Page 7 of 14
RD4.3 | Clinico-radiological Correlation for Primary Care Reasoning — SDL Guide
Learning Objectives
- Explain why clinico-radiological correlation — integrating anatomy, pathophysiology and imaging findings — is a core reasoning skill for the primary-care physician.
- Apply a framework that chooses the modality from the clinical question and reads the radiological pattern back against anatomy and pathophysiology.
- Correlate osteoarthritis: synovial-joint anatomy and cartilage-loss pathophysiology with the cardinal plain-X-ray signs, recognising the clinical-radiological mismatch.
- Correlate deep vein thrombosis (Wells/D-dimer and compression ultrasonography) and acute cholecystitis (ultrasound findings including the sonographic Murphy sign).
- Build an integrated clinical-radiological narrative and communicate it across the disciplinary interface to the radiologist.
INSTRUCTIONS
Imaging never makes a diagnosis on its own; it contributes a pattern that means something only when read against the patient's anatomy, pathophysiology and clinical picture. For the primary-care physician this clinico-radiological correlation is the daily reasoning skill that turns a report into a decision and that makes a request to the radiologist intelligible. Using three conditions named in the competency — osteoarthritis, deep vein thrombosis and acute cholecystitis — this module builds the habit of integrating anatomy, the disease mechanism, and the imaging sign into one clinical narrative, and then communicating that narrative clearly to the imaging specialist.
References
- Sutton's Textbook of Radiology, 6th edition (musculoskeletal, vascular and hepatobiliary imaging) (textbook)
- Grainger & Allison's Diagnostic Radiology, 6th edition (clinico-radiological correlation) (textbook)
- Apley & Solomon's System of Orthopaedics and Fractures (osteoarthritis radiology) (textbook)
- ACR Appropriateness Criteria — suspected DVT, right upper quadrant pain, chronic joint pain (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two patients, two reports, one lesson. The first is a 68-year-old woman whose knee X-ray report reads 'severe tricompartmental osteoarthritis with marked joint-space loss and large osteophytes' — yet she walks into clinic with only mild, intermittent ache and a full daily routine. The second is a 40-year-old man whose knee looks almost normal on the same report but who is barely able to weight-bear in agony. If you treated the X-ray instead of the patient, you would operate on the wrong knee. Now a third patient: a febrile woman with right-upper-quadrant pain whose ultrasound shows gallstones, a thick gallbladder wall, and tenderness exactly under the probe. Here the image and the clinical picture lock together into a single diagnosis. Imaging, in other words, is never read in isolation — its meaning comes from correlation with anatomy, pathophysiology and the patient in front of you. Learning to make that correlation, and to communicate it, is the skill this module builds.
WHY THIS MATTERS
Clinico-radiological correlation is the reasoning engine of everyday clinical practice, and NMC competency RD4.3 names it explicitly: for diseases the primary-care physician commonly meets — osteoarthritis on X-ray, deep vein thrombosis, and cholecystitis — you must apply anatomical-radiological-pathophysiology correlations as a basis for clinical reasoning and inter-disciplinary communication. This matters for two reasons. First, an imaging finding interpreted without its clinical and anatomical context misleads: severe osteoarthritis on film may be near-silent, an incidental finding may be over-treated, and a normal scan may falsely reassure when the pre-test probability is high. Second, correlation is the language you share with the radiologist: a request that says '?DVT left calf, Wells score 2, D-dimer positive' or '?acute cholecystitis, Murphy positive, please assess gallbladder wall and for stones' tells the radiologist exactly what to look for and why. The skill is tested in clinical reasoning stations and in every case discussion, and it is what makes you a competent partner to the imaging service rather than a passive consumer of reports.
RECALL
Before reading further, bring forward the anatomy and modality principles you will integrate here:
- Synovial joint anatomy (from Year-1 anatomy): articular (hyaline) cartilage covering bone ends, the joint space (the radiolucent gap on X-ray that represents cartilage), the synovium and capsule, and subchondral bone beneath the cartilage.
- Deep venous anatomy of the leg: the deep veins (femoral, popliteal, calf veins) that ultrasound interrogates; a normal vein is fully compressible by the probe.
- Virchow's triad (the pathophysiology of thrombosis): venous stasis, endothelial injury, and hypercoagulability.
- Biliary anatomy: the gallbladder, cystic duct, and common bile duct; obstruction of the cystic duct underlies acute cholecystitis.
- Modality-choice principle (from the foundation module): ultrasound first for biliary and vascular questions and in pregnancy/children; plain X-ray first for bone; the modality is chosen from the clinical question.
If the synovial-joint, deep-venous or biliary anatomy is hazy, a quick review of your anatomy notes will make the correlations below much sharper.
Why Clinico-radiological Correlation Is the Primary Physician's Core Skill
Clinico-radiological correlation is the disciplined practice of reading every imaging finding against three things at once: the relevant anatomy, the disease's pathophysiology, and the individual patient's clinical picture. It is the single skill that separates a clinician who uses imaging well from one who is led astray by it. An image is a pattern, not a diagnosis; the same shadow can be trivial in one patient and critical in another, and only the clinical context tells you which. This is why a radiology report so often ends 'clinical correlation advised' — the radiologist is reminding you that the final synthesis of image plus patient is yours to make. For the primary-care physician, who is frequently the first to see the patient and the one who must act on the report, this correlation is not an academic nicety but the daily basis of safe decisions.
Doing this well has two practical halves, both of which RD4.3 requires:
- Reasoning: integrating anatomy, pathophysiology and the imaging sign into one coherent clinical narrative, so that the finding is understood mechanistically (why this sign appears in this disease) rather than merely recognised.
- Inter-disciplinary communication: translating that narrative into a precise request and discussion with the radiologist, so the right modality is chosen and the right question is answered.
A recurring trap that correlation guards against is clinical-radiological mismatch — most strikingly in osteoarthritis, where the severity of the X-ray and the severity of the symptoms correlate poorly. The next sections build the correlation framework and then apply it to the three conditions the competency names.
The Correlation Framework — Anatomy, Pathophysiology, Imaging
The governing framework for clinico-radiological correlation can be stated as a sequence that runs in both directions between the clinic and the imaging. Forward, the clinical question determines the appropriate modality; backward, the imaging pattern is read against the anatomy and pathophysiology to confirm or refute the hypothesis. The discipline is to never treat the image as a free-standing fact: every sign has an anatomical location and a pathophysiological cause, and understanding both is what lets you interpret it correctly and explain it to the radiologist. This bidirectional habit also protects against two opposite errors — ordering the wrong test for the question, and then over-reading or under-reading whatever that test produces — because at each step the clinical reasoning constrains what the image is allowed to mean. It is a deliberately slow, explicit process at first; with practice it becomes the automatic way an experienced clinician moves from a presenting complaint to a targeted study to a confident interpretation.
The framework, applied to any presentation:
- Start from the clinical question and choose the modality from it. Bone and joint structure are seen on plain X-ray; soft tissue, fluid and flow are seen on ultrasound (no ionising radiation, real-time, first-line for vascular and biliary questions and in pregnancy/children). The modality follows the question, not habit.
- Map the relevant anatomy. Know what structure the modality is interrogating (the joint space and subchondral bone; the deep vein lumen; the gallbladder wall and lumen).
- Connect the pathophysiology to the expected sign. Ask what the disease does to that anatomy and therefore what the image should show (cartilage loss narrows the joint space; thrombus fills and fixes the vein so it will not compress; cystic-duct obstruction inflames and thickens the gallbladder wall).
- Read the pattern back against the clinic. Confirm the sign matches the hypothesis, weigh pre-test probability, and watch for clinical-radiological mismatch (severe imaging with mild symptoms, or vice versa).
- Communicate the correlation. State the specific question and your provisional correlation to the radiologist so the study targets it.
This framework is now applied to osteoarthritis, deep vein thrombosis, and acute cholecystitis in turn.
Worked Correlation 1 — Osteoarthritis on Plain X-ray
Osteoarthritis is the clearest teaching example of clinico-radiological correlation because its anatomy, pathophysiology and radiographic signs map onto one another precisely — and because it is the condition where clinical-radiological mismatch is most pronounced. The relevant anatomy is the synovial joint: hyaline articular cartilage capping the bone ends, the joint space (the radiolucent gap that on X-ray represents the otherwise invisible cartilage), the subchondral bone beneath it, and the joint margins. The pathophysiology is progressive loss of articular cartilage with secondary changes in the underlying and surrounding bone: as cartilage thins, the bones approximate, the subchondral bone is overloaded and reacts, and new bone forms at the unloaded margins. Plain X-ray (ideally weight-bearing for the knee, so the true joint space under load is seen) is the appropriate first-line modality because it directly shows these bony and joint-space changes.
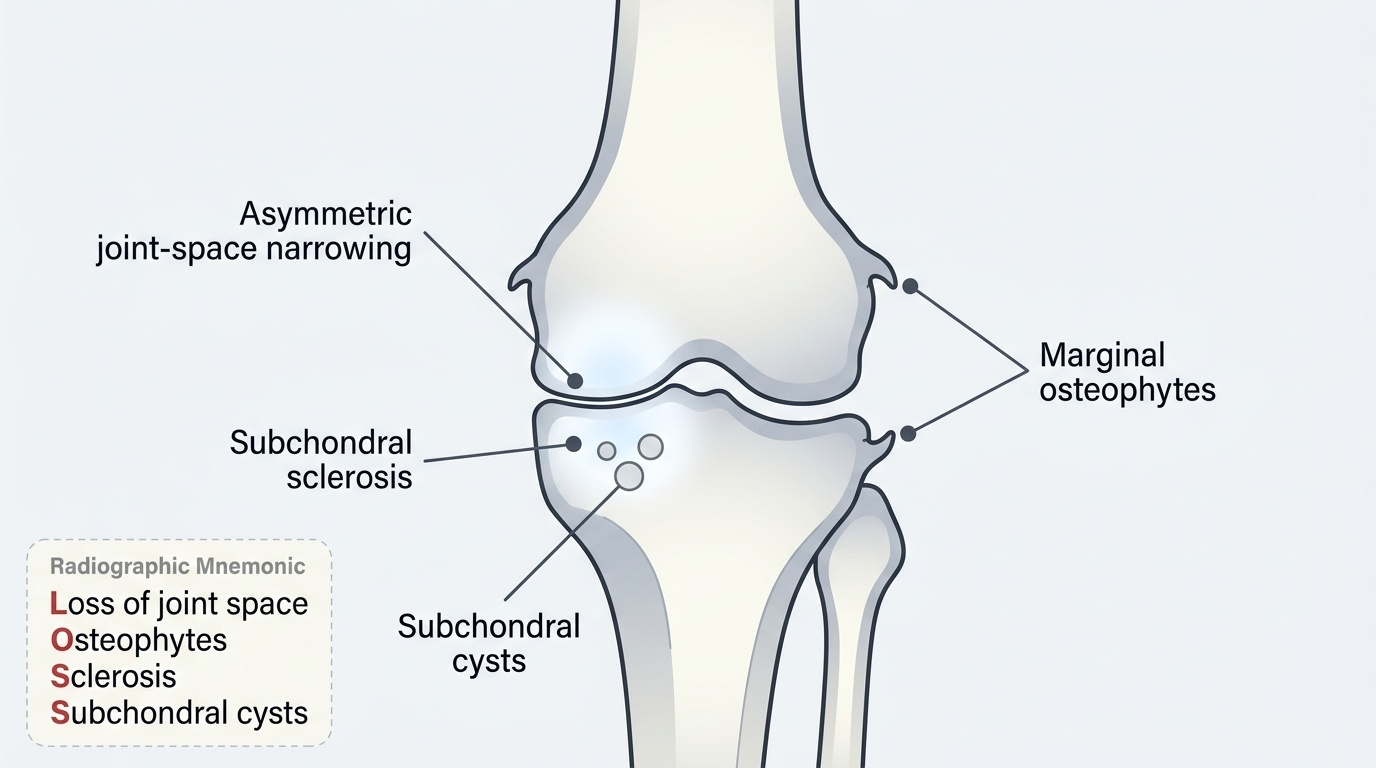
The four cardinal radiographic signs of osteoarthritis, each tied to the pathophysiology (mnemonic LOSS):
- Loss of joint space (joint-space narrowing): cartilage loss reduces the radiolucent gap; characteristically asymmetric (affecting the loaded compartment), unlike the symmetric narrowing of inflammatory arthritis.
- Osteophytes: bony outgrowths at the joint margins, formed where cartilage and bone remodel at the periphery.
- Subchondral sclerosis: increased density (whiteness) of the bone immediately beneath the cartilage, from reactive new bone in response to increased load.
- Subchondral cysts (geodes): lucent cavities in the subchondral bone, formed by synovial fluid intrusion or microfracture through the damaged surface.
Crucially, the radiographic severity correlates poorly with symptoms: a knee with marked narrowing and large osteophytes may be only mildly painful, and a near-normal film may accompany severe pain. The clinical implication is decisive — treat the patient, not the X-ray. This mismatch is exactly why correlation, not image-reading alone, is the competency.
Provided image
SELF-CHECK
A 66-year-old woman has chronic right knee pain. Her weight-bearing knee X-ray shows asymmetric medial joint-space narrowing, marginal osteophytes, subchondral sclerosis and a subchondral cyst. Which statement best reflects correct clinico-radiological correlation?
A. The X-ray confirms osteoarthritis, and the severity of these findings reliably predicts the severity of her pain
B. The findings are the cardinal signs of osteoarthritis, but radiographic severity correlates poorly with symptoms, so management is guided by the clinical picture
C. Symmetric narrowing of this kind indicates rheumatoid arthritis rather than osteoarthritis
D. Subchondral cysts indicate infection and require urgent aspiration
Reveal Answer
Answer: B. The findings are the cardinal signs of osteoarthritis, but radiographic severity correlates poorly with symptoms, so management is guided by the clinical picture
Asymmetric joint-space narrowing, marginal osteophytes, subchondral sclerosis and subchondral cysts (LOSS) are the cardinal radiographic signs of osteoarthritis; however, radiographic severity correlates poorly with symptom severity, so management is guided by the patient's clinical picture, not the X-ray grade. The narrowing in OA is characteristically asymmetric (loaded compartment), unlike the symmetric narrowing of inflammatory arthritis, and subchondral cysts are part of OA, not a sign of infection.