Page 2 of 11
PS5.1-2 | Depression in Primary Care — SDL Guide (Part 2)
Management of Depression at the Primary-Care Level
The management of a depressive episode in primary care combines pharmacological treatment, psychoeducation, simple psychological support, and social interventions. The overall goal is full remission (not merely response), sustained over time, with return to pre-illness functioning.
Pharmacological treatment — SSRIs as first-line agents. The selective serotonin reuptake inhibitors (SSRIs) are the first-line pharmacological treatment for depression in primary care, recommended by WHO Essential Medicines, NICE guidelines, and Indian expert consensus. Their superiority to TCAs and MAOIs as first-line agents rests on four pillars: comparable efficacy, substantially improved tolerability, a far wider therapeutic window (much safer in overdose — a critical consideration when prescribing to a potentially suicidal patient), and once-daily dosing that supports adherence. Available SSRIs in Indian primary-care settings include escitalopram (10–20 mg/day), sertraline (50–200 mg/day), fluoxetine (20–60 mg/day), and paroxetine (20–50 mg/day). Escitalopram and sertraline are generally preferred because of their minimal pharmacokinetic drug interactions (important in multimorbid patients on other medications).
All SSRIs share a class of common initial adverse effects — nausea, headache, insomnia, and sexual dysfunction — which typically improve after the first 2–4 weeks. There is a critically important risk of behavioural activation or increased suicidal ideation in the first 1–4 weeks of SSRI initiation, particularly in adolescents and young adults; all patients and their families must be counselled about this before the first prescription, and a review appointment should be scheduled within 2 weeks of starting.
The antidepressant effect does not onset immediately; patients should be counselled that clinical improvement typically begins at 2–4 weeks and the full therapeutic effect may not be apparent for 6–8 weeks. Premature discontinuation due to perceived lack of effect is one of the commonest causes of treatment failure. Once remission is achieved, antidepressant therapy should be continued for at least 6–9 months after remission to prevent relapse; patients with two or more previous episodes require maintenance therapy for 2 years or more, and some require indefinite treatment.
Non-pharmacological approaches. In mild-to-moderate depression, structured psychological interventions — particularly cognitive behavioural therapy (CBT) — are as effective as medication and may have more durable effects. In primary care settings where formal CBT is unavailable, the physician can provide basic behavioural activation (scheduling pleasurable activities, reinstating routine), psychoeducation about the illness, and social problem-solving. Addressing social stressors (economic hardship, domestic conflict) is integral to recovery. Physical exercise has moderate evidence for antidepressant benefit and should be recommended as an adjunct.
Drug safety — serotonin syndrome vs NMS. A prescribing physician must understand the distinction between two serious drug-related complications. Serotonin syndrome is caused by excess serotonergic activity — most commonly from combining two serotonergic agents (e.g. SSRI + tramadol, or SSRI + linezolid). It presents with the triad of altered mental status, autonomic instability, and neuromuscular abnormalities — specifically hyperreflexia and clonus (spontaneous or inducible), with rapid onset (typically within hours of the precipitating drug change). Neuroleptic malignant syndrome (NMS) is caused by dopamine receptor blockade by antipsychotics, presents with lead-pipe muscular rigidity, hyperthermia, bradyreflexia (not hyperreflexia), autonomic instability, and markedly elevated CK, with a much slower onset (days to weeks). These two syndromes share superficial features (hyperthermia, autonomic dysfunction) but are differentiated by the reflex examination: clonus and hyperreflexia in serotonin syndrome, whereas lead-pipe rigidity and bradyreflexia point to NMS. The correct identification matters because treatment differs.
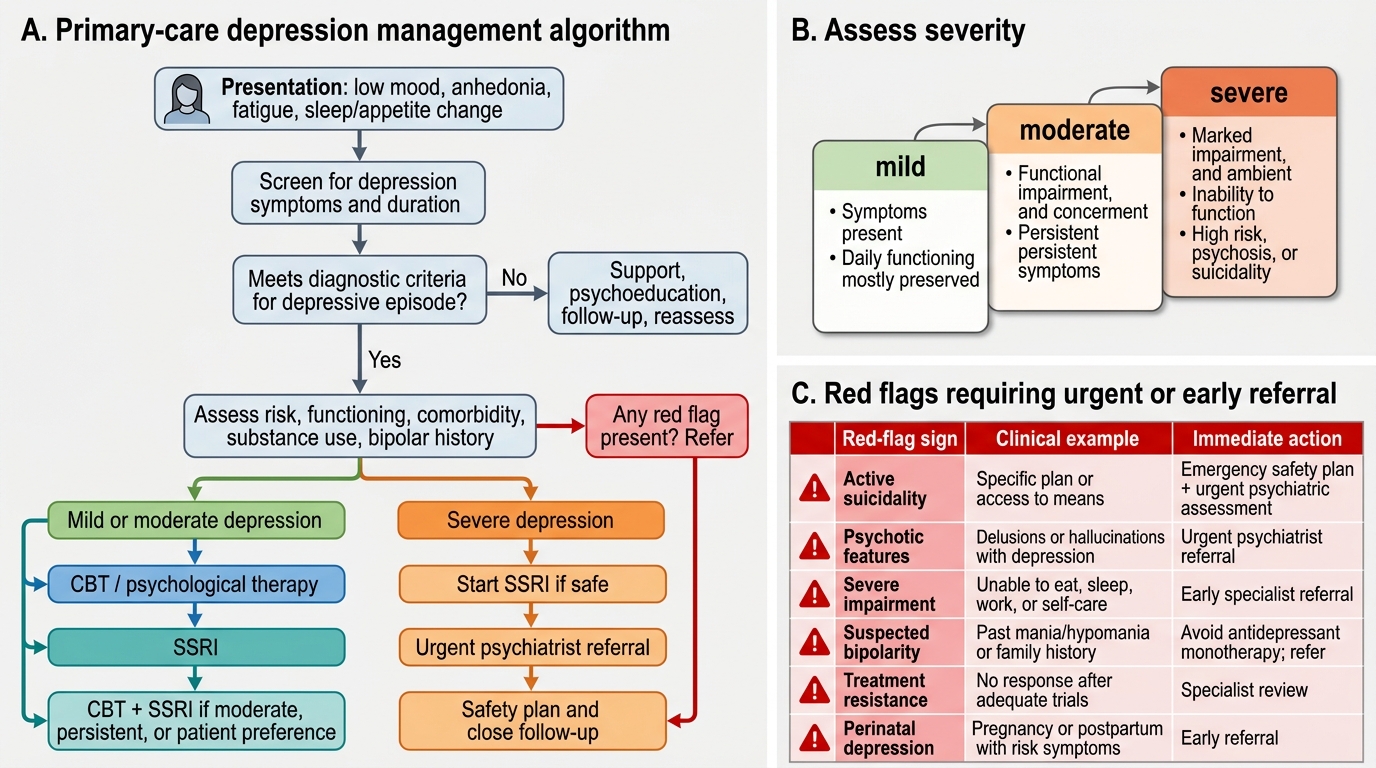
Primary-Care Depression Management Algorithm
Red-Flag Signs and Specialist Referral
A central competency for the primary-care physician is knowing not only how to treat depression, but also when the clinical situation exceeds what is safe to manage without specialist support. The following red-flag signs of depression indicate that urgent or early specialist referral is warranted.
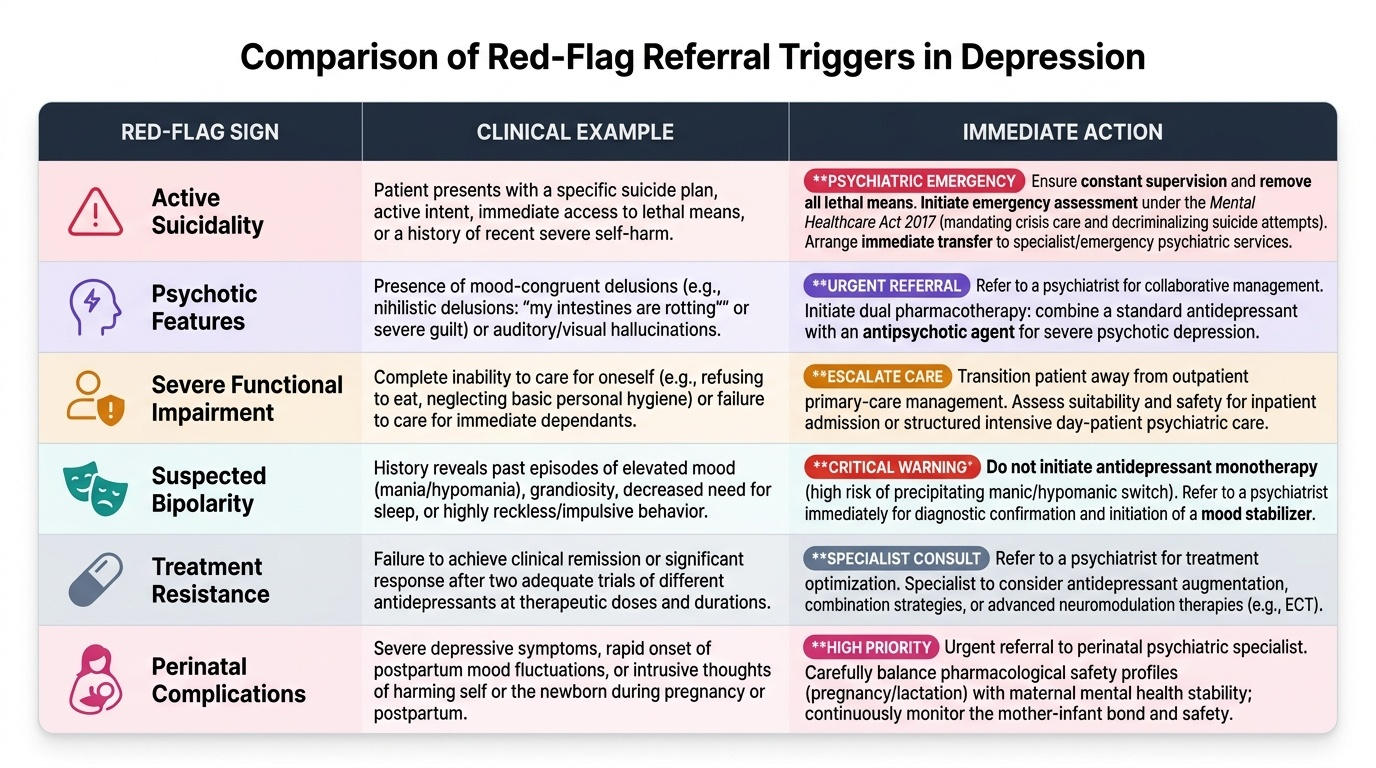
Provided image
First, active suicidality with a specific plan and access to means demands immediate action — this is a psychiatric emergency. The primary-care physician must provide immediate safety planning (removal of means, ensuring constant supervision), and in cases of imminent risk, initiation of emergency assessment under the Mental Healthcare Act 2017. The Mental Healthcare Act 2017 — which replaced the earlier 1987 Act — decriminalises suicide attempts (a critical shift: a person who survives a suicide attempt must not be prosecuted), mandates access to mental health care, and establishes the framework for advance directives and the role of the nominated representative. The primary-care doctor is empowered to initiate emergency assessment and supported admission under this Act.
Second, psychotic features — such as mood-congruent hallucinations or delusions (e.g. nihilistic delusions: 'my intestines are rotting') — indicate psychotic depression, a severe subtype that requires augmentation with an antipsychotic agent alongside the antidepressant. This combination management is best supervised by a psychiatrist.
Third, severe functional impairment — inability to care for oneself (not eating, not maintaining hygiene) or to care for dependants — represents a threshold where outpatient primary-care management is no longer appropriate and inpatient or day-patient psychiatric care should be considered.
Fourth, suspected bipolarity is a critical referral trigger. If the history reveals previous episodes of elevated mood, grandiosity, reduced need for sleep, or reckless behaviour, the current depressive episode may be part of bipolar disorder rather than unipolar depression. Treating bipolar depression with antidepressant monotherapy (without a mood stabiliser) carries a risk of precipitating hypomania or mania, which is potentially hazardous. The distinction is among the most clinically important in psychiatry, and uncertain cases should be referred.
Fifth, treatment resistance — failure to respond to two adequate trials (correct dose, ≥6–8 weeks duration) of different antidepressants — requires specialist evaluation for diagnosis re-evaluation, augmentation strategies, and consideration of electroconvulsive therapy (ECT) in selected cases.
Sixth, pregnancy and the postpartum period introduce additional complexity in both diagnosis (mood symptoms overlap with physiological changes) and treatment (medication safety data, breastfeeding considerations), and should prompt early liaison with psychiatric services.
SELF-CHECK
A 30-year-old patient on sertraline 50 mg/day for depression is also taking tramadol prescribed by an orthopaedic surgeon for back pain. He presents to your clinic with agitation, diaphoresis, and rhythmic jerking of both legs. Which is the most likely diagnosis and which distinguishing feature points to it?
A. Neuroleptic malignant syndrome — the lead-pipe rigidity distinguishes it
B. Serotonin syndrome — the clonus and rapid-onset presentation distinguish it
C. Neuroleptic malignant syndrome — the antidopaminergic drug combination distinguishes it
D. Serotonin syndrome — the bradyreflexia confirms excess serotonergic activity
Reveal Answer
Answer: B. Serotonin syndrome — the clonus and rapid-onset presentation distinguish it
This is serotonin syndrome caused by the combination of sertraline (SSRI) and tramadol (which inhibits serotonin reuptake and has weak agonist activity). The hallmark distinguishing features are hyperreflexia and clonus (the rhythmic leg jerking), rapid onset (within hours of the drug combination), and the serotonergic drug pairing. NMS is caused by antidopaminergic agents, has a slower onset over days to weeks, and presents with lead-pipe rigidity and bradyreflexia, not clonus. Serotonin syndrome features hyperreflexia, not bradyreflexia.
Self-Assessment & Consolidation
At the close of this module, you should be able to apply the full clinical reasoning chain for depression in primary care — from recognition to management to referral — without reference materials. Use the following consolidation prompts to actively test your understanding before your next clinical encounter.
Begin with diagnostic criteria. Can you state, without hesitation, the two anchor symptoms of a major depressive episode, the minimum duration threshold (≥2 weeks per both ICD-11 and DSM-5), and the number of symptoms required by DSM-5? Can you distinguish the subjective (mood) from the objective (affect) component of the MSE, and explain what 'constricted affect' means in observable terms?
Move to aetiological reasoning. When a patient presents with new-onset depression, what three reversible causes should you actively screen for before labelling the disorder as primary MDD? Think: thyroid dysfunction, medications (corticosteroids, beta-blockers, interferon), and substance use. Can you explain the biopsychosocial model to a patient or a colleague in plain language?
Apply your pharmacological knowledge. Why are SSRIs preferred over TCAs as first-line agents in primary care? There are four distinct reasons — efficacy equivalence, better tolerability, superior safety in overdose, and once-daily dosing. At what point in time should you counsel the patient to expect initial improvement (2–4 weeks) and full effect (6–8 weeks)? How long should remission be sustained before medication discontinuation is considered in a first episode (6–9 months)? What must you warn every patient about in the first 1–4 weeks of SSRI initiation (risk of increased suicidal ideation or behavioural activation, especially in young adults)?
Test your red-flag recall. Without looking, can you list all five red-flag signs that mandate specialist referral from primary care? These are: active suicidality with plan and means, psychotic features, severe functional impairment, suspected bipolarity, and treatment resistance after two adequate SSRI trials. Can you explain why treating suspected bipolar depression with antidepressant monotherapy is potentially dangerous?
Confirm your understanding of drug safety. You encounter a patient on an SSRI who develops clonus, hyperreflexia, and diaphoresis shortly after starting a new serotonergic drug. You encounter another patient on haloperidol who develops lead-pipe rigidity, hyperthermia, and elevated CK over three days. Which is which? Serotonin syndrome: clonus + hyperreflexia + fast onset + serotonergic agent. NMS: lead-pipe rigidity + bradyreflexia + slow onset + antidopaminergic agent.
Finally, confirm your knowledge of the Mental Healthcare Act 2017: what right does it restore to individuals who survive a suicide attempt (decriminalisation), and which historical Act does it replace (the 1987 Mental Health Act)?
CLINICAL PEARL
The 'antidepressant failure' that is actually non-adherence. The single commonest reason an SSRI 'doesn't work' is that the patient stopped taking it in the first two weeks — often because of initial side effects (nausea, headache) or because they saw no benefit yet and concluded the drug was ineffective. At every follow-up appointment, explicitly ask: 'Have you taken the tablet every day without missing?' Frame the conversation proactively at initiation: 'You may feel slightly nauseated for the first week or two — this is normal and temporary. You will not feel better immediately; the antidepressant effect builds over 4–8 weeks. Stopping early is the most common reason people don't get better.' Adherence counselling is as pharmacologically important as dose selection.