Page 3 of 9
PS3.1 | Psychoactive Substance Use Disorders — SDL Guide (Part 3)
Management: Alcohol Withdrawal and Wernicke Prevention
Safe management of alcohol withdrawal is a core clinical emergency skill for the Indian Medical Graduate, relevant in every setting from a primary health centre to a tertiary emergency department. The treatment strategy has two inseparable parallel goals: first, suppress the CNS hyperexcitability of withdrawal to prevent progression from minor symptoms through seizures to delirium tremens; and second, prevent Wernicke encephalopathy in thiamine-depleted patients by replacing thiamine before any intravenous glucose is administered. These goals are not sequential — they must be addressed together, simultaneously, and in the correct order. Failure on either front carries a distinct mortality risk: untreated delirium tremens kills through hyperthermia and cardiovascular collapse, while missed Wernicke encephalopathy kills neurons permanently and leaves the patient with Korsakoff syndrome.
Benzodiazepines — the cornerstone of withdrawal management: Benzodiazepines act on GABA-A receptors, directly compensating for alcohol's absence and suppressing the hyperexcitable state. In India, chlordiazepoxide is the preferred agent (long half-life provides a 'self-tapering' effect via active metabolites; less respiratory depression than diazepam; available and inexpensive). Diazepam is the alternative, especially parenterally in severe withdrawal. The dose is titrated against CIWA-Ar severity:
- Mild withdrawal (CIWA <10): oral chlordiazepoxide 25–50 mg every 6 hours with PRN doses.
- Moderate (CIWA 10–18): chlordiazepoxide 50 mg every 6 hours; closely monitored.
- Severe (CIWA >18) or delirium tremens: IV diazepam or lorazepam, intensive care monitoring.
A symptom-triggered protocol (dose given when CIWA-Ar ≥8, rather than on a fixed schedule) has been shown to use less total benzodiazepine and shorten treatment duration without loss of efficacy.
Thiamine (Vitamin B1) — MUST precede glucose: Chronic alcohol use causes thiamine deficiency due to poor dietary intake, impaired absorption, and reduced hepatic storage. Thiamine is an essential cofactor for glucose metabolism (pyruvate dehydrogenase complex). When thiamine-depleted patients receive intravenous glucose without prior thiamine replacement, the sudden glucose load may precipitate Wernicke encephalopathy — an acute neuropsychiatric emergency characterised by the triad of confusion, ophthalmoplegia (cranial nerve VI palsy is earliest — lateral gaze palsy), and ataxia. ALWAYS give thiamine 100 mg IV (or IM) BEFORE or SIMULTANEOUSLY with intravenous dextrose — never after. Thiamine (Pabrinex in UK; thiamine injection available in Indian hospitals) should be given prophylactically to all patients presenting with alcohol dependence. Untreated Wernicke encephalopathy progresses to Korsakoff syndrome (permanent anterograde amnesia with confabulation) in up to 85% of cases.
Fluid, electrolyte and nutritional correction: Dehydration, hyponatraemia, hypomagnesaemia, and hypokalaemia are common and must be corrected. Magnesium supplementation reduces seizure risk.
Monitoring: Vital signs (BP, PR, temperature), CIWA-Ar score, GCS, seizure occurrence. Respiratory rate must be monitored when high-dose benzodiazepines are used.
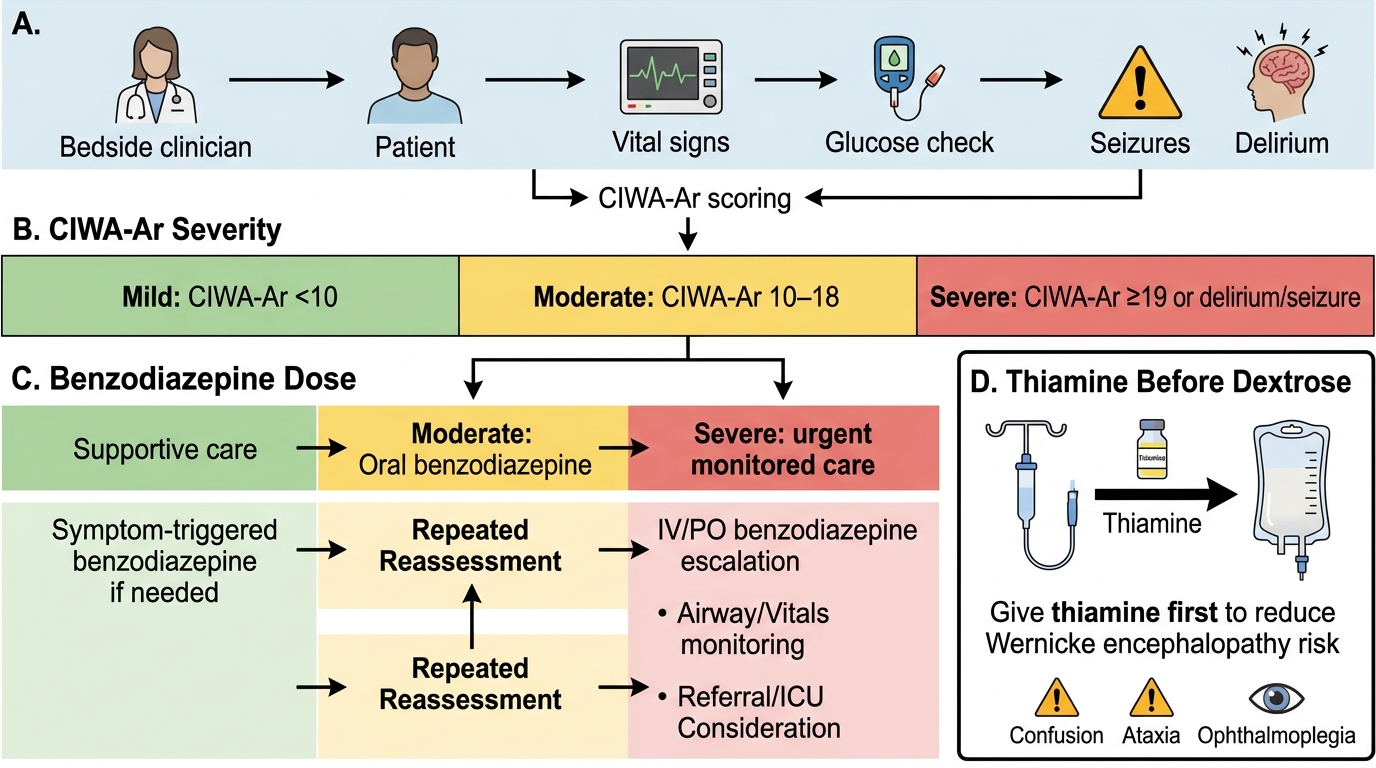
Alcohol Withdrawal Management Flow
Management: Tobacco Cessation
Tobacco use — both smoked and smokeless — is the single largest preventable cause of premature death in India, responsible for cancers (oral, lung, oesophageal, bladder), ischaemic heart disease, and chronic obstructive pulmonary disease. With over 260 million users and more than 1 million deaths annually attributable to tobacco, India's clinicians carry a unique population-level responsibility: every clinical encounter with a tobacco user is a potential intervention that, across millions of consultations per year, translates into measurable reductions in national disease burden. This is why the NMC emphasises tobacco cessation as a core primary-care skill, not merely a secondary referral. Even a brief conversation of 3–5 minutes — delivered without specialist training or resources — increases the annual quit rate at the population level. The evidence-based framework that makes this practical in any setting is the 5 A's:
Provided image
- Ask every patient about tobacco use at every visit — normalise the enquiry.
- Advise all tobacco users to quit — brief, clear, personalised advice ('Your gutka use is directly increasing your risk of oral cancer').
- Assess willingness to quit — stage of change informs the response.
- Assist those willing to quit with behavioural counselling and pharmacotherapy.
- Arrange follow-up within 1–2 weeks and at subsequent visits.
Brief advice alone (3–5 minutes) increases quit rates by 1–3% above controls — a small but population-significant effect.
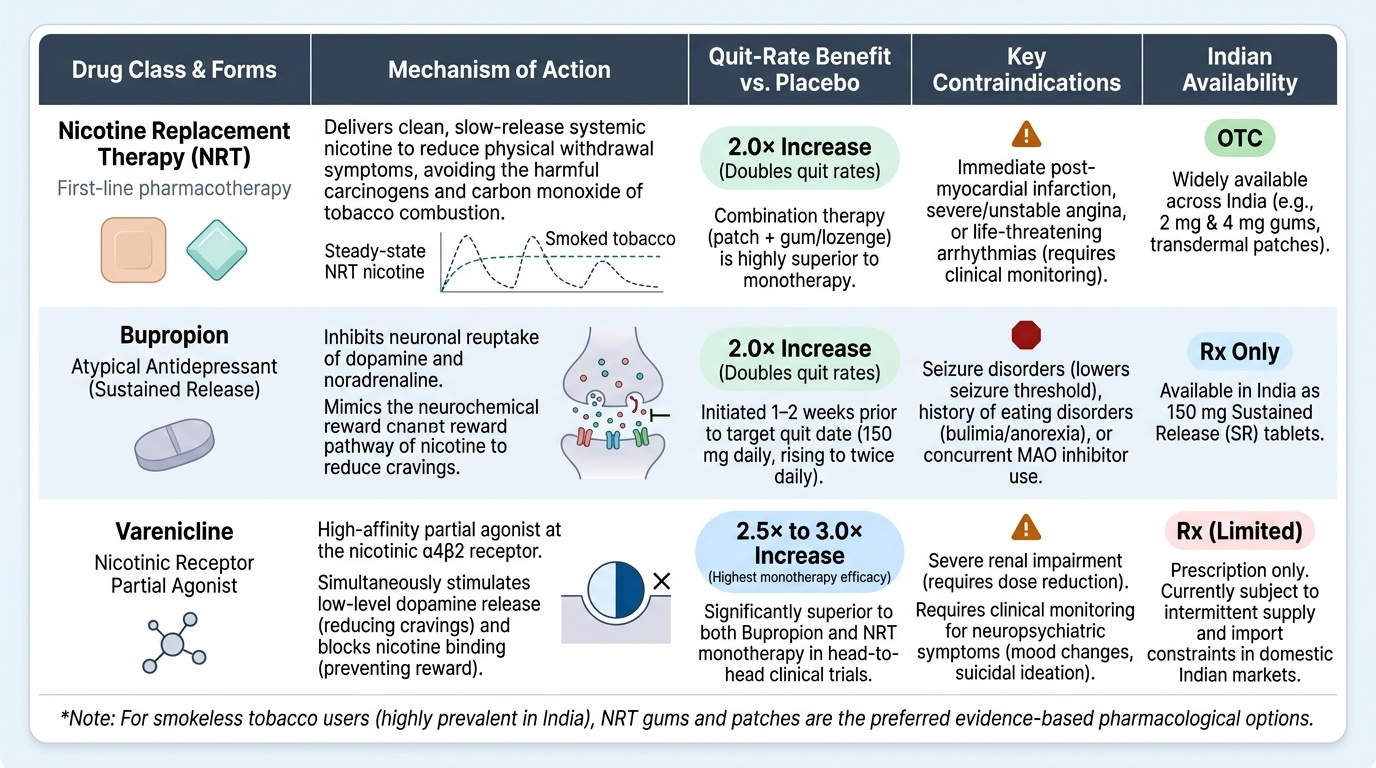
Nicotine Replacement Therapy (NRT): Nicotine patches, gum, lozenges, and inhalers deliver nicotine without the carcinogens and carbon monoxide of combustion. NRT doubles quit rates compared to placebo. Combining long-acting (patch) with short-acting (gum, lozenge) NRT is more effective than monotherapy. For smokeless tobacco users, NRT gum and patch are the recommended pharmacological options; data on smokeless tobacco cessation are less robust than for smoked tobacco.
Bupropion: An atypical antidepressant that reduces nicotine craving and withdrawal by inhibiting reuptake of dopamine and noradrenaline. Doubles quit rates. Contraindicated in patients with a history of seizures, eating disorders, or on MAO inhibitors. Start 1–2 weeks before the quit date at 150 mg daily for 3 days, then 150 mg twice daily.
Varenicline: A partial agonist at nicotinic α4β2 receptors. It both reduces craving (agonist action) and reduces the reward of smoking if the patient does smoke (competitive antagonism). The most effective single pharmacotherapy — approximately triples quit rates. Requires monitoring for mood changes (black-box warning lifted in most guidelines after post-marketing studies, but monitor in patients with psychiatric history). Varenicline is the first-line pharmacotherapy for motivated quitters in India where accessible.
For smokeless tobacco, the same cessation counselling principles apply; emphasise the oral cancer risk (visual aids of oral lesions are highly effective in motivating smokeless tobacco users).
Management: Opioid Use Disorder
Opioid use disorder presents with the classic triad of intoxication (miosis, respiratory depression, CNS depression), a well-defined withdrawal syndrome, and the pervasive medical and social consequences of chronic use. In India, opioid dependence — particularly heroin and pharmaceutical opioid misuse — is concentrated in certain states but is encountered nationally, and an understanding of its management is essential regardless of specialty. The Indian Medical Graduate must be able to recognise the intoxication emergency, manage the withdrawal syndrome humanely and safely, and either initiate or facilitate access to evidence-based long-term maintenance treatment. These are not psychiatry-only competencies: opioid emergencies arrive in emergency departments, general wards, and rural health centres. Management has two distinct but related phases: managing acute withdrawal and initiating long-term maintenance treatment.
Provided image
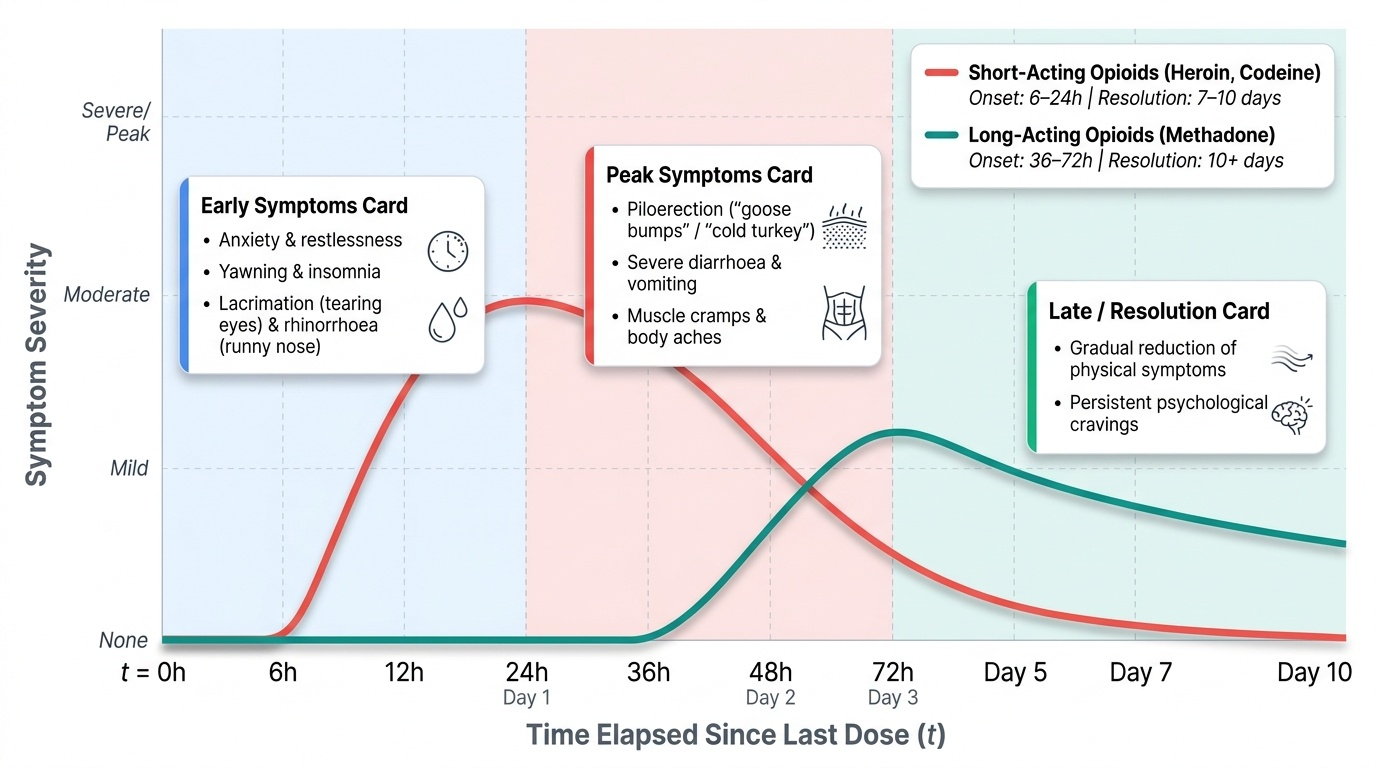
Opioid withdrawal begins 6–24 hours after the last dose of short-acting opioids (heroin, codeine) and 36–72 hours for long-acting opioids (methadone). Although intensely uncomfortable — producing anxiety, restlessness, yawning, lacrimation, rhinorrhoea, piloerection ('goose bumps', hence 'cold turkey'), muscle cramps, severe diarrhoea, vomiting, and insomnia — opioid withdrawal is not typically life-threatening in otherwise healthy adults (contrast with alcohol withdrawal). However, it is a major driver of relapse and requires humane management.
Withdrawal management options:
- Symptomatic (non-opioid) management: Clonidine (alpha-2 agonist) reduces autonomic symptoms (tachycardia, sweating, hypertension). Loperamide for diarrhoea. Analgesics for myalgia. Does not address craving.
- Opioid substitution (agonist) therapy for detoxification: Short-acting opioid substituted and tapered over 1–4 weeks. Rarely used for primary detoxification in India due to regulatory constraints.
Long-term Opioid Agonist Therapy (OAT/Maintenance Treatment): This is the evidence-based standard of care for opioid dependence. By providing a stable, supervised opioid agonist dose, OAT eliminates withdrawal symptoms and craving, prevents needle sharing (and HIV/HCV transmission), and allows social functioning. Two agents are available:
- Buprenorphine (Subutex/Buprenorphine SL): A partial agonist at mu-opioid receptors with ceiling effect on respiratory depression (safer in overdose). Available in India under the National Drug Dependence Treatment Centre (NDDTC/NDDTCP) opioid substitution programme. Often formulated with naloxone (buprenorphine-naloxone, to deter injection).
- Methadone: A long-acting full mu-opioid agonist; highly effective for maintenance; QTc prolongation is a concern at higher doses; available in India but less accessible than buprenorphine in most states.
Both agents require prescription under narcotic drug regulations (NDPS Act 1985, with amended rules permitting OAT). Referral to a government-recognised opioid substitution treatment centre is appropriate for most patients. Psychosocial interventions — motivational enhancement, relapse prevention counselling, family therapy, and self-help groups — are essential complements to pharmacotherapy.
SELF-CHECK
You are about to give IV dextrose to a malnourished patient with alcohol dependence who has presented in a confused state. What must you do FIRST and why?
A. Give IV diazepam first to prevent seizures before glucose
B. Give IV thiamine BEFORE or WITH the dextrose — glucose without thiamine may precipitate Wernicke encephalopathy
C. Perform blood sugar first; give dextrose only if hypoglycaemic
D. Administer naloxone first to exclude opioid co-ingestion
Reveal Answer
Answer: B. Give IV thiamine BEFORE or WITH the dextrose — glucose without thiamine may precipitate Wernicke encephalopathy
Thiamine MUST be given before or simultaneously with intravenous glucose in any malnourished or alcohol-dependent patient. Chronic alcohol use depletes thiamine (Vitamin B1), which is a critical cofactor for glucose metabolism (pyruvate dehydrogenase). Giving dextrose to a thiamine-depleted patient without first correcting thiamine can precipitate Wernicke encephalopathy — an acute neurological emergency causing confusion, ophthalmoplegia, and ataxia that may become permanent (Korsakoff syndrome). Checking blood glucose before treating is sensible, but the thiamine-before-glucose rule applies regardless. IV diazepam addresses withdrawal seizures, not the thiamine-Wernicke pathway. Naloxone would be relevant if opioid toxidrome (miosis, respiratory depression) were present.
CLINICAL PEARL
Thiamine before glucose — a life-saving sequence. Wernicke encephalopathy is preventable. Give thiamine 100 mg IV (or IM) BEFORE or SIMULTANEOUSLY with any intravenous dextrose in patients who are malnourished, alcohol-dependent, or at risk. The sequence matters: glucose without thiamine in a thiamine-depleted brain triggers a catastrophic metabolic crisis in glucose-dependent neurons (especially the mammillary bodies and dorsomedial thalamus). Missing this sequence transforms a treatable emergency into permanent Korsakoff amnesia. Similarly, in alcohol withdrawal, do NOT wait for delirium tremens to develop before starting benzodiazepines — the CIWA-Ar should be scored early and treatment initiated at moderate severity. Early treatment reduces total benzodiazepine requirement and prevents escalation.
Self-Assessment: Integration and Reflection
The management of substance use disorders in India demands integrated clinical reasoning: you must identify the substance, classify the disorder, manage the acute medical emergency (if present), and initiate a longer-term management plan aligned with patient readiness and available resources. This section tests your integration across all four arc steps of this SDL.
Begin by asking yourself: can you walk a patient with alcohol dependence through the withdrawal timeline, explaining why their tremors started 8 hours after their last drink, why you are worried about seizures at 24 hours, and why you are most vigilant between 48 and 72 hours? Can you justify prescribing thiamine before dextrose at the bedside — not as a rule to memorise, but as a physiological necessity arising from thiamine's role in the pyruvate dehydrogenase complex? Can you distinguish ICD-11 harmful use from dependence in a patient who drinks heavily three times a week but does not drink daily — and avoid over-diagnosing dependence simply because of quantity?
For tobacco cessation, ask: can you deliver a 3-minute brief advice session using the 5 A's framework to a patient with a 20-pack-year history of bidi smoking? Can you explain to the patient why varenicline reduces both craving and the reward of smoking, and what mood-related side effects to watch for? For a gutka user, can you adapt your counselling to emphasise the oral cancer risk — the most salient motivator in the Indian context?
For opioid use disorder, can you explain to a patient's family why buprenorphine maintenance is evidence-based treatment and not 'replacing one addiction with another' — the most common myth encountered in Indian clinical practice? Can you describe what opioid withdrawal looks and feels like, and reassure them it is not life-threatening while taking it seriously as a driver of relapse?
Finally, revisit the opening hook: the 45-year-old farm labourer who seized at 30 hours. Your immediate priorities are benzodiazepines (IV lorazepam or diazepam for the acute seizure if ongoing), thiamine 100 mg IV before further dextrose, CIWA-Ar scoring, electrolyte correction, monitoring for delirium tremens over the next 48 hours, and, once medically stable, a conversation about alcohol dependence treatment and relapse prevention. This is the breadth of the practising Indian clinician's skill set for substance use disorders.