Page 5 of 11
PS11.1 | Intellectual Disability Disorder — SDL Guide (Part 2)
Management — Multidisciplinary and Preventive Approaches
The management of Intellectual Disability Disorder is fundamentally multidisciplinary and lifelong. There is no pharmacological treatment that reverses the intellectual disability itself — management is directed at maximising functional capacity, managing co-morbidities, supporting the family, and addressing preventable causes at the population level. Effective management requires coordinated input from physicians, psychologists, speech-language pathologists, occupational therapists, physiotherapists, special educators, social workers, and the family itself — no single clinician can provide this comprehensively alone.
Early identification and intervention is the single most powerful determinant of long-term outcomes. Early intensive developmental intervention programmes — starting as early as infancy — can substantially improve language, adaptive skills, and social functioning even in children with significant ID. The 0–5 year window is critical for brain plasticity; waiting for a definitive diagnosis before starting intervention is counterproductive. Key intervention components include:
- Special and inclusive education: Structured special education programmes tailored to the child's cognitive level provide academic skills, socialisation, and pre-vocational training. The Rights of Persons with Disabilities Act (2016) in India mandates inclusive education for children with intellectual disability where feasible, with appropriate support and accommodations.
- Speech and language therapy: Targets communication deficits — ranging from articulation in mild IDD to building an AAC system in severe or profound IDD. Early SLT referral is essential for any child with language delay.
- Occupational therapy (OT): Addresses self-care skills, fine motor development, and sensory integration. OT-designed activities of daily living training can significantly increase independence in mild and moderate IDD.
- Physiotherapy: Important for children with associated motor impairments, hypotonia (commonly seen in Down syndrome and many genetic causes), and for children with severe/profound IDD who may also have cerebral palsy.
- Behaviour management: Functional behaviour assessment identifies the function of challenging behaviours (communication of need, avoidance, sensory-seeking) and guides positive behaviour support strategies. Physical restraint is not a therapeutic approach.
- Family psychoeducation and support: Parents require structured counselling about the diagnosis, prognosis, realistic expectations, legal rights, and available services. Caregiver burden is high and mental health support for family members is an important but often neglected component.
Pharmacotherapy in IDD does not treat the intellectual disability itself. Drugs are used to manage co-morbid conditions: antiepileptic drugs for seizures (noting that some AEDs have cognitive side effects to be balanced against seizure control); risperidone or aripiprazole for challenging behaviours and irritability; melatonin for sleep disturbance; and SSRIs or anxiolytics for co-occurring anxiety or mood disorders. Hypothyroidism as a cause (e.g., cretinism, Down syndrome-associated hypothyroidism) is treated with levothyroxine — this is one of the few pharmacological interventions that can directly improve cognitive development when the cause is hormonal.
Genetic counselling is offered to families of children with chromosomal or monogenic causes of IDD. Recurrence risks vary by cause: Down syndrome (non-disjunction) recurrence risk increases with maternal age; Fragile X (X-linked inheritance) has specific carrier-status and penetrance considerations; autosomal recessive conditions (PKU) carry a 25% recurrence risk in future pregnancies.
Prevention is a critical dimension of IDD management at the population and individual level:
- Antenatal: Universal iodine supplementation in pregnancy; periconceptional folic acid to prevent neural tube defects; congenital rubella prevention through MMR vaccination; avoidance of teratogenic drugs (valproate in women of childbearing age — mandatory counselling and the MHRA/NMC valproate risk acknowledgement); avoidance of alcohol in pregnancy; management of maternal hypothyroidism; antenatal screening for chromosomal abnormalities (cell-free fetal DNA, amniocentesis/chorionic villus sampling for high-risk pregnancies).
- Perinatal: Skilled birth attendant availability to prevent birth asphyxia; appropriate management of neonatal jaundice (phototherapy, exchange transfusion for severe hyperbilirubinaemia); neonatal intensive care for premature infants.
- Neonatal screening: Universal newborn screening for PKU (Guthrie test, dried blood spot), congenital hypothyroidism, and other treatable metabolic conditions allows initiation of specific dietary or hormonal therapy before intellectual damage occurs.
- Postnatal: Prevention of CNS infections through immunisation (Hib, pneumococcal, meningococcal vaccines); lead poisoning prevention through environmental measures; nutritional supplementation in at-risk infants.
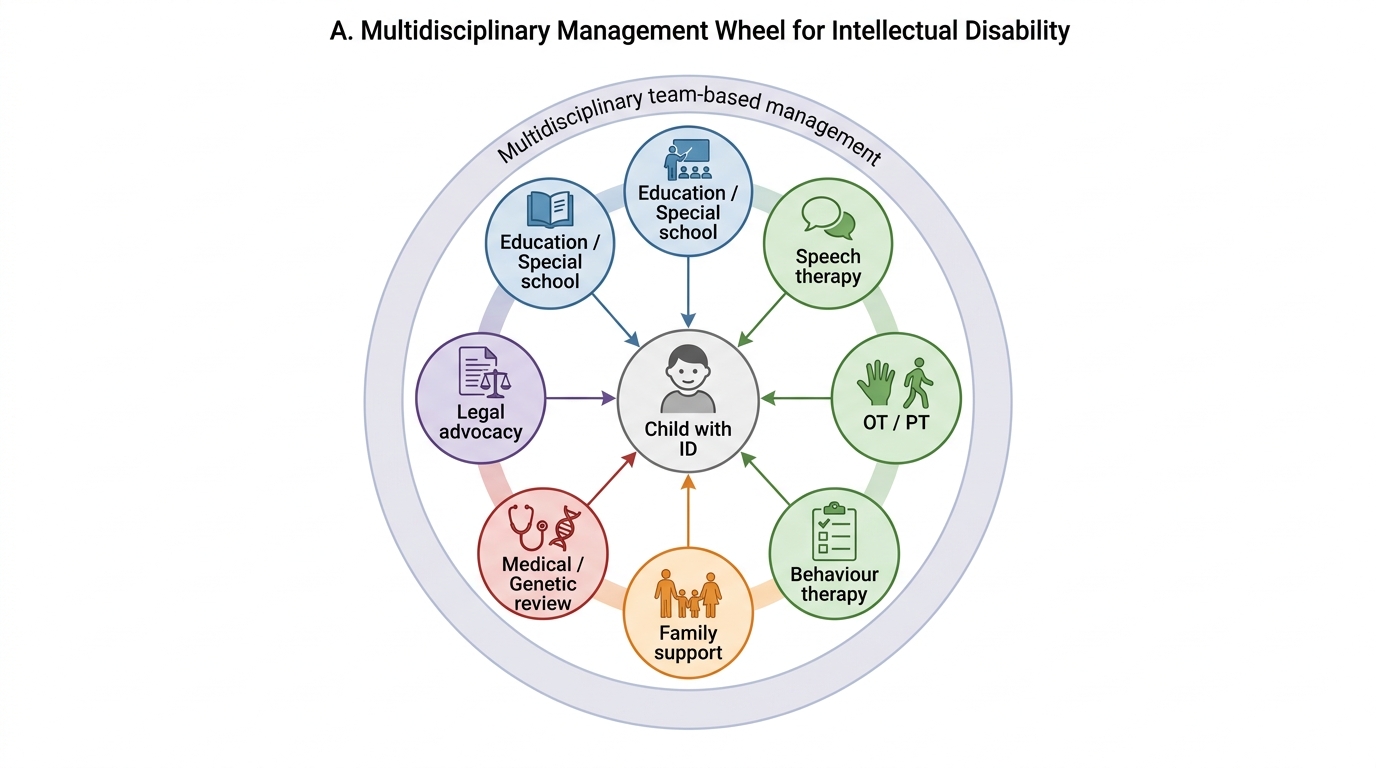
Multidisciplinary Management of Intellectual Disability
Self-Assessment — Consolidating Intellectual Disability Disorder
This self-assessment section invites you to consolidate your understanding of Intellectual Disability Disorder by reviewing the core concepts of this module. Work through each paragraph actively, testing your recall of criteria, classifications, causes, and management principles.
Diagnostic criteria. Intellectual Disability Disorder is diagnosed when three criteria co-exist: (1) significant deficits in intellectual functioning — typically IQ approximately ≤70 (2 standard deviations below the mean) on a standardised, individually administered intelligence test; (2) significant deficits in adaptive behaviour across conceptual, social, and practical domains; and (3) onset during the developmental period (childhood or adolescence). This three-part definition is consistent across ICD-11 (Disorders of intellectual development) and DSM-5. A key point for clinical examination and practice: the absence of any one of the three criteria rules out an IDD diagnosis — a low IQ in isolation, without adaptive behaviour deficits, does not constitute IDD.
Severity and the primacy of adaptive function. DSM-5 grades severity of intellectual disability based on adaptive functioning — how much support the individual needs across conceptual, social, and practical domains — rather than by IQ score. The historical IQ bands (mild 50–69, moderate 35–49, severe 20–34, profound <20) are presented in clinical training as approximate guides to understanding the IDD spectrum and as historical context, but they are explicitly not the DSM-5 severity criterion. Management planning, educational placement, and long-term support needs are determined by adaptive function, not IQ numbers.
Aetiological categories. The four aetiological categories — genetic/chromosomal (Down syndrome, Fragile X, PKU), prenatal non-genetic (congenital infections, iodine deficiency, alcohol, valproate), perinatal (birth asphyxia, prematurity, kernicterus), and postnatal (meningitis, lead poisoning, malnutrition) — provide the clinical framework for investigation and preventive counselling. Preventable causes deserve emphasis: iodine supplementation in pregnancy, newborn screening for PKU and hypothyroidism, rubella vaccination, skilled birth attendance, and prevention of neonatal jaundice are all primary-care-level interventions that can prevent intellectual disability before it occurs.
Management principles. The management of IDD is multidisciplinary and focused on maximising functional capacity, not on reversing the intellectual disability. The pillars are: early intensive intervention, special and inclusive education, speech and language therapy, occupational therapy, physiotherapy (where motor involvement is present), behaviour support, and family psychoeducation. Pharmacotherapy does not treat IDD itself but addresses co-morbidities (epilepsy, challenging behaviour, sleep disorders, anxiety). Genetic counselling and antenatal prevention strategies complete the management framework.
Differential diagnosis. The key differentials are: ASD (social communication/RRBs are the primary feature; IQ may be above the IDD threshold), specific learning disorder (circumscribed deficit in one academic domain), dementia (acquired cognitive decline in adulthood, not neurodevelopmental onset), and sensory impairment masquerading as cognitive delay. ASD and IDD frequently co-occur — both diagnoses can and should be made when criteria for both are met.
Test yourself: Can you recite the three diagnostic criteria for IDD from memory? Can you explain to an intern why DSM-5 grades severity by adaptive function rather than IQ? Can you name the most common chromosomal cause and the most common inherited cause of IDD? Can you describe at least three preventable causes of intellectual disability and the corresponding preventive intervention? Can you list the members of the multidisciplinary team involved in IDD management?
CLINICAL PEARL
The most common clinical and examination error with Intellectual Disability Disorder is to grade severity by IQ score alone, ignoring adaptive functioning. DSM-5 grades IDD severity by adaptive behaviour across conceptual, social, and practical domains — not by IQ cut-offs. A child with an IQ of 55 who is self-sufficient in daily living skills, has friendships, and can manage basic financial transactions has very different support needs from a child with the same IQ who requires full assistance with all self-care. The IQ bands (mild 50–69, moderate 35–49, severe 20–34, profound <20) are historical approximations — present them as such, and always qualify them with the adaptive functioning picture. For Down syndrome specifically: IDD severity in trisomy 21 spans the full range from mild to moderate (most commonly), and these individuals have unique medical co-morbidities (congenital heart disease, hypothyroidism, Alzheimer disease after age 40) that require lifelong proactive screening.