Page 2 of 13
PS1.1 | Psychiatric Classification Foundations — SDL Guide (Part 2)
ICD-11 Structural Overview: Major Categories and Their Organisation
The ICD-11 Chapter 6 (Mental, behavioural, or neurodevelopmental disorders) organises psychiatric conditions into a hierarchical classification that reflects current scientific understanding of disorder groupings while maintaining practical clinical utility. Understanding the broad architecture of this chapter helps the clinician navigate between categories and recognise the rationale for placing specific disorders where they are.
Provided image
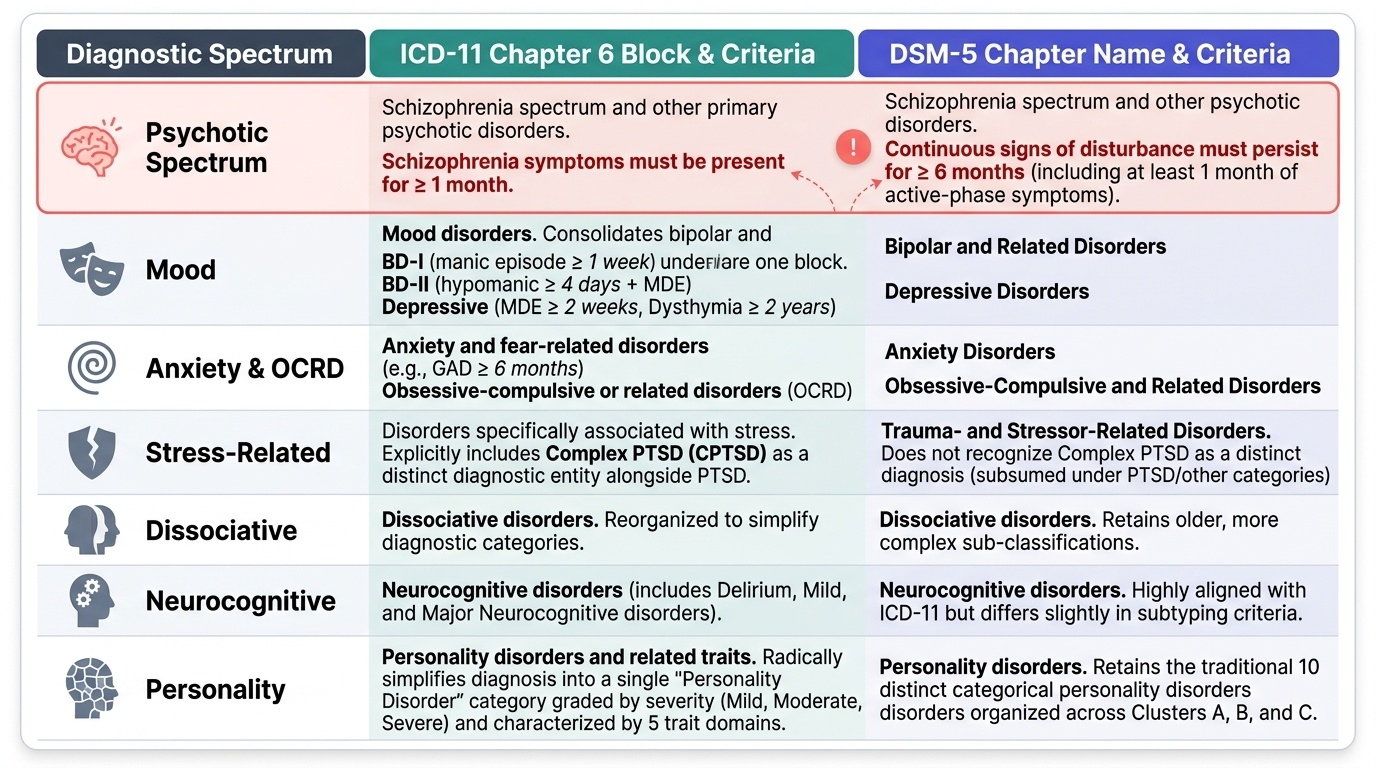
The major blocks within ICD-11 Chapter 6 are as follows, moving from neurodevelopmental through stress-related, dissociative, somatic, feeding, elimination, body-image, impulse-control, substance, neurocognitive, and personality spectra. The key blocks relevant to PS1.1 are:
1. Neurodevelopmental disorders — include intellectual developmental disorders, autism spectrum disorder (ASD), attention-deficit hyperactivity disorder (ADHD), specific learning disorders, and developmental motor disorders. These manifest early in development and are characterised by deficits in the acquisition or application of developmental functions.
2. Schizophrenia spectrum and other primary psychotic disorders — the core psychotic disorders including schizophrenia (≥1 month of positive symptoms per ICD-11), schizoaffective disorder, delusional disorder, acute and transient psychotic disorder (<1 month), and schizotypal disorder. Positive symptoms (hallucinations, delusions, disorganised thinking) and negative symptoms (flat affect, alogia, avolition, anhedonia) are the defining features.
3. Mood disorders (bipolar type, depressive type) — bipolar disorders (BD-I requiring at least one manic episode lasting ≥1 week or requiring hospitalisation; BD-II requiring at least one hypomanic episode ≥4 days and one MDE without full mania) and depressive disorders (MDE ≥2 weeks; persistent depressive disorder/dysthymia ≥2 years).
4. Anxiety and fear-related disorders — generalised anxiety disorder (GAD ≥6 months), panic disorder, agoraphobia, specific phobias, social anxiety disorder, separation anxiety disorder.
5. Obsessive-compulsive or related disorders (OCRD) — OCD, body dysmorphic disorder, hoarding disorder, trichotillomania, excoriation disorder.
6. Disorders specifically associated with stress — post-traumatic stress disorder (PTSD), complex PTSD, adjustment disorder, prolonged grief disorder.
7. Dissociative disorders — dissociative neurological symptom disorder (formerly conversion disorder), dissociative amnesia, depersonalisation-derealisation disorder.
8. Feeding or eating disorders — anorexia nervosa, bulimia nervosa, binge-eating disorder.
9. Substance use and addictive disorders — including alcohol, opioids, cannabis, stimulants, sedatives; ICD-11 also includes gaming disorder under this chapter.
10. Neurocognitive disorders — delirium, dementia (Alzheimer's, vascular, frontotemporal, Lewy body, etc.).
11. Personality disorders — ICD-11 introduces a dimensional approach with a severity specifier (mild, moderate, severe) plus optional trait domain qualifiers (negative affectivity, detachment, dissociality, disinhibition, anankastia, borderline pattern).
The DSM-5 covers similar territory but organises some categories differently. Most notably, DSM-5 requires a total illness duration of ≥6 months for a schizophrenia diagnosis (including prodromal and residual phases), compared to ICD-11's ≥1 month of core positive symptoms. DSM-5 also retains a distinct 'Somatic symptom and related disorders' chapter that partially corresponds to ICD-11's 'Bodily distress disorders.'
SELF-CHECK
A 60-year-old retired teacher with no prior psychiatric history presents with a 3-week history of auditory hallucinations and paranoid delusions. Blood investigations reveal serum TSH of 0.01 mU/L (suppressed). What is the most appropriate next step?
A. Start antipsychotic medication immediately and refer to psychiatry
B. Diagnose schizophrenia — the 1-month duration threshold has not been met yet
C. Treat hyperthyroidism first; investigate for organic psychosis
D. Diagnose brief psychotic disorder and observe for 1 month
Reveal Answer
Answer: C. Treat hyperthyroidism first; investigate for organic psychosis
This presentation is a red flag for organic psychosis — a first psychotic episode in an elderly patient with suppressed TSH (indicating hyperthyroidism, which can cause organic psychosis). Organic causes must be ruled out before attributing psychotic symptoms to a primary psychiatric disorder. Treating the underlying hyperthyroidism may resolve the psychosis without antipsychotics. Schizophrenia and brief psychotic disorder are diagnoses of exclusion — organic aetiology must be systematically excluded first.
Mechanisms and Principles Underlying Psychiatric Classification
The neuroscientific and phenomenological principles underlying modern psychiatric classification are essential for understanding why disorders are grouped as they are, and why the same classification system needs periodic revision as scientific knowledge advances. This section traces the key mechanisms that inform the current nosological framework.
Phenomenological principle: ICD-11 and DSM-5 both adopt a descriptive, atheoretical approach — disorders are defined by their observable phenomenology (what the patient experiences and reports, what the clinician observes) rather than by presumed aetiology. This was a deliberate decision in DSM-III (1980) and has been maintained through subsequent editions to avoid embedding potentially incorrect aetiological theories into the diagnostic criteria. The practical implication is that two patients with identical symptom profiles receive the same diagnosis, regardless of whether one has a strong family history and the other does not, or whether one has identifiable psychosocial stressors and the other does not.
Multi-axial history and dimensional shifts: DSM-IV used a multi-axial system (Axis I: clinical disorders; Axis II: personality and intellectual developmental disorders; Axis III: general medical conditions; Axis IV: psychosocial stressors; Axis V: Global Assessment of Functioning). DSM-5 integrated axes I-III into a single diagnostic system, reflecting that the distinction between 'mental' and 'physical' illness is scientifically arbitrary. ICD-11 similarly integrates conditions across its chapters. Both systems are moving toward dimensional assessment of symptom severity alongside categorical diagnosis — recognising that 'caseness' versus 'no caseness' is a spectrum rather than a binary.
Neurobiological correlates: The major neurotransmitter hypotheses — the dopaminergic hypothesis of schizophrenia (excess mesolimbic dopamine activity producing positive symptoms; mesocortical dopamine deficiency producing negative symptoms), the monoamine hypothesis of depression (deficiency of serotonin, noradrenaline, and/or dopamine), and the GABAergic/glutamatergic dysregulation in anxiety disorders — represent simplified but clinically useful frameworks. They explain, at least partially, why dopamine D2 antagonists (typical antipsychotics) and D2/D3 partial agonists (atypical antipsychotics) treat psychosis, while selective serotonin reuptake inhibitors (SSRIs) treat depression and anxiety. These neurobiological substrates also explain some of the overlap between categories — for example, severe depression and bipolar disorder share abnormalities in the HPA axis and monoamine systems.
Cultural and contextual sensitivity: The ICD-11 explicitly incorporates cultural formulation — the recognition that symptoms must be interpreted within the patient's cultural context. What constitutes a fixed false belief (delusion) in one cultural setting may be a culturally sanctioned belief in another. ICD-11's cross-cultural field studies, including studies from India, have informed the revised criteria to be more applicable across diverse populations than earlier versions.
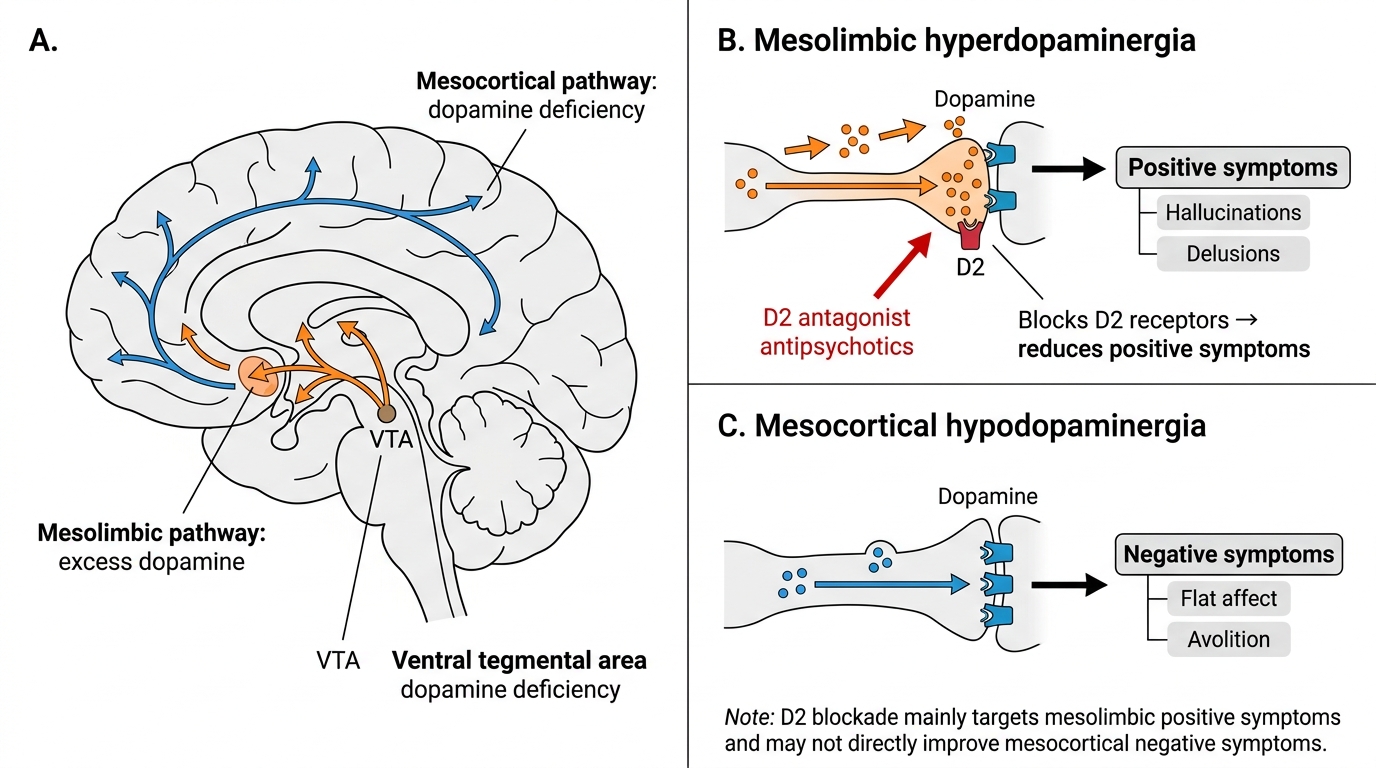
Dopaminergic Hypothesis of Schizophrenia
Clinical Significance: Applying Classification at the Bedside
The clinical utility of psychiatric classification manifests at multiple levels — from the individual patient encounter to the population health and policy context. A clinician who can confidently apply classification principles to a psychiatric presentation will make better diagnostic, investigative, and therapeutic decisions across all clinical settings.
At the individual patient level, classification directly guides management. Identifying a disorder as organic (e.g. hepatic encephalopathy producing delirium) versus functional (e.g. schizophrenia) determines whether definitive treatment is directed at the underlying medical condition versus psychiatric pharmacotherapy. Within functional disorders, distinguishing psychotic from neurotic conditions determines whether antipsychotic therapy is indicated. The classification of a mood episode as part of unipolar depression versus bipolar disorder (which requires documentation of at least one manic or hypomanic episode in the patient's lifetime history) has major therapeutic implications — prescribing an antidepressant alone in bipolar disorder without a mood stabiliser can trigger hypomania or rapid cycling.
At the medicolegal level, classification interfaces with the Mental Healthcare Act 2017 (India), which replaced the Mental Health Act 1987. The Act defines 'mental illness' as a 'substantial disorder of thinking, mood, perception, orientation or memory that grossly impairs judgment, behaviour, capacity to recognise reality or ability to meet the ordinary demands of life' — a definition consistent with the psychotic and severe mood disorder categories. The Act decriminalised suicide attempt (section 115), established rights of persons with mental illness, introduced the concept of advance directives and nominated representatives, and mandated free treatment for persons with mental illness in government hospitals. Classification determines which patients are covered by these provisions.
At the epidemiological level, standardised classification enables international comparison of psychiatric morbidity, the measurement of disease burden (disability-adjusted life years, DALYs), the evaluation of public health interventions, and the rational allocation of mental health resources. The WHO's Global Burden of Disease studies use ICD coding as the primary data source, and these data directly influence health policy and resource allocation in India and globally.
Practical application — a systematic diagnostic approach: When encountering a patient with possible psychiatric symptoms, the clinician should follow this sequence: (1) Rule out organic causes (medical history, physical examination, targeted investigations); (2) Characterise the primary syndrome (psychotic features present? mood disturbance? anxiety? cognitive impairment?); (3) Assess severity and functional impairment; (4) Determine duration to apply threshold criteria; (5) Apply ICD-11 or DSM-5 criteria systematically; (6) Consider comorbidity (psychiatric comorbidity is the rule rather than the exception — e.g. depression commonly co-occurs with anxiety disorders, and substance use disorders frequently co-occur with mood and psychotic disorders).
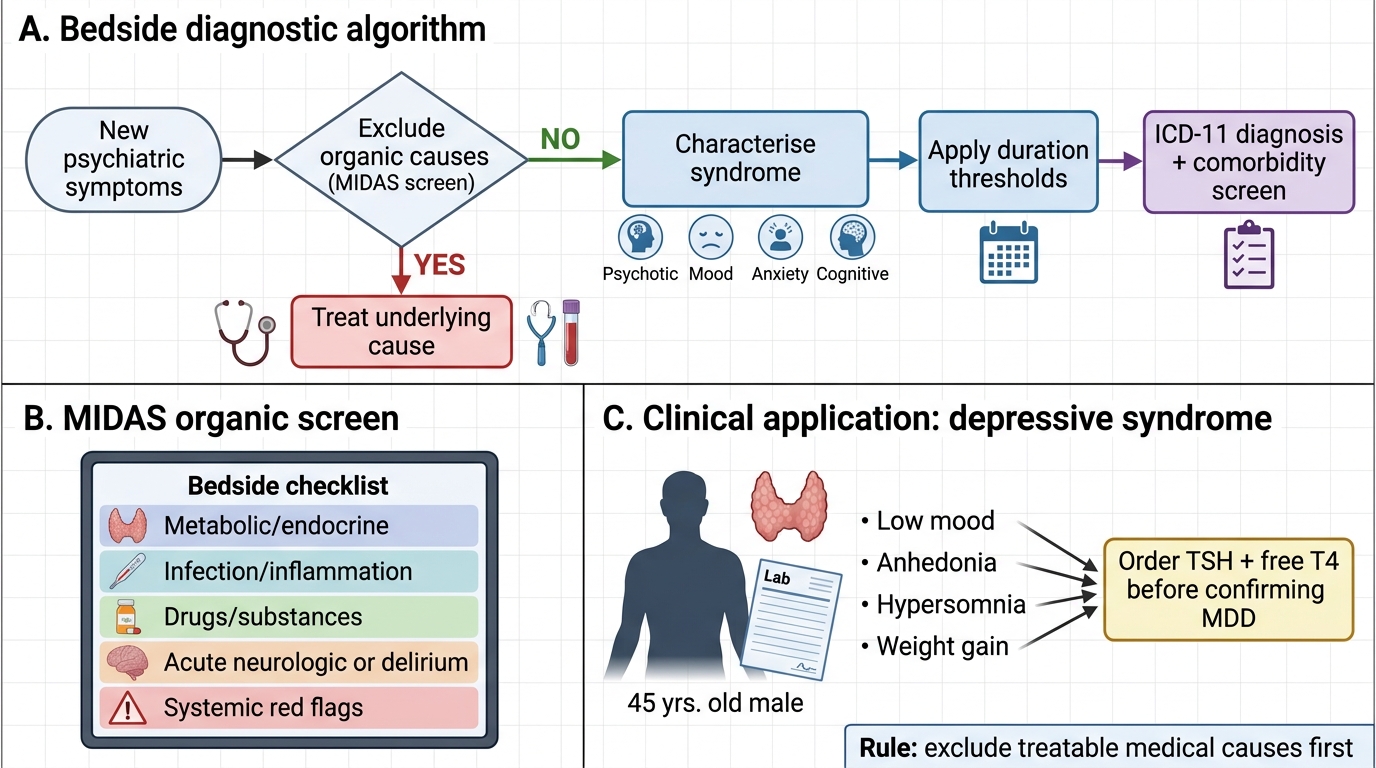
Bedside Algorithm for a New Psychiatric Presentation
SELF-CHECK
A 45-year-old man with known Type 2 diabetes mellitus and hypertension presents with a 3-month history of low mood, anhedonia, hypersomnia, and weight gain. Which investigation is most critical to order before confirming a diagnosis of major depressive disorder?
A. Complete blood count and ESR
B. Thyroid function tests (TSH and free T4)
C. ECG and echocardiogram
D. HbA1c and fasting lipid profile
Reveal Answer
Answer: B. Thyroid function tests (TSH and free T4)
Hypothyroidism is a common and easily treatable organic cause of depressive syndrome, especially in patients with other metabolic conditions like diabetes and hypertension. Thyroid function tests (TSH is the most sensitive screen) must be checked before attributing low mood to primary major depressive disorder. Treating hypothyroidism may fully resolve the depressive syndrome without antidepressants. This exemplifies the organic-versus-functional rule: always exclude medical causes first.