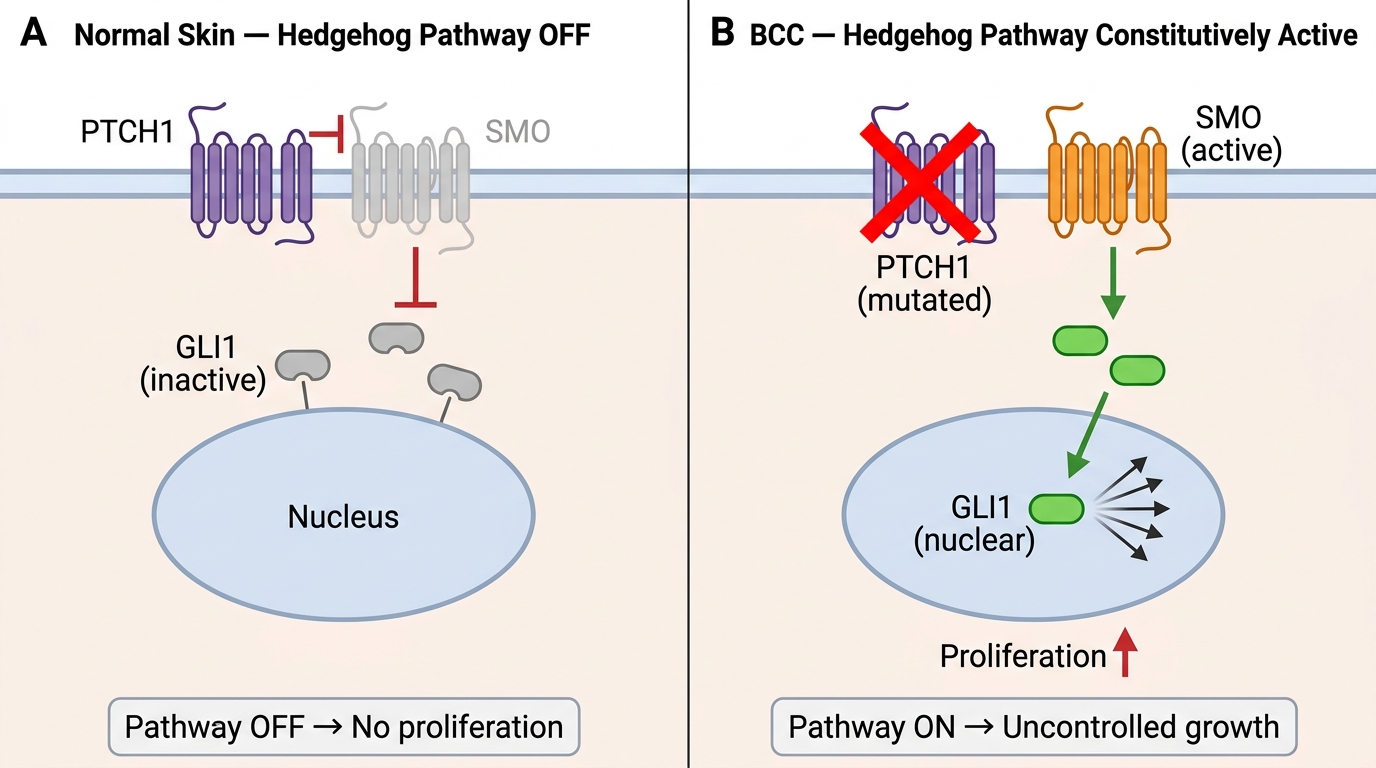
Hedgehog Signalling Pathway: Normal Skin vs Basal Cell Carcinoma
Histological patterns of BCC:
(1) Nodular BCC — the most common subtype (~60–70%):
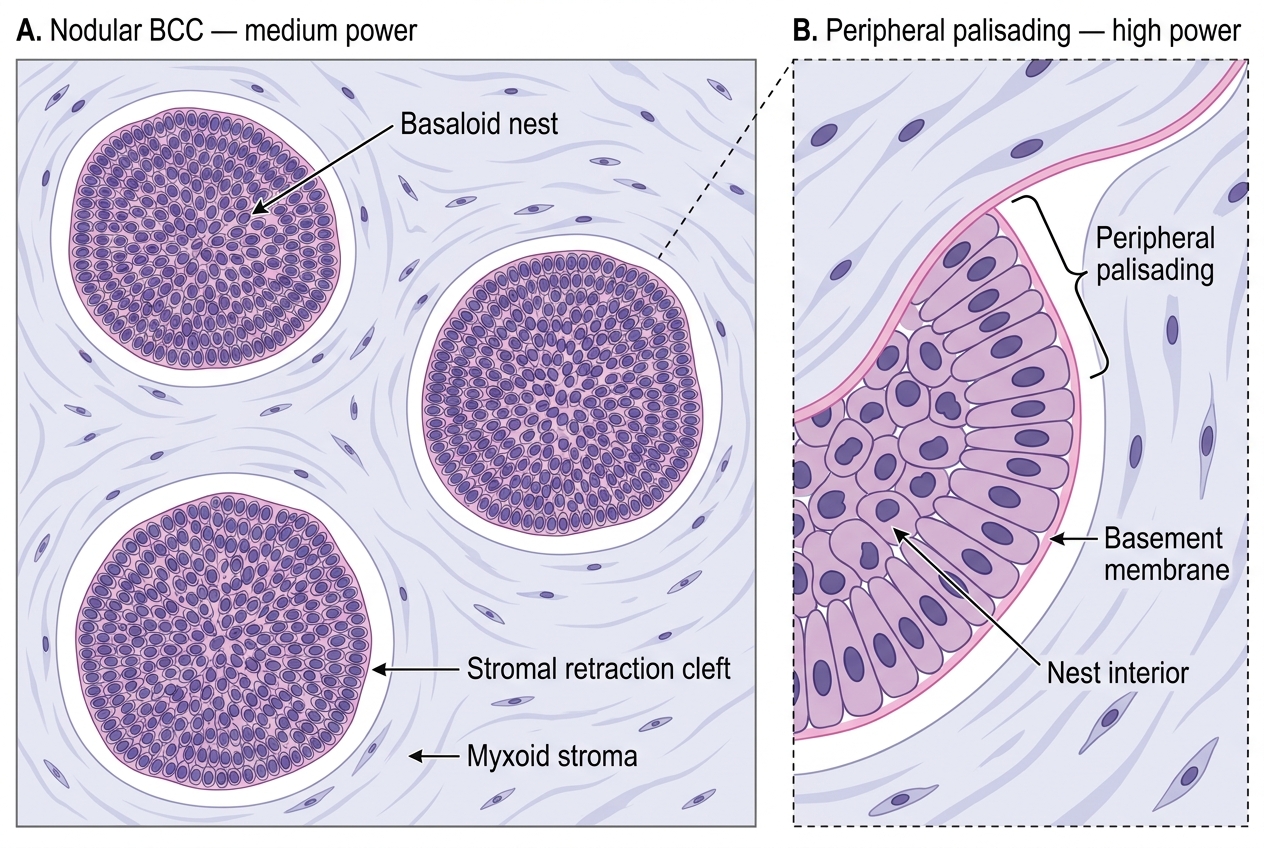
Nodular Basal Cell Carcinoma — Histological Features
- Basaloid cells — small, uniform cells with scant cytoplasm and oval, hyperchromatic nuclei; resemble the basal layer cells (hence the name)
- Peripheral palisading — at the edge of every tumour nest, cells line up perpendicular to the basement membrane, like a picket fence; highly characteristic of BCC
- Stromal retraction (clefting) — a clear space appears between the tumour nests and the stroma; this is a fixation artifact (the mucin-rich stroma shrinks away from the nests during processing) but it is a diagnostically important artifact
- Minimal mitoses; minimal nuclear pleomorphism — BCC is a 'slow grower' cytologically
- Mucin (myxoid stroma) — blue-grey mucinous material in the stroma
(2) Morphoeic (sclerosing/infiltrative) BCC — the most dangerous subtype:
• Thin cords and strands of basaloid cells embedded in a dense desmoplastic fibrous stroma
• No peripheral palisading; no retraction clefts
• Poorly defined clinical margins → highest recurrence rate after excision
• Clinical appearance: flat, scar-like, indurated plaque (easily missed)
(3) Superficial BCC:
• Buds of basaloid cells attached to the undersurface of the epidermis, extending only superficially
• Seen on the trunk; multiple lesions common in arsenic exposure
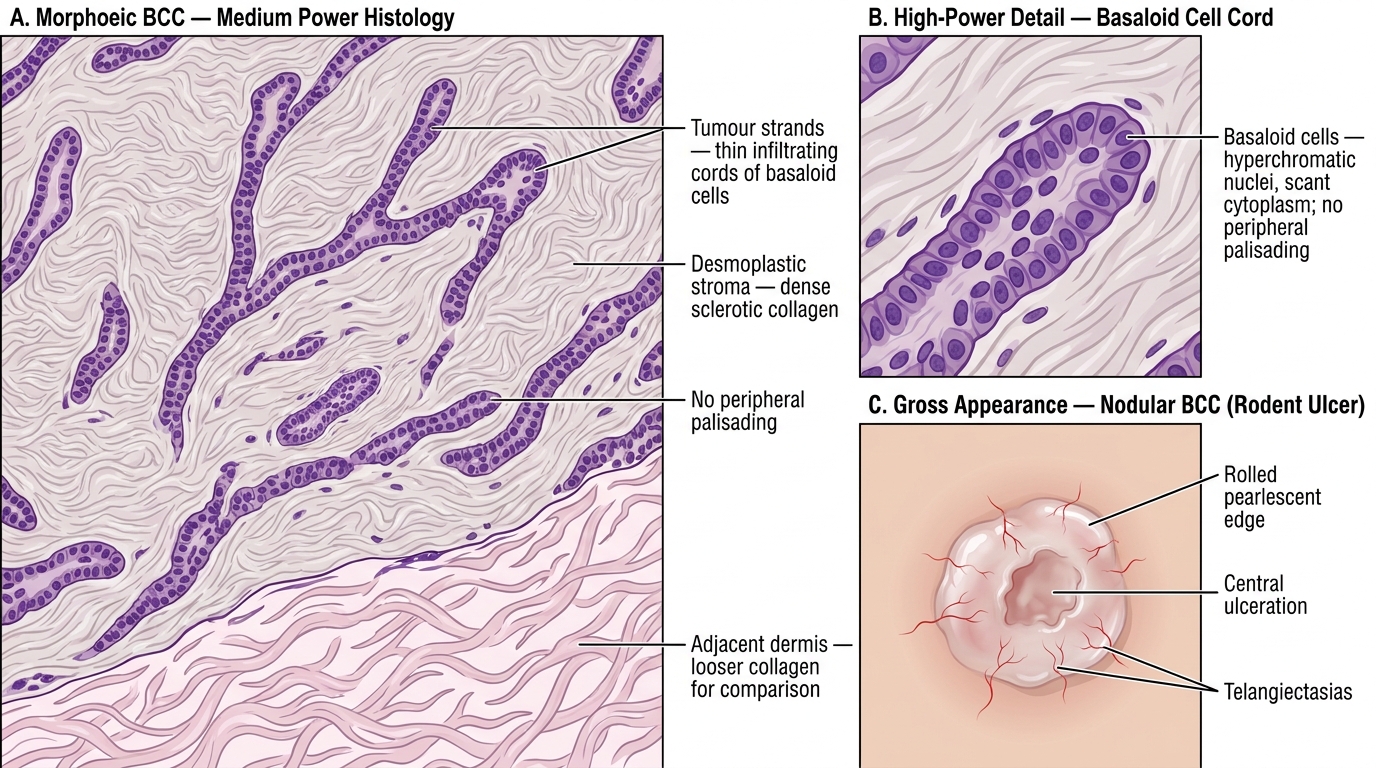
Morphoeic BCC — Histology and Gross Appearance
Gross appearance:
- Nodular BCC ("rodent ulcer"): Pearly, translucent nodule with rolled (pearlescent) edges and central ulceration; overlying telangiectasias (superficial blood vessels) visible through the thinned epidermis; classically on the face, nose, or periorbital area
- The term 'rodent ulcer' historically described the central ulceration that can progressively enlarge and erode underlying tissue (like a rodent gnawing)
Natural history — locally destructive, almost never metastasises:
This is the most clinically important fact about BCC:
- Metastatic rate: <0.01–0.1% — extraordinarily rare; BCC is therefore classified as a locally invasive malignancy, not a metastatic one
- Local destruction is the key threat: untreated BCC can erode deeply into subcutaneous tissue, cartilage (nose, ear), and bone (skull, orbit) — hence the 'rodent ulcer' metaphor
- Recurrence after incomplete excision is common, especially morphoeic subtype
- Why doesn't BCC metastasise? Several theories: (1) tumour cells require specific stromal signals (paracrine dependence) that are not available at distant sites; (2) lack of efficient lymphovascular invasion machinery; (3) slow growth rate
Management: Surgical excision with clear margins is the standard. Mohs micrographic surgery for high-risk/morphoeic lesions. Vismodegib for locally advanced/unresectable disease.
BCC vs SCC vs Melanoma — Comparison Table
| Feature | BCC | SCC | Melanoma |
|---|---|---|---|
| Cell of origin | Basal keratinocyte / hair follicle outer root sheath | Suprabasal keratinocyte | Melanocyte |
| Frequency | Most common skin cancer (~75%) | Second most common (~20%) | ~5% but most deadly |
| Key mutation | PTCH1 (Hedgehog pathway) | TP53 (UV-induced) | BRAF V600E (~50%), NRAS |
| Main UV type | UVB (intense/intermittent) | UVB (cumulative, chronic) | UVA + UVB |
| Gross appearance | Pearly nodule, rolled edges, telangiectasias | Indurated ulcerated plaque/nodule | Pigmented, irregular, asymmetric |
| Key histology | Basaloid nests, peripheral palisading, retraction cleft | Keratin pearls, atypical squamous cells | Atypical melanocytes, pagetoid spread, radial/vertical growth phases |
| Premalignant lesion | None clearly defined (AK is SCC precursor, not BCC) | Actinic keratosis, Bowen's disease | Dysplastic naevus |
| Metastatic potential | Almost none (<0.1%) | Low (2–5%), higher in high-risk SCC | High; can metastasise early |
| Prognosis | Excellent (local control) | Good (localised); poor (metastatic) | Poor once metastatic |
| Key prognostic measure | Completeness of excision | Depth, grade, LVI, perineural invasion | Breslow depth, Clark level, ulceration, mitoses |
| IHC markers | BerEP4+, EMA−, S100− | CK5/6+, p40+, EMA+, S100− | S100+, HMB-45+, Melan-A+ |
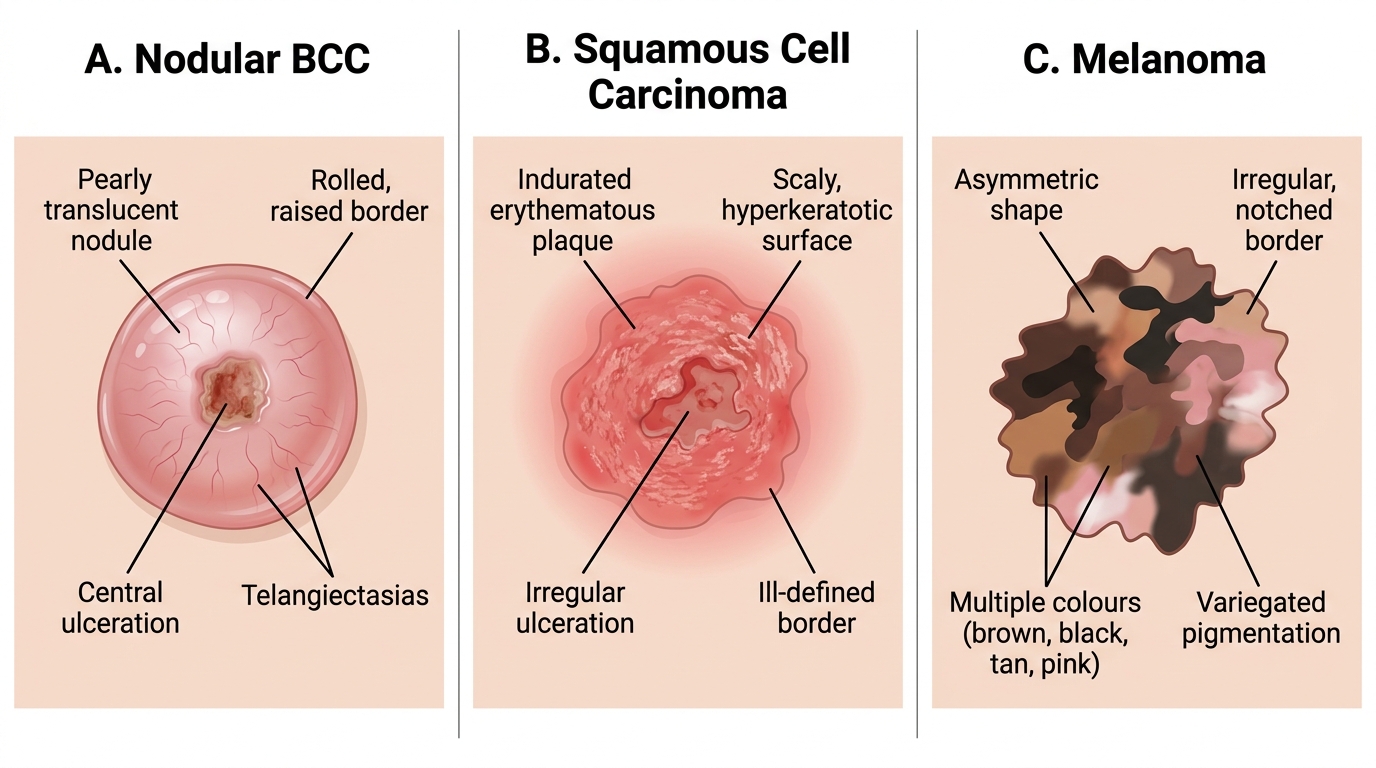
Clinical Comparison of Common Skin Malignancies: BCC, SCC, and Melanoma
SELF-CHECK
A histology slide from a skin biopsy shows nests of small, uniform basaloid cells with scant cytoplasm. At the periphery of each nest, the cells are arranged perpendicular to the basement membrane. There is a clear space between the tumour nests and the surrounding stroma. Which of the following BEST describes these findings?
A. Keratin pearls — confirming well-differentiated squamous cell carcinoma
B. Peripheral palisading with retraction clefting — confirming nodular basal cell carcinoma
C. Pagetoid spread — confirming melanoma in situ
D. Full-thickness epidermal atypia — confirming Bowen's disease (SCC in situ)
Reveal Answer
Answer: B. Peripheral palisading with retraction clefting — confirming nodular basal cell carcinoma
The description precisely matches nodular BCC: (1) small basaloid cells with scant cytoplasm — unlike the large pink squamous cells of SCC; (2) peripheral palisading (cells arranged perpendicular at the nest edge — like a picket fence) — pathognomonic of BCC; (3) retraction cleft (clear space between nest and stroma) — a fixation artifact characteristic of BCC. Keratin pearls are concentric whorls of eosinophilic keratin seen in SCC. Pagetoid spread (single atypical cells spreading along the basal layer) characterises melanoma in situ. Full-thickness epidermal atypia is Bowen's disease.
Melanocytic Naevus — The Benign Baseline
Before understanding melanoma, you must understand what it is NOT — the benign melanocytic naevus (common mole).
Melanocytic naevus (plural: naevi) is a benign proliferation of naevus cells (melanocytes that have aggregated into clusters called nests).
Types of common acquired naevi:
- Junctional naevus — nests of naevus cells at the dermo-epidermal junction (DEJ); flat, uniformly pigmented macule; seen in children and adolescents
- Compound naevus — nests at the DEJ and in the dermis; slightly raised, pigmented papule
- Intradermal naevus — nests entirely within the dermis; flesh-coloured or lightly pigmented dome-shaped papule; seen in adults
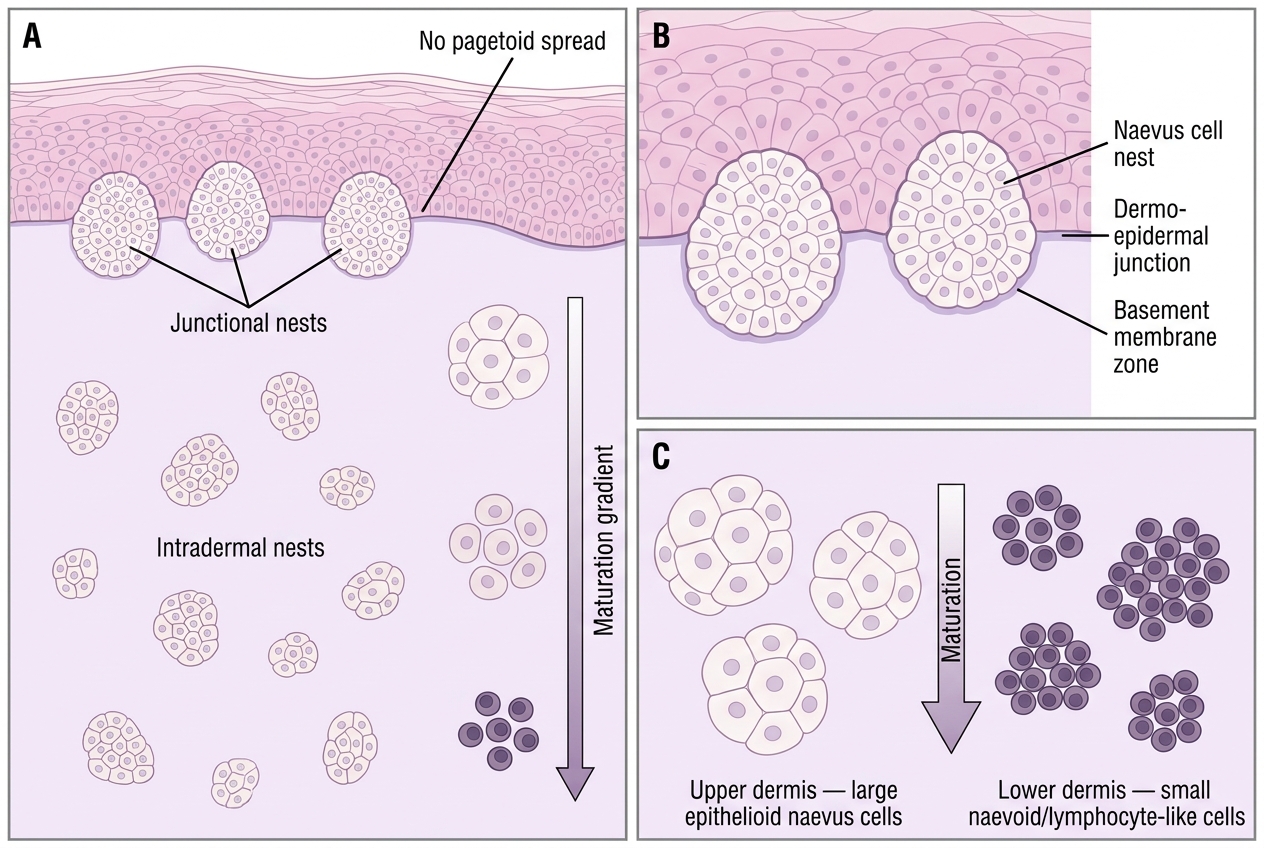
This sequence (junctional → compound → intradermal) represents the natural progression of naevi as the naevus cells 'mature' and migrate downwards — this is called naevus maturation.
Histological features of benign naevi (features that say 'don't worry'):
• Maturation — naevus cells in the superficial dermis are larger; those deeper are smaller (opposite of what malignant cells do)
• Orderly nests — regular, similar-sized nests with equal spacing
• No pagetoid spread — naevus cells do not migrate upward through the epidermis (epidermal levels above the DEJ are free of naevus cells)
• No significant mitoses in the dermis
• No ulceration
Compound Melanocytic Naevus — Histological Features
Dysplastic naevus (Clark's naevus):
A dysplastic naevus is an architecturally and cytologically atypical naevus that is considered a precursor lesion and marker for increased melanoma risk. Features: size >5 mm, irregular border, variable pigmentation ('fried egg' appearance clinically). Histology: bridging of rete ridges, shouldering, lamellar fibroplasia, mild–moderate cytological atypia. Patients with dysplastic naevus syndrome (>50 atypical moles, family history of melanoma) have a lifetime melanoma risk approaching 100%.