Page 1 of 11
PS5.1-2 | Depression in Primary Care — SDL Guide
Learning Objectives
- Recognise the core clinical features of a major depressive episode (ICD-11/DSM-5) and elicit a structured psychiatric history
- Apply the diagnostic criteria — including the ≥2-week duration threshold — to confirm or exclude major depressive disorder at the primary-care level
- Identify red-flag signs that mandate urgent specialist referral, including active suicidality, psychotic features, severe functional impairment, suspected bipolarity, and treatment resistance
- Select SSRIs as the first-line pharmacological treatment and counsel the patient on onset of action, duration of therapy, and adherence
- Distinguish serotonin syndrome from neuroleptic malignant syndrome based on clinical features
- Apply relevant provisions of the Mental Healthcare Act 2017 in the management of a depressed patient
INSTRUCTIONS
Depression is the single most common psychiatric disorder encountered at the primary-care interface, and the majority of patients with a depressive illness will first present — and continue to receive care — outside a specialist psychiatric setting. As a MBBS graduate working at a district hospital, PHC, or rural health centre, you are often the only clinician available to diagnose depression, initiate treatment, and recognise when a case exceeds the scope of primary care. This module equips you with the clinical reasoning, pharmacological knowledge, and referral thresholds needed to provide safe, guideline-concordant depression care from day one of independent practice.
References
- Ahuja N. A Short Textbook of Psychiatry, 8th ed. New Delhi: Jaypee; 2022. Ch 7 (Mood Disorders) (textbook)
- Kaplan HI, Sadock BJ. Synopsis of Psychiatry, 11th ed. Philadelphia: Wolters Kluwer; 2015. Ch 8 (textbook)
- Mental Healthcare Act 2017. Government of India. Ministry of Law and Justice. (guideline)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 38-year-old schoolteacher presents to your PHC with a six-week history of persistent low mood, early-morning awakening, loss of appetite, and inability to concentrate on her work. She has stopped attending social events she previously enjoyed and confides, 'I feel like everything I do is worthless.' Her husband reports that she has been tearful most days and has made vague comments about 'not wanting to be here.' You have ten minutes before the next patient. What is the most important thing to do first, and what is the most dangerous thing you could miss?
WHY THIS MATTERS
Major depressive disorder (MDD) is the leading cause of disability worldwide and the commonest psychiatric diagnosis in primary-care settings in India. The Global Burden of Disease study estimates that depression accounts for more years lived with disability than any other single condition. Yet fewer than one in five people with depression in India receive any treatment — the 'treatment gap' — largely because diagnosis and first-contact management must happen at the level of the general practitioner. As an MBBS graduate working in primary care, you will encounter patients with unrecognised depression embedded in presentations of chronic pain, fatigue, diabetes, or non-specific somatic complaints. Recognising the disorder, initiating safe first-line treatment, and identifying when to refer can dramatically reduce suffering and prevent suicide.
RECALL
Before proceeding, activate what you already know. In PY you studied the limbic system, the role of the prefrontal cortex in mood regulation, and the monoamine neurotransmitters — serotonin, norepinephrine, and dopamine — whose dysregulation forms the neurobiological basis of depression. In PH you learnt the pharmacology of tricyclic antidepressants (TCAs) and monoamine oxidase inhibitors (MAOIs). You will now build on that foundation to understand why modern first-line treatment has moved to selective serotonin reuptake inhibitors (SSRIs) and how their mechanism, safety profile, and tolerability make them preferable for primary care.
Clinical Presentation of a Depressive Episode
Depression presents along a spectrum, but the entry-point for every assessment is recognising the core symptoms of a major depressive episode as codified by both ICD-11 and DSM-5. Central to both diagnostic systems is the concept that symptoms must be present for a minimum of two weeks, represent a change from previous functioning, and cause clinically significant distress or impairment in social, occupational, or other important areas of functioning. The two anchor symptoms are persistently depressed mood (most of the day, nearly every day) and markedly diminished interest or pleasure in activities once found enjoyable — this second feature is termed anhedonia and is one of the most clinically reliable signs of a true depressive episode rather than ordinary sadness.
In addition to the two anchor symptoms, ICD-11 identifies a set of associated features that the clinician must actively enquire about: changes in appetite or weight (increase or decrease), disruption of sleep (early-morning awakening is particularly characteristic), psychomotor retardation or agitation (observable to others, not merely subjective), fatigue and loss of energy, feelings of worthlessness or excessive guilt, difficulty concentrating or making decisions, and recurrent thoughts of death or suicide. DSM-5 requires five or more symptoms from this list to be present during the same two-week period, with at least one being depressed mood or anhedonia. ICD-11 uses a similar, though not identical, threshold.
In clinical practice, Indian patients frequently present with somatic equivalents of depression — persistent headache, backache, abdominal discomfort, or palpitations — with the affective component minimised or absent from the initial complaint. This is sometimes described as 'masked depression'. The skilled primary-care clinician learns to screen for mood symptoms even when the presenting complaint appears entirely physical.
IMPORTANT NOTE on duration: the ≥2-week threshold applies to a major depressive episode. Briefer episodes that do not meet duration criteria do not qualify for this diagnosis, although they still deserve compassionate attention and may meet criteria for other diagnoses such as adjustment disorder.
IMPORTANT NOTE on system: whenever you state a diagnostic criterion, be explicit about which classification system you are applying (ICD-11 vs DSM-5), because the threshold numbers and symptom counts differ subtly between them.
SELF-CHECK
A 45-year-old man reports persistently depressed mood, anhedonia, early-morning awakening, loss of appetite, and feelings of worthlessness for the past 10 days. He is significantly impaired at work. Which statement about his diagnosis is most accurate?
A. He meets DSM-5 criteria for major depressive disorder because he has five core symptoms
B. He does not yet meet criteria for a major depressive episode because the duration is less than two weeks
C. The diagnosis requires a serum serotonin level to confirm the monoamine deficiency
D. ICD-11 requires at least eight symptoms to diagnose a major depressive episode
Reveal Answer
Answer: B. He does not yet meet criteria for a major depressive episode because the duration is less than two weeks
Both ICD-11 and DSM-5 require symptoms to be present for at least two weeks to diagnose a major depressive episode. This patient has only 10 days of symptoms, so the duration criterion is not yet met, regardless of the number or severity of symptoms. There is no blood test for depression — it is a clinical diagnosis. ICD-11 does not require eight symptoms.
Psychopathology and Aetiology of Depression
Understanding why a patient becomes depressed requires integrating several levels of explanation, from molecular biology to social circumstance. The dominant neurobiological model — the monoamine deficiency hypothesis — proposes that depression results from functional deficiency of monoamine neurotransmitters, particularly serotonin and norepinephrine, at central synapses. This hypothesis is supported by the observation that drugs that deplete monoamines (e.g. reserpine) can precipitate depression, while antidepressants that increase monoamine availability (SSRIs, SNRIs, TCAs, MAOIs) alleviate it. However, the delayed clinical response (2–4 weeks) despite rapid reuptake inhibition has prompted refinement of this model: current understanding emphasises downstream neuroplasticity changes, including upregulation of BDNF (brain-derived neurotrophic factor) and synaptic remodelling, as the actual mechanism of therapeutic effect.
The aetiology of depression is best understood through the biopsychosocial model, which integrates three interacting domains. Biological factors include genetic predisposition (heritability ~40%), female sex, medical comorbidities (hypothyroidism, chronic pain, post-myocardial infarction state, Parkinson's disease), medications (corticosteroids, beta-blockers, interferon, oral contraceptives), and substance use. Psychological factors include neuroticism as a personality trait, a history of childhood adversity or abuse, a previous depressive episode (the single strongest predictor of recurrence — approximately 50% of people who have one episode will have a second), and maladaptive cognitive schemas such as Beck's cognitive triad of negative views of self, world, and future. Social factors include stressful life events (bereavement, job loss, relationship breakdown), social isolation, poverty, and chronic interpersonal conflict.
The concept of kindling deserves specific mention: with each successive depressive episode, less psychosocial stress is required to trigger the next one, and episodes may eventually become autonomous and self-perpetuating. This is one of the key arguments for maintenance antidepressant therapy after recovery from a first severe episode.
For the primary-care physician, the practical take-away from understanding aetiology is twofold: first, actively screen for and treat reversible medical and pharmacological causes of depression before labelling a patient with primary MDD; second, recognise that effective treatment must address biological, psychological, and social determinants — medication alone is rarely sufficient for sustained recovery.
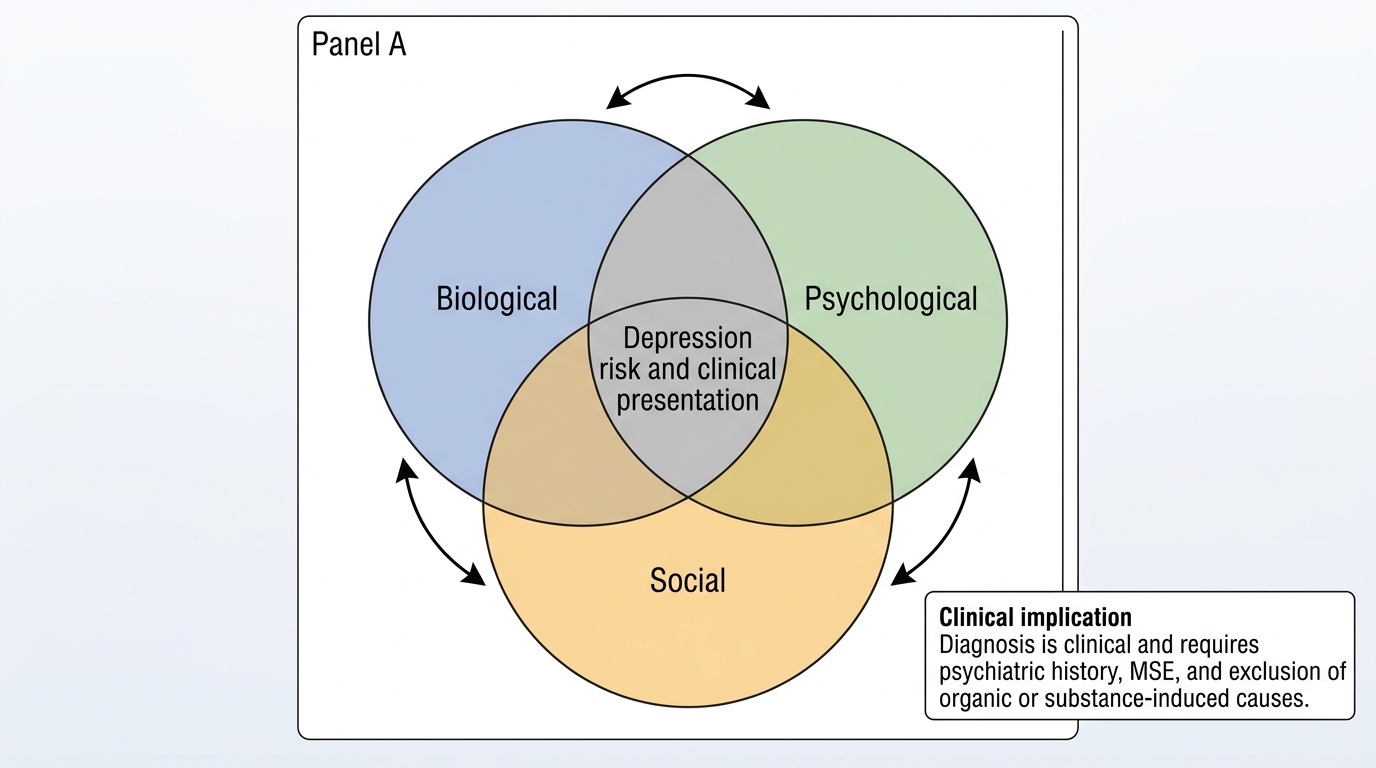
Biopsychosocial Model of Depression
Diagnosis and Mental Status Examination in Depression
The diagnosis of depression is entirely clinical — there is no biomarker or imaging test that confirms the disorder. The primary-care physician makes the diagnosis through a structured psychiatric history, a targeted mental status examination (MSE), and the exclusion of organic and substance-induced causes. The history should cover the onset, duration, and progression of symptoms; previous depressive or hypomanic episodes; family history of mood disorders; current medications (including non-prescription drugs and herbal preparations); and psychosocial circumstances.
Provided image
The mental status examination is the psychiatric equivalent of the physical examination and must be performed for every patient presenting with possible depression. In the domain of appearance and behaviour, the examiner notes psychomotor retardation (slowed movement and speech), poor eye contact, neglected self-care, and the overall level of distress. Speech in depression is characteristically reduced in quantity (poverty of speech), slow in rate, and low in volume. Mood is assessed both subjectively (asking 'How are you feeling in yourself?') and objectively by the examiner's observation — mood is described as depressed, low, or dysphoric. Affect is the observable expression of emotional state; in depression it is constricted and may be blunted, with reduced variability and reactivity. Thought form is typically slowed (retarded) rather than formal-thought-disordered; thought content may include themes of worthlessness, guilt, hopelessness, and suicidal ideation. Perceptions: hallucinations are not a feature of uncomplicated depression, though mood-congruent psychotic features (e.g. auditory hallucinations of a persecutory or self-critical nature) may occur in severe depression with psychotic features. Cognition shows difficulty with concentration and attention but not global dementia. Insight is usually preserved in depression, unlike in mania.
Assessment of suicidal ideation is not optional — it is a mandatory component of every assessment of a depressed patient. The SLAP framework (Specificity of plan, Lethality of method, Availability of means, Proximity of rescue) provides a structured approach to risk stratification. Passive death wishes ('I wish I were not here') carry lower immediate risk than active suicidal ideation with a specific plan and access to means (e.g. stockpiled medications, firearm availability).
Organic exclusion: basic investigations warranted include TSH (hypothyroidism as a reversible cause), full blood count, renal and liver function, blood glucose (diabetes and depression are bidirectionally related), and urine toxicology where substance use is suspected.
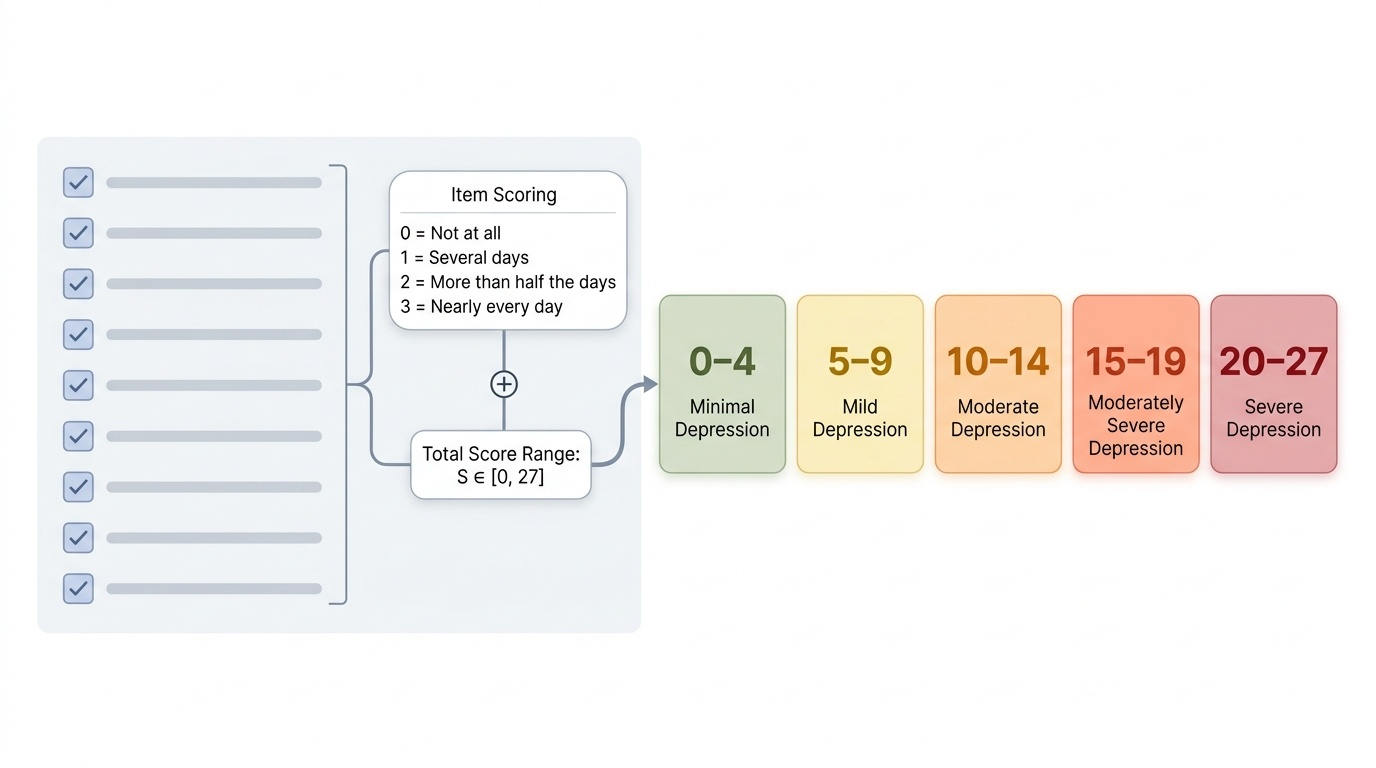
The PHQ-9 (Patient Health Questionnaire-9) is a validated, freely available screening and monitoring tool in the public domain, easily administered in primary care. A score ≥10 is the standard threshold for probable major depression; it also tracks treatment response over time.
SELF-CHECK
During the mental status examination of a depressed patient, you observe slow, monotonous speech, minimal spontaneous movement, and a flat facial expression. The patient reports feeling 'completely empty.' Which component of the MSE best captures the observable expression of his emotional state?
A. Mood
B. Affect
C. Thought content
D. Insight
Reveal Answer
Answer: B. Affect
Affect is the observable, objective expression of the emotional state as seen by the examiner (flat, constricted, blunted, reactive). Mood is the subjective internal emotional experience as reported by the patient ('completely empty'). Thought content refers to what the patient is thinking about (e.g. themes of guilt or suicidality). Insight refers to the patient's awareness of being ill.