Page 1 of 13
PS1.1 | Psychiatric Classification Foundations — SDL Guide
Learning Objectives
- Describe the historical and conceptual basis of psychiatric classification systems
- Distinguish neurotic from psychotic disorders using the ICD-11 and DSM-5 frameworks
- Differentiate organic from non-organic (functional) psychiatric disorders with clinical examples
- Apply classification principles to categorise common psychiatric presentations encountered in medical practice
INSTRUCTIONS
Classification is the backbone of clinical psychiatry — without a shared language for grouping disorders, diagnosis, communication between clinicians, and rational treatment selection would collapse. This module equips you with the conceptual map that underlies every psychiatric diagnosis you will encounter as a physician, whether in a general ward, emergency setting, or outpatient clinic.
References
- Ahuja N. A Short Textbook of Psychiatry, 8th ed., Ch. 1 & 2 (textbook)
- Kaplan & Sadock's Synopsis of Psychiatry, 12th ed., Ch. 1 (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 35-year-old woman presents to the medicine outpatient department saying she 'hears voices telling her she is being watched.' Her husband reports she has been increasingly withdrawn for the past two months, neglecting household responsibilities, and expressing unusual beliefs that her food is being poisoned. Meanwhile, a 55-year-old man in the adjacent bed is diagnosed with delirium following post-operative recovery from a hepatic resection — he too is confused and agitated, and seeing things that are not there. Both patients are experiencing psychotic features, yet their diagnoses, causes, and treatments are entirely different. How does psychiatry create order from such apparent clinical overlap? The answer begins with classification.
WHY THIS MATTERS
As a medical graduate, you will encounter patients with psychiatric symptoms in every clinical setting — from emergency departments managing acute psychosis, to general medicine wards where delirium mimics dementia, to primary care where anxiety disorders present with somatic complaints. The ability to place a patient's symptoms within a classification framework is not an abstract academic exercise: it determines which investigations to order (ruling out organic causes first), which specialist to refer to, and which broad treatment category to initiate. The NMC 2024 curriculum (PS1.1) mandates this foundational competency precisely because a misclassified disorder leads to mismanaged care.
RECALL
Before proceeding, recall from your Physiology and Biochemistry studies: the brain's neurotransmitter systems — dopaminergic, serotonergic, noradrenergic, and GABAergic pathways — are the molecular substrates that underpin both normal mental function and its disorders. From Pathology, you learned how systemic disease (thyroid dysfunction, hepatic failure, vitamin deficiencies) can produce neuropsychiatric manifestations. These cross-disciplinary links are central to understanding the organic versus non-organic distinction in psychiatry.
Why Psychiatric Classification Matters: Historical and Clinical Context
Psychiatric classification has evolved over more than a century, driven by the recognition that clinical psychiatry needed a common diagnostic language to enable systematic research, reliable communication between practitioners, and rational treatment planning. Before the development of standardised systems, diagnosis was highly subjective and varied enormously between clinicians, institutions, and countries — a patient diagnosed with schizophrenia in one country might be labelled as having a personality disorder in another. This lack of reliability was not merely an academic inconvenience; it meant that clinical trials, epidemiological studies, and treatment guidelines could not be meaningfully compared or generalised.
The two major classification systems currently in use are the World Health Organization's International Classification of Diseases, 11th revision (ICD-11), which came into effect in January 2022 and is the system predominantly used in India and most of the world for official health statistics and clinical practice, and the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5), published in 2013, which is widely used in research, North America, and increasingly in international psychiatric literature. Both systems use a descriptive, operational approach — that is, they define disorders by observable, agreed-upon clusters of symptoms and signs with specified duration and impairment criteria, rather than by presumed aetiology or underlying biological mechanisms, which remain incompletely understood for most psychiatric conditions.
For the Indian medical graduate, the ICD-11 is the primary reference for clinical practice and medicolegal documentation. However, DSM-5 is frequently cited in research literature and postgraduate examinations, and its criteria are often more operationally explicit. Understanding both systems and knowing where they agree and diverge is a core competency for the modern psychiatrist and general physician alike.
A student beginning psychiatry may wonder why psychiatry 'needs' its own classification when medicine classifies diseases by pathology and aetiology. The honest answer is that for most psychiatric disorders, the precise neuropathological substrate remains unknown — we cannot biopsy a depressed brain the way we biopsy a tumour. Classification therefore rests on phenomenology (the pattern and quality of symptoms as experienced and reported by the patient) rather than histopathology.
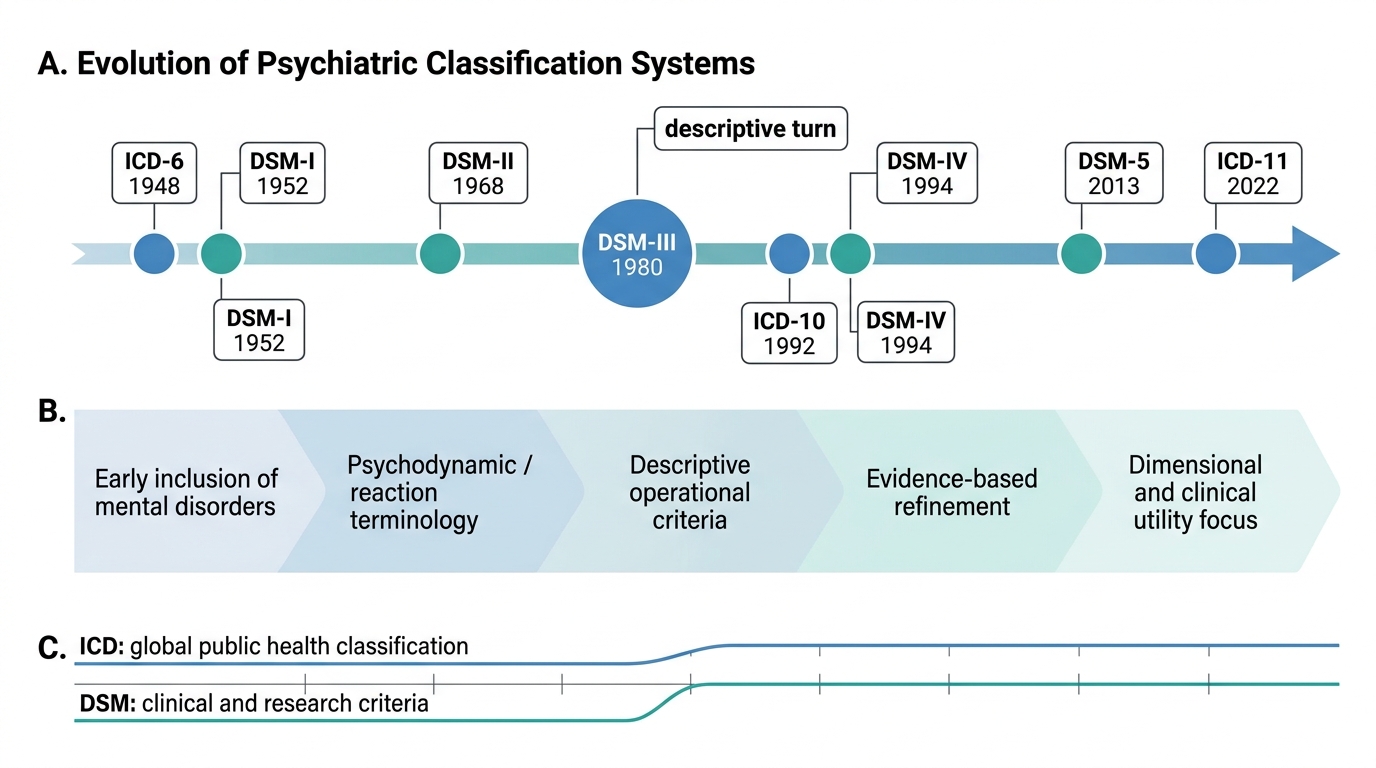
Evolution of Psychiatric Classification Systems
The Neurotic-Psychotic Dichotomy: Conceptual Basis and Current Status
The distinction between neurosis and psychosis is one of the oldest and most clinically useful frameworks in psychiatry, even though the ICD-11 has formally moved away from using 'neurosis' as a primary organising category. Understanding this dichotomy remains essential because it underpins much of the clinical reasoning taught in undergraduate psychiatry and continues to appear in textbooks, clinical discussions, and examination questions.
Provided image
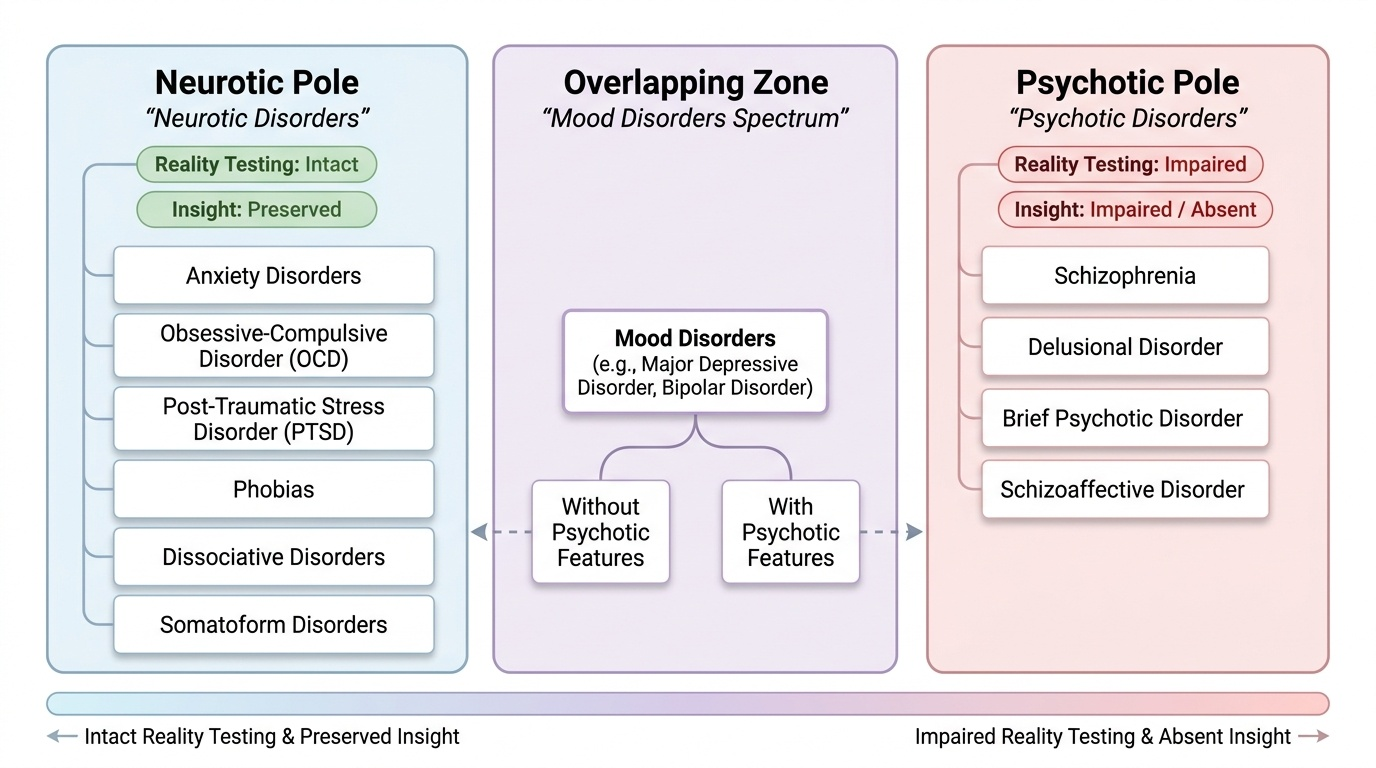
The conceptual basis of the neurotic-psychotic divide rests on two dimensions: reality testing and insight. In neurotic disorders (now largely subsumed under ICD-11's 'Anxiety and fear-related disorders,' 'Obsessive-compulsive or related disorders,' 'Disorders specifically associated with stress,' and 'Dissociative disorders'), the patient retains contact with shared reality — they recognise that the world around them is real, even though they may experience excessive fear, compulsive rituals, conversion symptoms, or depressive cognitions. Crucially, the neurotic patient retains insight — an awareness that their symptoms are abnormal or excessive, even if they cannot control them. A patient with obsessive-compulsive disorder (OCD) who repeatedly washes their hands knows the compulsion is irrational; this preserved insight is a hallmark of the neurotic spectrum.
In psychotic disorders, by contrast, the patient experiences a fundamental break with shared reality. Hallucinations (perceptions without an external stimulus — most commonly auditory in schizophrenia), delusions (fixed false beliefs held with conviction and not amenable to reason, inconsistent with the patient's cultural background), disorganised thinking, and severely disorganised or catatonic behaviour are the cardinal features. Insight is characteristically impaired or absent — the patient does not recognise their experiences as symptoms of illness. The major psychotic disorders under ICD-11 include schizophrenia (required duration of core symptoms ≥1 month per ICD-11; note that DSM-5 requires a total duration of ≥6 months including prodromal and residual phases), schizoaffective disorder, delusional disorder, brief psychotic disorder (<1 month of psychotic symptoms), and psychotic episodes within severe mood disorders (such as psychotic depression or bipolar disorder with psychotic features).
Important caveat: ICD-11 has restructured its chapter on mental disorders and no longer uses 'neurosis' as a chapter heading, reflecting the recognition that the neurotic-psychotic boundary is a spectrum rather than a sharp divide — some conditions (e.g. severe OCD with poor insight, or major depressive disorder with psychotic features) sit at the boundary. Nevertheless, the neurotic-psychotic framework remains a valid and useful teaching framework for organising clinical thinking, and Ahuja's Short Textbook of Psychiatry retains this organisation as pedagogically appropriate for undergraduate education.
IMPORTANT CLASSIFICATION CONSISTENCY: A disorder placed under the psychotic category must not simultaneously be framed as neurotic. Schizophrenia, delusional disorder, and acute/transient psychotic episodes are psychotic disorders — they must not be listed under the neurotic spectrum in any table or discussion. Conversely, anxiety disorders, phobias, OCD, PTSD, adjustment disorders, and dissociative disorders are neurotic-spectrum conditions — they do not involve loss of reality testing as a primary feature.
IMPORTANT IMAGE: Classification tree showing the neurotic-psychotic spectrum with representative disorders under each pole.
Diagnostic duration note: Major depressive episode (MDE) requires ≥2 weeks of symptoms (ICD-11 and DSM-5 largely concordant); manic episode requires ≥1 week (or any duration if hospitalisation is required; ICD-11/DSM-5); hypomanic episode requires ≥4 days (ICD-11/DSM-5); generalised anxiety disorder (GAD) requires ≥6 months of persistent anxiety and worry (ICD-11/DSM-5). These duration thresholds serve as diagnostic anchors that distinguish acute stress responses from sustained clinical disorders.
SELF-CHECK
A 28-year-old patient presents with recurrent intrusive thoughts about contamination and engages in repeated hand-washing rituals for 3 hours daily. She reports distress about these rituals and recognises them as excessive. Which classification best describes her condition?
A. Psychotic disorder — she has lost reality contact
B. Neurotic-spectrum disorder — she has preserved insight and reality contact
C. Organic disorder — her compulsions have a physical cause
D. Personality disorder — this is a character trait, not a disease
Reveal Answer
Answer: B. Neurotic-spectrum disorder — she has preserved insight and reality contact
OCD belongs to the neurotic spectrum (ICD-11: Obsessive-compulsive or related disorders). The key distinguishing feature here is preserved insight — the patient recognises her rituals as excessive and irrational. In psychotic disorders, insight is characteristically impaired. Organic disorders require a demonstrable physical cause. This is not a personality trait but an Axis I condition with episodic features.
Organic versus Non-Organic (Functional) Psychiatric Disorders
The second major classificatory axis in psychiatry is the distinction between organic and non-organic (functional) disorders — a dimension that every general physician must master, because failure to identify an organic cause of psychiatric symptoms is one of the most consequential diagnostic errors in clinical medicine.
Provided image
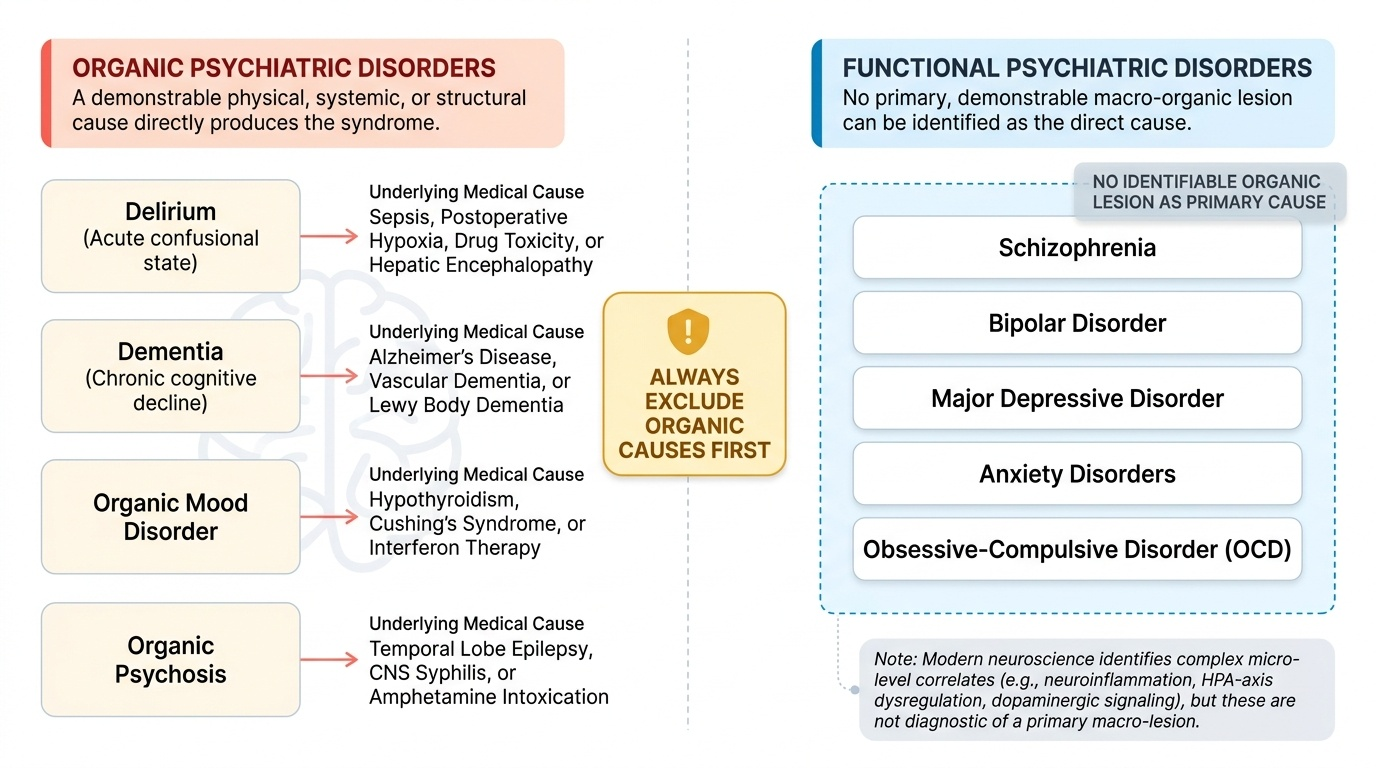
Organic psychiatric disorders are those in which a demonstrable physical cause — a systemic medical condition, a primary brain lesion, a substance, or a medication — directly produces the psychiatric syndrome. The organic cause is not merely an aggravating factor; it is the necessary and sufficient cause of the mental disorder. Examples include delirium (acute confusional state arising from sepsis, postoperative hypoxia, hepatic encephalopathy, or drug toxicity), dementia (chronic, progressive cognitive decline in Alzheimer's disease, vascular dementia, or Lewy body dementia), organic mood disorder (depression secondary to hypothyroidism, Cushing's syndrome, or interferon therapy), organic psychosis (psychotic features from temporal lobe epilepsy, CNS syphilis, or amphetamine intoxication), and substance use disorders with intoxication and withdrawal states. In the ICD-11, these are grouped under 'Mental or behavioural disorders due to use of psychoactive substances' and the 'Neurocognitive disorders' chapter.
Non-organic (functional) psychiatric disorders are those in which no such demonstrable organic lesion can be identified as the primary cause. The term 'functional' historically meant 'of unknown or psychosocial origin,' though contemporary neuroscience is rapidly identifying neurobiological correlates of conditions previously considered purely functional — for example, the neuroinflammatory and HPA-axis dysregulation in depression, and the dopaminergic dysregulation hypothesis in schizophrenia. The term should therefore be understood to mean 'no currently identifiable organic lesion sufficient to explain the syndrome,' not 'not real' or 'without biological basis.' Schizophrenia, bipolar disorder, major depressive disorder, anxiety disorders, and OCD are the major functional disorders — they cause profound disability, respond to specific pharmacological and psychological treatments, and have substantial genetic and neurobiological substrates.
The clinical implication for the general physician is straightforward but critically important: always investigate for organic causes first, particularly in presentations that are atypical (e.g. first psychotic episode in a middle-aged or elderly patient without prior psychiatric history, depression of sudden onset with constitutional symptoms, or cognitive changes with focal neurological signs). A thyroid function test, blood glucose, liver function tests, serum B12/folate, and urine toxicology screen should be part of the standard workup for any new psychiatric presentation in a general medical setting.