Page 4 of 11
PS11.1 | Intellectual Disability Disorder — SDL Guide
Learning Objectives
- Describe the definition and diagnostic criteria of Intellectual Disability Disorder per ICD-11 and DSM-5
- Identify the aetiological categories of intellectual disability including genetic, prenatal, perinatal, and postnatal causes
- Outline the principles of developmental assessment including intellectual and adaptive functioning evaluation
- Apply the DSM-5 severity classification framework based on adaptive functioning domains
- Describe the multidisciplinary management and prevention strategies for intellectual disability
INSTRUCTIONS
Intellectual Disability Disorder (IDD) is a leading cause of lifelong disability worldwide, with a global prevalence of approximately 1–3%. It represents a heterogeneous group of conditions sharing a final common pathway of impaired intellectual and adaptive functioning arising during the developmental period. Recognising IDD early, establishing its aetiology, and coordinating multidisciplinary care can substantially improve functional outcomes for affected children and reduce the impact on families.
References
- Ahuja N. A Short Textbook of Psychiatry, 8th ed. Jaypee Brothers, New Delhi. Chapter 16: Child and Adolescent Psychiatry — Intellectual Disability (textbook)
- Kaplan HI, Sadock BJ. Synopsis of Psychiatry, 11th ed. Wolters Kluwer. Chapter 31: Intellectual Disability (textbook)
- ICD-11 Classification of Mental and Behavioural Disorders. WHO, Geneva, 2022. Section 06: Neurodevelopmental Disorders — Disorders of Intellectual Development (6A00-6A03) (guideline)
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (DSM-5). APA, 2013. Intellectual Disability (Intellectual Developmental Disorder) (guideline)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 4-year-old boy is brought to the developmental paediatrics clinic by his parents, who are worried that he is not speaking in sentences, cannot button his shirt, and struggles to follow simple two-step instructions. They had assumed he was 'a late developer', but his nursery teacher recently expressed concern that his development is significantly behind his peers. On assessment, his IQ is estimated at 52 on a standardised test, and his adaptive behaviour on the Vineland Adaptive Behavior Scales is well below age norms across communication, daily living skills, and socialisation domains. His older sister has similar features, and the family has a history of miscarriages. Chromosomal microarray identifies a Fragile X syndrome mutation. This child has Intellectual Disability Disorder — and understanding this condition means understanding not just a diagnostic label, but a lifelong trajectory that can be profoundly shaped by early identification, multidisciplinary support, and preventive strategies.
WHY THIS MATTERS
Intellectual Disability Disorder affects an estimated 1–3% of the global population, making it among the most common serious neurodevelopmental conditions seen in clinical practice. In India, the Persons with Disabilities Act and the Rights of Persons with Disabilities Act (2016) legally recognise intellectual disability and mandate educational inclusion, rehabilitation, and social support — meaning that clinicians must understand not only the medical dimensions of IDD but also its legal and social frameworks. Importantly, intellectual disability is a common differential diagnosis encountered in paediatrics, general medicine, psychiatry, and even obstetrics (antenatal prevention is a key management dimension). The Indian burden is amplified by preventable causes including iodine deficiency, congenital infections, and perinatal hypoxia — all of which are addressable at the primary care level.
RECALL
Before proceeding, recall what you know from Year 1 Physiology about normal cognitive development and from Biochemistry about metabolic disorders that can affect the brain in early life. Intellectual functioning is measured by standardised IQ tests, which are normed so that the population mean is 100 and the standard deviation is 15. This means that an IQ of 70 corresponds to 2 standard deviations below the mean — the conventional threshold below which intellectual functioning is considered significantly impaired. You should also recall from Biochemistry that Phenylketonuria (PKU) results from a deficiency of phenylalanine hydroxylase, leading to accumulation of phenylalanine which is neurotoxic — and that early detection by neonatal screening followed by a low-phenylalanine diet can prevent intellectual disability entirely.
Clinical Presentation and Developmental Features of Intellectual Disability
Intellectual Disability Disorder (IDD) — also termed Disorders of intellectual development in ICD-11 — is a neurodevelopmental condition characterised by significant limitations in intellectual functioning and adaptive behaviour, with onset during the developmental period (childhood and adolescence). The clinical presentation varies considerably with the severity of disability and the presence of associated conditions.
In mild intellectual disability, which accounts for approximately 85% of all cases, the child often presents to clinical attention only at school age when academic demands exceed capacity. Prior to school, development may appear only mildly delayed. The child can develop social and communication skills, may read and write at a basic level, and as an adult can typically achieve semi-independent living with appropriate support. Mild IDD is often identified through school referral for poor academic performance rather than through early developmental surveillance.
In moderate intellectual disability (approximately 10% of cases), delays in language, motor, and self-care milestones are evident by early childhood. These children can learn to communicate — verbally or via AAC — and can manage some self-care tasks with supervision. They typically require supported living arrangements as adults and benefit substantially from structured special education.
In severe intellectual disability (approximately 3–4%), significant developmental delays are evident in infancy, and these children have very limited expressive language and substantial self-care needs throughout life. In profound intellectual disability (approximately 1–2%), there is extensive impairment in all domains including sensorimotor function; most individuals require intensive support for all activities of daily living. Severe and profound IDD are more likely to be associated with an identifiable neurological or genetic cause.
Across all severity levels, the clinical picture includes delays in reaching developmental milestones (motor, language, adaptive), below-average academic performance, difficulty with abstract thinking and problem-solving, and limitations in adaptive behaviour — the set of learned conceptual, social, and practical skills needed to function in daily life. Co-morbid conditions are common and clinically important: epilepsy occurs in approximately 25–30% of people with IDD (rising sharply with severity), ASD co-occurs in approximately 30%, and co-morbid psychiatric conditions (anxiety, depression, ADHD, sleep disorders) are significantly more prevalent than in the general population.
The clinical distinction between IDD and other neurodevelopmental conditions is critical: unlike ASD (where social communication deficits are the primary feature and IQ may be average or high), IDD involves a global deficit in intellectual and adaptive functioning. Unlike specific learning disorders (where deficits are circumscribed to reading, writing, or mathematics), IDD affects all domains of intellectual functioning.
SELF-CHECK
A 6-year-old girl has below-average academic performance, can speak in short sentences, and needs help with dressing but can eat independently. Psychometric testing shows a full-scale IQ of 58. Her Vineland Adaptive Behavior Scales score is below the 2nd percentile for communication and daily living skills. Which of the following best describes the classification of her condition?
A. Specific learning disorder in reading
B. Mild intellectual disability
C. Moderate intellectual disability
D. Borderline intellectual functioning
Reveal Answer
Answer: B. Mild intellectual disability
An IQ of 58 falls in the historical 'mild' IDD range (approximately 50-69). She communicates in short sentences, manages some self-care, and requires support — all consistent with mild IDD. Specific learning disorder would show circumscribed deficits (e.g., only reading) without global cognitive impairment. Borderline intellectual functioning refers to IQ 71-84, which does not meet the IDD threshold. Moderate IDD (historical IQ 35-49) would typically show more significant language delays and greater self-care dependence. Note: under DSM-5, severity is graded by adaptive functioning — her Vineland scores confirm significant adaptive deficits consistent with mild IDD.
Aetiology — Genetic, Prenatal, Perinatal, and Postnatal Causes
The aetiology of Intellectual Disability Disorder is heterogeneous — multiple causes operate across a spectrum from conception to early childhood. Systematic aetiological classification into four categories (genetic, prenatal, perinatal, postnatal) provides a clinically useful framework for investigation, family counselling, and prevention planning.
Genetic and chromosomal causes account for the largest single group identified in moderate-to-severe IDD. Down syndrome (Trisomy 21) is the most common chromosomal cause, occurring in approximately 1 in 700–1,000 live births; the extra chromosome 21 disrupts brain development and is associated with intellectual disability (most commonly in the mild-to-moderate range), distinctive facial features, congenital heart disease, and early-onset Alzheimer disease. Fragile X syndrome is the most common inherited (single-gene) cause of intellectual disability, caused by a CGG trinucleotide repeat expansion in the FMR1 gene on the X chromosome; it predominantly affects males (females are often carriers with milder features) and is associated with IDD, macroorchidism, large ears, hyperactivity, and ASD features. Other significant genetic causes include Phenylketonuria (PKU — phenylalanine hydroxylase deficiency; autosomal recessive; preventable with early dietary intervention), chromosomal deletions and duplications detected by microarray (e.g., 22q11.2 deletion syndrome), and rare monogenic disorders.
Prenatal non-genetic causes include congenital infections — particularly the TORCH group: Toxoplasma gondii, Rubella virus, Cytomegalovirus (CMV), Herpes simplex, and others including Treponema pallidum (syphilis) and Zika virus. These pathogens cross the placenta during critical periods of brain development, causing microcephaly, cerebral calcifications, and intellectual disability. Iodine deficiency during pregnancy leads to hypothyroidism in the foetus (cretinism) — characterised by intellectual disability, growth retardation, and deafness — and remains a preventable cause in iodine-deficient regions. Prenatal alcohol exposure (Foetal Alcohol Spectrum Disorder) causes structural brain damage and is one of the leading preventable causes of IDD globally. Teratogenic drugs — including valproate taken during pregnancy for epilepsy — carry a significant risk of neurodevelopmental effects including IDD and ASD in the exposed child.
Perinatal causes include birth asphyxia (hypoxic-ischaemic encephalopathy — HIE) due to obstetric complications causing brain hypoxia around the time of delivery, prematurity with associated complications (intraventricular haemorrhage, periventricular leukomalacia), and neonatal hyperbilirubinaemia (kernicterus from severe jaundice damaging the basal ganglia and brainstem).
Postnatal causes include central nervous system infections (bacterial meningitis, tuberculous meningitis, viral encephalitis) causing brain damage in infancy and early childhood, traumatic brain injury, lead poisoning (chronic low-level exposure in children impairs cognitive development), and severe nutritional deficiencies (iron, iodine) in early childhood.
In clinical practice, a specific aetiology is identified in approximately 50–70% of severe IDD cases and in a lower proportion of mild IDD cases (where polygenic factors and social-environmental influences often predominate). The aetiological work-up typically includes chromosomal microarray, metabolic screening, neuroimaging, TORCH serology, and thyroid function.
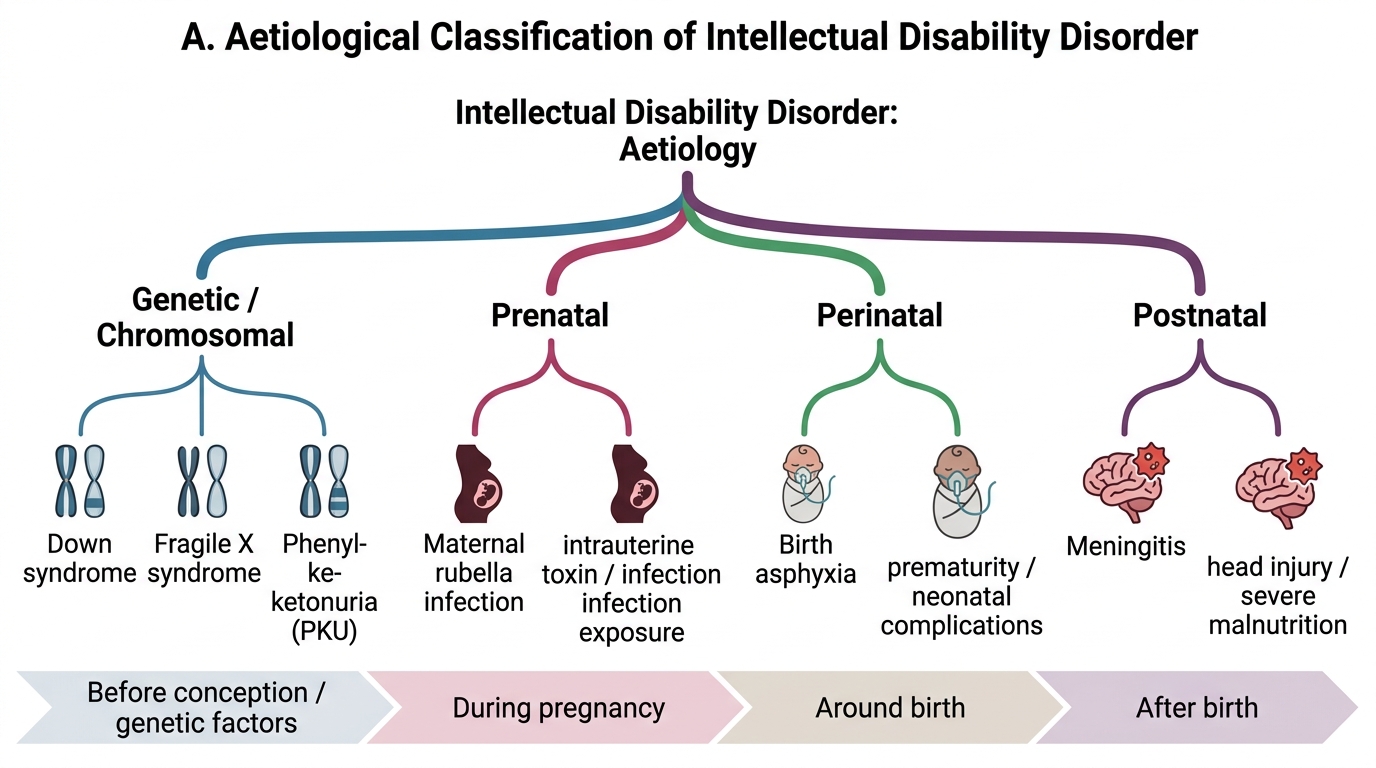
Aetiological Classification of Intellectual Disability Disorder
Diagnosis and Developmental Assessment
Diagnosis of Intellectual Disability Disorder requires the co-presence of three criteria, consistently across both ICD-11 and DSM-5: (1) significant deficits in intellectual functioning, (2) significant deficits in adaptive functioning, and (3) onset during the developmental period. All three must be present — no single criterion alone establishes the diagnosis.
Provided image
Criterion 1: Intellectual functioning deficits. Intellectual functioning is measured by standardised, individually administered intelligence tests. A full-scale IQ approximately 2 or more standard deviations below the population mean — corresponding to approximately IQ ≤70 (with a standard error of measurement of approximately ±5 points) — is considered a significant deficit. Commonly used instruments include the Wechsler Intelligence Scale for Children (WISC), the Stanford-Binet Intelligence Scale, and the Malin's Intelligence Scale for Indian Children (MISIC — normed on the Indian population).
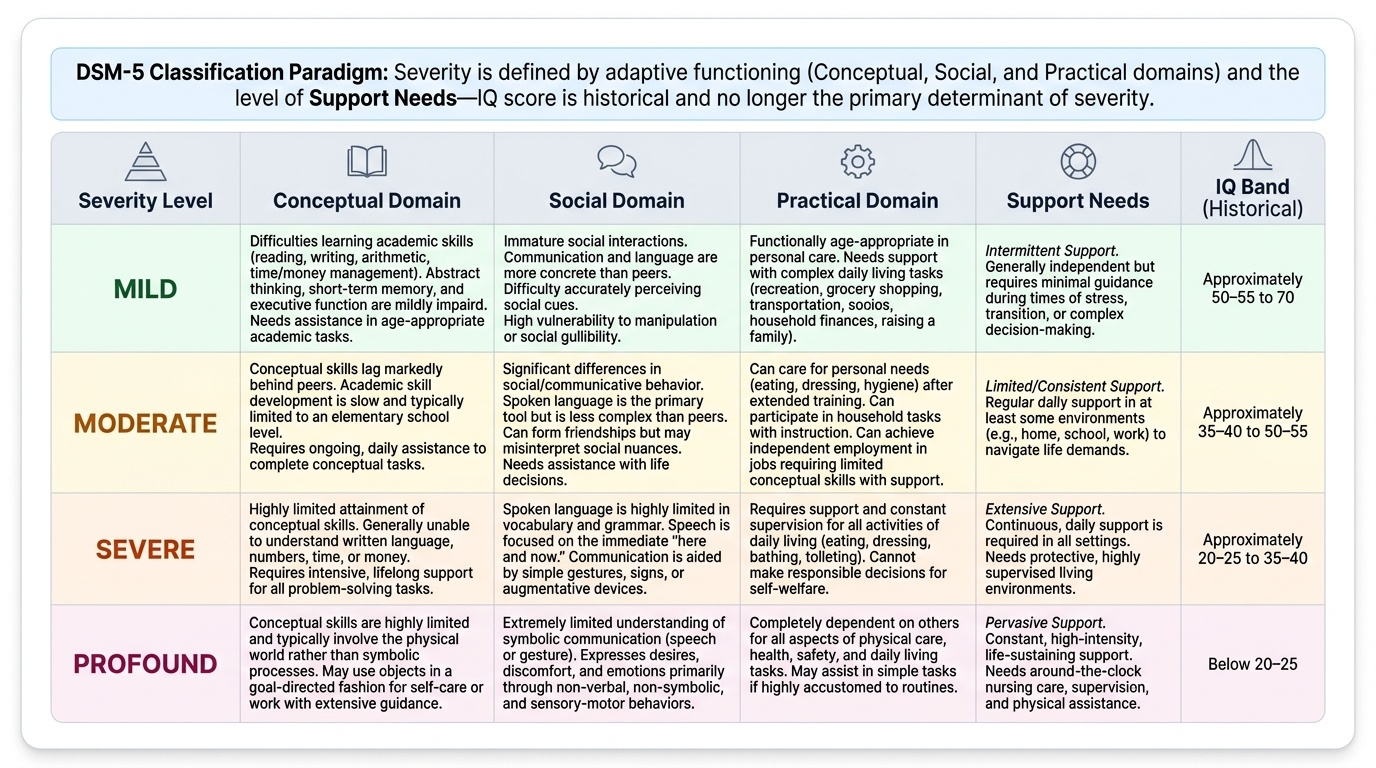
Criterion 2: Adaptive behaviour deficits. Adaptive behaviour encompasses the set of conceptual, social, and practical skills that people learn and apply in everyday life. The Vineland Adaptive Behavior Scales is the most widely used standardised tool, assessing communication, daily living skills, socialisation, and motor skills through structured caregiver interview. DSM-5 places the primary severity classification on adaptive functioning, not IQ. This is a critical distinction: severity is graded by how much support the person needs to function in the three adaptive domains (conceptual, social, practical) — an IQ score alone does not determine management or prognosis.
Severity classification (DSM-5, adaptive function-based):
| Severity | Conceptual domain | Social domain | Practical domain | Historical IQ (approx.) |
|---|---|---|---|---|
| Mild | Difficulties with reading, writing, money management | Immature social interaction, gullible; friendships possible | Some self-care, may need support with finances, transport | 50–69 |
| Moderate | Below grade-level academic skills; needs support with written tasks | Notable differences in social behaviour; limited social judgement | Some ADL independence with training; needs supervision in novel settings | 35–49 |
| Severe | Limited understanding of written language and number concepts | Very limited symbolic communication | Requires support for all ADLs; cannot make responsible decisions | 20–34 |
| Profound | Symbolic processes very limited; physical rather than symbolic communication | Understanding very limited; emotional relationships with familiar carers | Dependent for all aspects of physical care | <20 |
IMPORTANT: The IQ bands in the table are historical approximations only — DSM-5 explicitly states that severity is graded by adaptive functioning, not IQ. Clinical management and support planning are based on adaptive function, not an IQ number.
Criterion 3: Developmental period onset. This criterion distinguishes IDD from dementia (acquired cognitive decline in adulthood after a period of normal development). The developmental period conventionally extends through childhood and adolescence (approximately age 0–18 years). Onset during this period is a DSM-5 and ICD-11 requirement.
Developmental history is the cornerstone of assessment, complementing psychometric testing. Key elements include: birth history (gestation, mode of delivery, birth asphyxia, neonatal course), developmental milestone timeline (when did the child sit, walk, say first words?), family history (consanguinity, similar conditions in relatives, miscarriage history — the Fragile X case in the hook), and educational history (performance and teacher concerns). Maternal history during pregnancy — infections, drug exposures, iodine status, alcohol use — is essential for aetiological investigation.
Differential diagnosis:
| Condition | Key distinguishing feature |
|---|---|
| Autism Spectrum Disorder | Social communication + RRBs are the core features; IQ may be average or high; ASD may co-occur with IDD |
| Specific learning disorder | Circumscribed deficit (reading only, or maths only); overall IQ above IDD threshold |
| Acquired dementia | Cognitive decline AFTER a period of normal adult development — not a neurodevelopmental onset |
| Deafness / visual impairment | Apparent developmental delay may reflect sensory limitation; audiometric and ophthalmic assessment essential |
| Chronic psychosocial deprivation | Severe early deprivation may impair cognitive development; may be reversible with enriched environment |
SELF-CHECK
A 12-year-old boy with an IQ of 42 on standardised testing requires assistance with all activities of daily living (dressing, bathing, eating with adaptive utensils) and communicates through single words and gesture. He attends a special school. According to DSM-5, which criterion is the PRIMARY basis for grading his severity level?
A. His full-scale IQ score of 42
B. His performance on academic tests in school
C. Deficits in adaptive functioning across conceptual, social, and practical domains
D. Age of first developmental concern as reported by parents
Reveal Answer
Answer: C. Deficits in adaptive functioning across conceptual, social, and practical domains
DSM-5 explicitly classifies severity of Intellectual Disability Disorder based on adaptive functioning across conceptual, social, and practical domains — NOT IQ score. IQ score is relevant for establishing the intellectual functioning criterion (significant deficit below ~70) but does not determine severity level. This shift from the historical IQ-band system (used in earlier DSM and ICD versions) reflects recognition that adaptive function predicts real-world support needs, quality of life, and functional outcomes far better than IQ alone. This child's profile (ADL dependence, single-word communication, special school placement) is consistent with severe IDD based on adaptive function.