Page 2 of 9
PS3.1 | Psychoactive Substance Use Disorders — SDL Guide (Part 2)
ICD-11 Diagnostic Concepts: Harmful Use vs Dependence
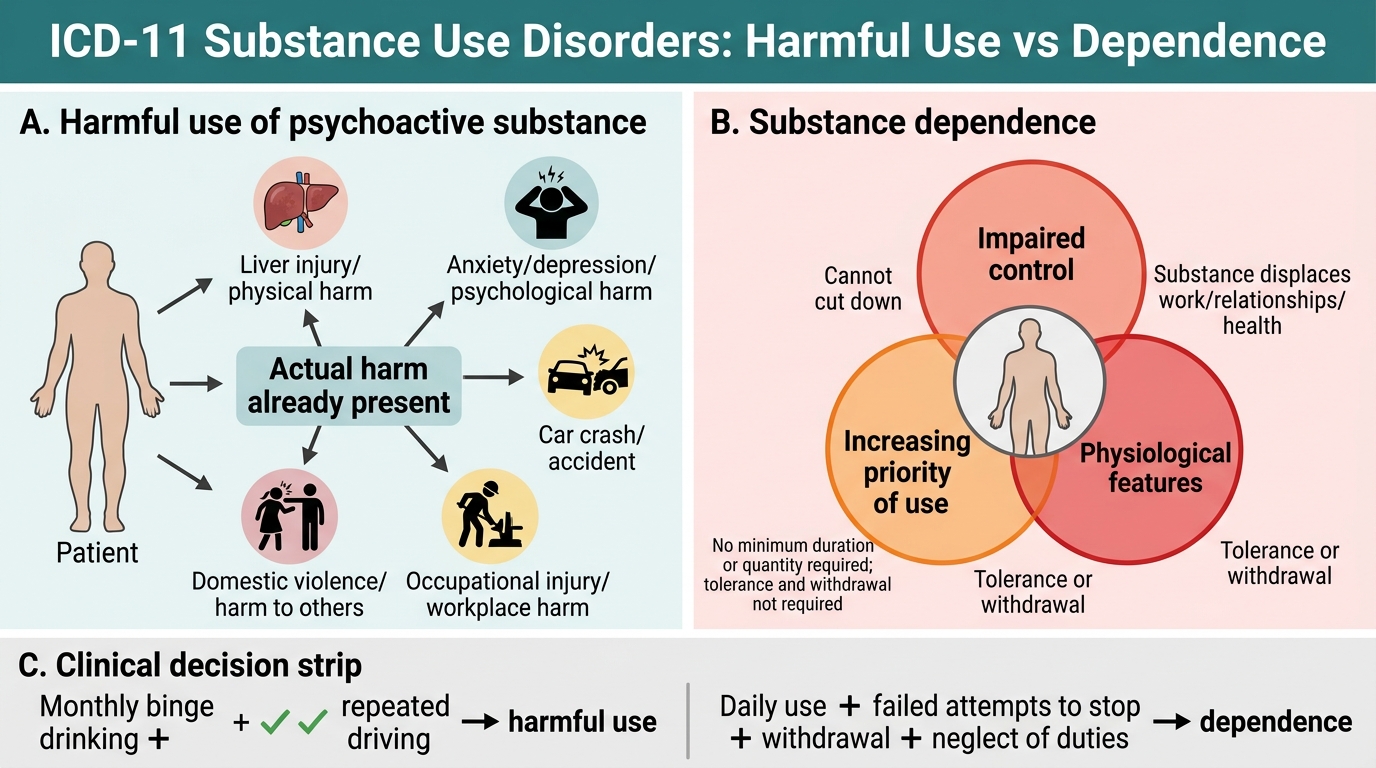
Two fundamental ICD-11 diagnostic categories govern the classification of pathological substance use, and confusing them is a common error. This distinction has clinical, legal, and treatment implications.
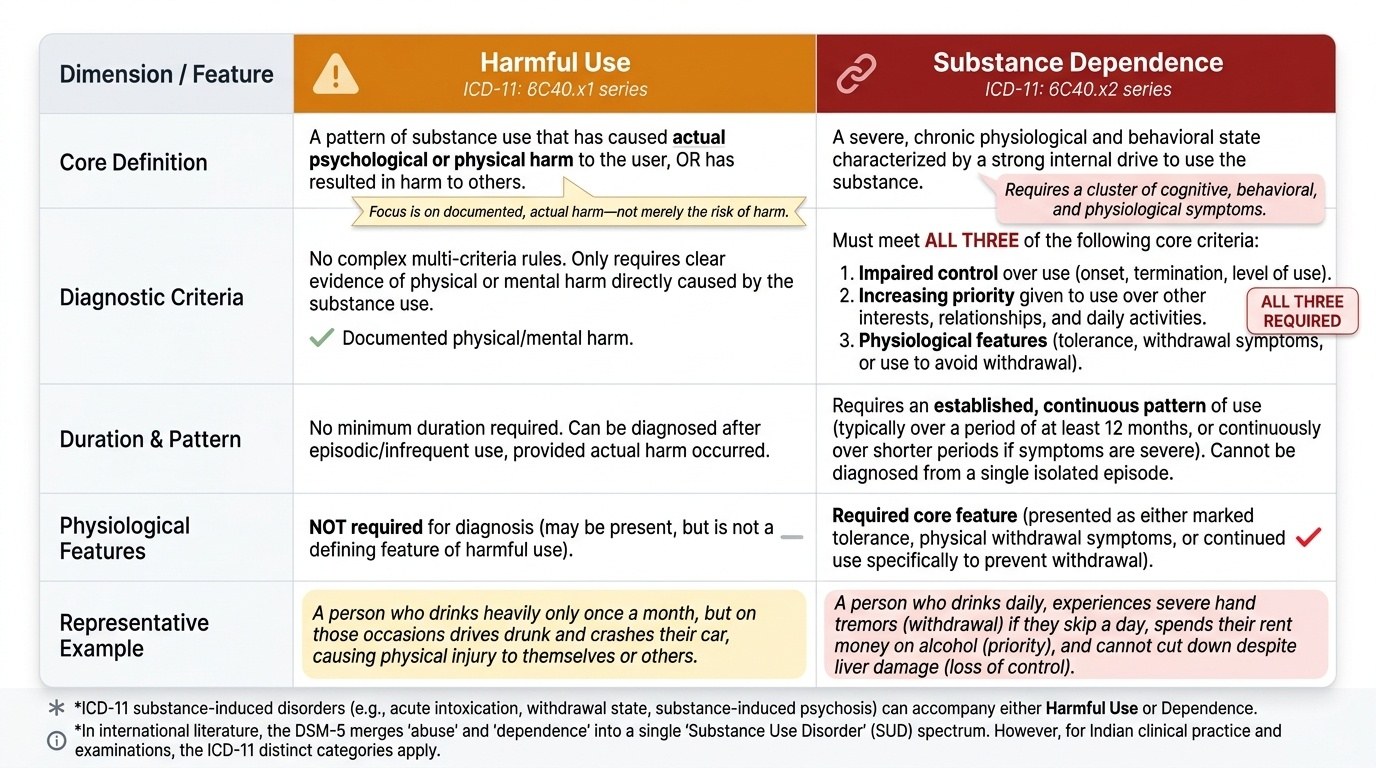
Provided image
Harmful use of a psychoactive substance (ICD-11: 6C40.x1 series) is defined as a pattern of use that has caused actual psychological or physical harm to the user, OR has resulted in harm to others (including accidents, domestic violence, occupational injury). The key feature is actual harm already documented — not merely risk of harm. There is no required minimum duration or quantity. A person who drinks heavily once a month and each time drives drunk may qualify for harmful use even without daily drinking. Tolerance and withdrawal features, while they may be present, are NOT required for the diagnosis of harmful use.
Substance dependence (ICD-11: 6C40.x2 series) is a more severe condition characterised by all three of the following defining criteria:
- Impaired control over substance use (difficulty limiting the quantity, duration, or circumstances of use; unsuccessful attempts to cut down; persistent use despite consequences).
- Increasing priority of substance use relative to other activities and obligations (the substance dominates the person's daily life, displacing work, relationships, and health).
- Physiological features: either tolerance (requiring increasing amounts for the same effect, or diminished effect with the same amount) OR withdrawal symptoms (a characteristic syndrome on dose reduction or cessation), OR continued use to avoid withdrawal.
A critical distinction: you cannot diagnose dependence after a single or occasional episode of heavy use. Dependence requires an established pattern. ICD-11 also introduces the concept of substance-induced disorders (intoxication, withdrawal, psychotic disorder, mood disorder, etc.) as separate diagnoses that can accompany either harmful use or dependence.
The DSM-5 system merges 'abuse' and 'dependence' into a single Substance Use Disorder spectrum (mild/moderate/severe, based on criterion count), which you may encounter in international literature. For NMC examinations and Indian clinical practice, the ICD-11 classification applies.
ICD-11 Harmful Use vs Substance Dependence
Neurobiology and Aetiology of Substance Dependence
Substance dependence is not a moral failing but a brain disorder with a coherent neurobiological basis. Understanding this framework is essential for every clinician: it transforms the clinical interaction from one of moral judgement to one of therapeutics, and it underpins the modern bio-psycho-social model of addiction that guides both Indian and international psychiatric practice. Without this neurobiological grounding, clinicians tend to attribute dependence to weak character — a framing that increases stigma, reduces treatment engagement, and worsens outcomes for patients. With it, dependence becomes as comprehensible as hypertension: a dysregulation of normal physiology, caused by identifiable exposures, modifiable with targeted intervention.
Provided image
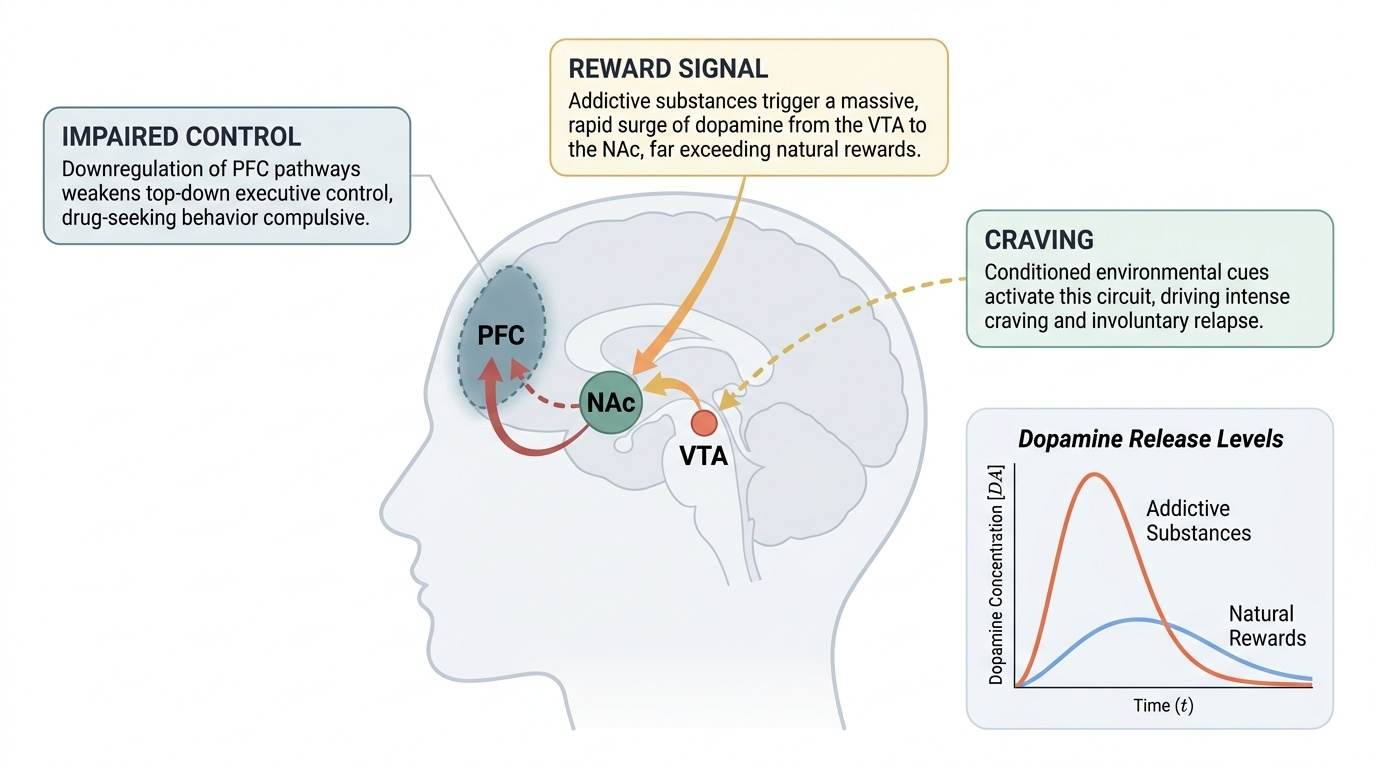
The mesolimbic dopamine reward pathway — running from the ventral tegmental area (VTA) to the nucleus accumbens (NAc) — is the core circuit subverted by virtually all addictive substances. Natural rewards (food, social connection) release modest amounts of dopamine in the NAc. Addictive substances produce a surge of dopamine that is far larger, faster, and more reliable than natural rewards, causing an exaggerated 'reward signal.' With repeated exposure, neuroadaptation occurs:
- Tolerance: dopaminergic and receptor-level downregulation reduces the response to a given dose, necessitating escalation.
- Withdrawal: removal of the substance leaves the brain's natural inhibitory tone (e.g., GABA in alcohol use) severely diminished relative to excitatory tone — producing the hyperexcitable withdrawal syndrome.
- Sensitisation to cues: drug-associated cues (places, people, smells) become powerfully conditioned stimuli that activate the circuit and drive craving even months to years after cessation — explaining relapse.
Aetiology of dependence is multi-factorial:
- Genetic factors account for approximately 40–60% of variance in alcohol dependence risk. Having a first-degree relative with alcohol dependence multiplies risk approximately three-fold. Specific gene variants in alcohol-metabolising enzymes (ADH1B, ALDH2 — the 'Asian flush' allele) confer relative protection due to aversive acetaldehyde accumulation.
- Psychological factors: trauma, adverse childhood experiences, depression, anxiety disorders, and post-traumatic stress disorder are strongly associated with substance use disorders — the 'self-medication' hypothesis.
- Social and environmental factors: availability, affordability, peer norms, occupational stress, unemployment, and the absence of social support all increase risk. In India, alcohol pricing policies and prohibition laws in certain states are recognised public health levers.
- Neurobiological vulnerabilities: impaired prefrontal cortical control over limbic impulses — reduced in individuals with early-onset use, ADHD, and certain personality types — underpins behavioural dis-inhibition.
Diagnosis: ICD-11 Criteria and Screening Tools
Accurate diagnosis of a substance use disorder in clinical practice combines a structured history, validated screening instruments, and elements of the mental status examination. The goal of the diagnostic assessment is to answer four questions: What substance(s)? At what level of use (harmful use vs dependence)? Are withdrawal features present? Are there psychiatric or medical complications?
Structured substance history: Obtain the CAGE acronym items systematically — (C) Have you ever felt you should Cut down your drinking? (A) Have people ever Annoyed you by criticising your drinking? (G) Have you ever felt Guilty about your drinking? (E) Have you ever needed a drink first thing in the morning to steady your nerves or get rid of a hangover (Eye-opener)? Two or more positive responses constitute a positive CAGE screen for likely harmful use or dependence — sensitivity approximately 60–95%, specificity 40–95% depending on the population.
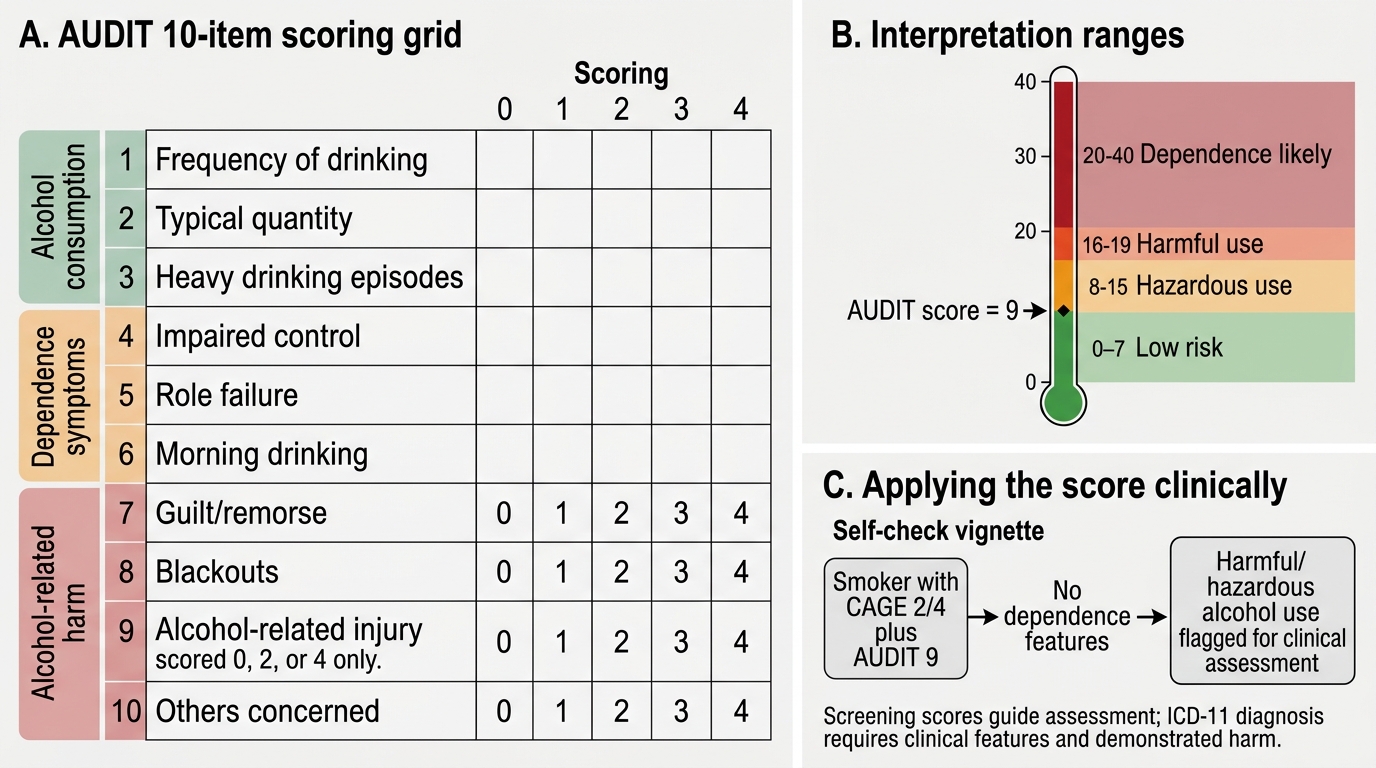
AUDIT (Alcohol Use Disorders Identification Test): The World Health Organization's validated 10-item questionnaire assesses quantity, frequency, frequency of heavy episodic drinking, and alcohol-related harm. Scores 0–7: low risk; 8–15: hazardous use; 16–19: harmful use; ≥20: probable dependence. AUDIT-C (first 3 items only) is a rapid 3-item screen suitable for busy primary care settings.
Mental Status Examination (MSE) features: Intoxicated patients show dysarthria, ataxic gait, nystagmus, behavioural disinhibition, emotional lability, and impaired attention/concentration. In delirium tremens, consciousness is clouded (delirium), perception is disturbed (hallucinations), and psychomotor agitation is marked. Patients in opioid intoxication show psychomotor retardation, miosis, and pin-point pupils. The MSE documents these findings systematically and guides the severity assessment.
ICD-11 diagnostic criteria application: Confirm at least the three dependence criteria (impaired control, increasing priority, physiological features) are present as an established pattern before diagnosing dependence — not as a momentary cluster but as a pattern over a meaningful period (the brief says 'established pattern'; ICD-11 does not specify a fixed duration for dependence, unlike DSM-5 which requires 12 months). Document which criteria are met.
Investigations: Liver function tests (elevated GGT is a sensitive marker of recent heavy drinking), complete blood count (macrocytosis from folate/B12 deficiency, thrombocytopenia), serum electrolytes (hyponatraemia, hypokalaemia in heavy drinkers), blood glucose, and urine drug screen for suspected polysubstance use.
AUDIT Scoring and Interpretation
SELF-CHECK
A smoker scores 2 out of 4 on the CAGE questionnaire. In the AUDIT, his score is 9. He has no features of dependence. Which ICD-11 category best describes his current status for alcohol?
A. Alcohol dependence — he meets two CAGE criteria
B. Alcohol harmful use — AUDIT 8–15 indicates hazardous/harmful use without dependence features
C. No alcohol use disorder — CAGE requires 3 of 4 for a positive screen
D. Alcohol dependence — any positive CAGE response is diagnostic
Reveal Answer
Answer: B. Alcohol harmful use — AUDIT 8–15 indicates hazardous/harmful use without dependence features
AUDIT 8–15 indicates hazardous or harmful use. The CAGE threshold for a positive screen is 2 or more positive responses, but a positive CAGE screen indicates probable harmful use or dependence — it is not automatically diagnostic of dependence. The vignette states 'no features of dependence' (no impaired control, increasing priority, or physiological features). ICD-11 harmful use requires demonstrated harm from the pattern of use. AUDIT score alone doesn't diagnose ICD-11 category but guides clinical assessment. In this vignette, without meeting the three dependence criteria, harmful use (or hazardous use flagged for intervention) is the appropriate label.