Page 8 of 14
RD4.3 | Clinico-radiological Correlation for Primary Care Reasoning — SDL Guide (Part 2)
Worked Correlations 2 and 3 — DVT on Doppler and Cholecystitis on Ultrasound
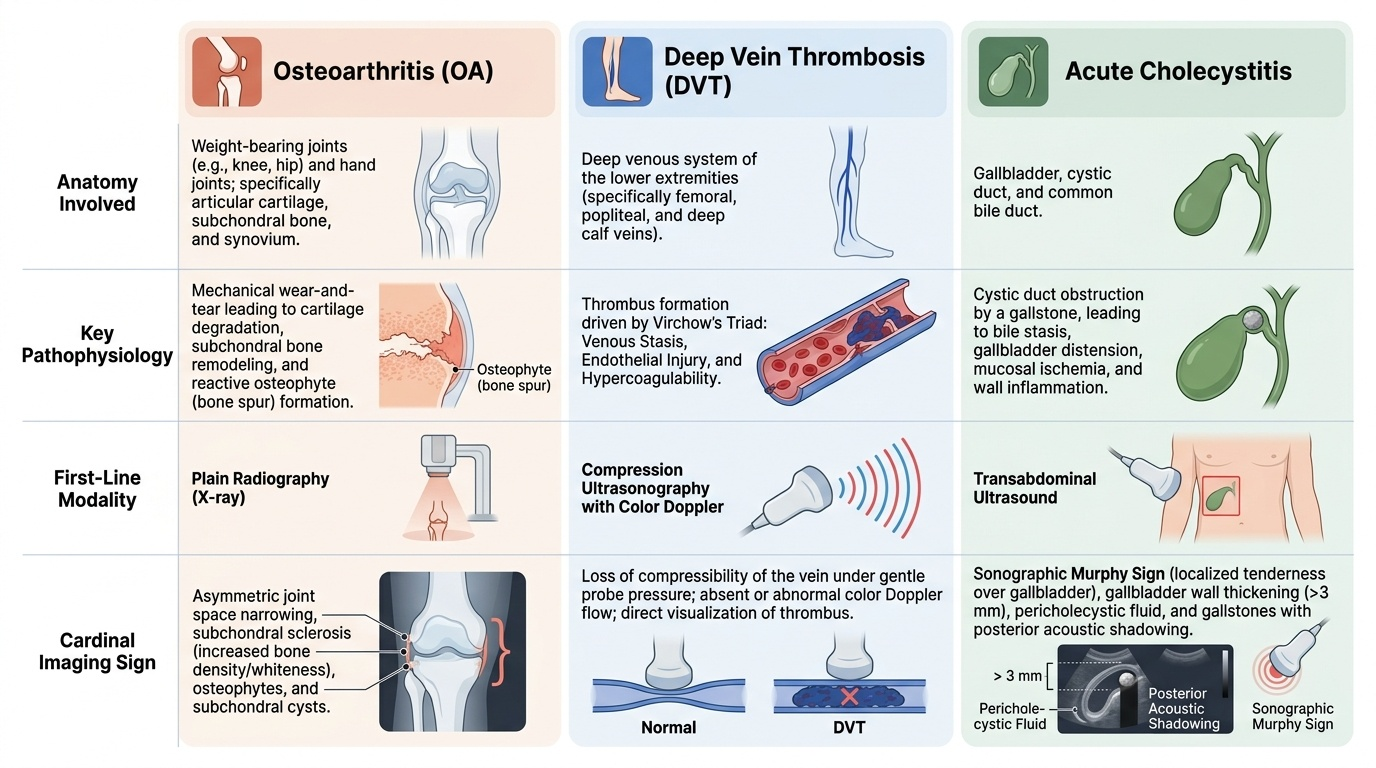
Deep vein thrombosis and acute cholecystitis extend the same correlation discipline to ultrasound, where the modality is chosen because it images soft tissue, fluid and flow in real time without ionising radiation, and where the cardinal sign in each case follows directly from the pathophysiology. In both, the clinical assessment does real work before the scan: it sets the pre-test probability and frames the specific question put to the radiologist.
Deep vein thrombosis (DVT). The anatomy is the deep venous system of the leg (femoral, popliteal and calf veins); the pathophysiology is thrombus formation driven by Virchow's triad (stasis, endothelial injury, hypercoagulability). Clinical reasoning starts with a validated pre-test probability rule, the Wells score, combined with D-dimer: a low Wells probability with a negative high-sensitivity D-dimer can exclude DVT without imaging, whereas a raised probability or positive D-dimer directs the patient to ultrasound. The first-line modality is compression ultrasonography with colour Doppler. The cardinal sign is loss of compressibility: a normal vein collapses completely under gentle probe pressure, whereas a vein filled with thrombus will not compress. Doppler adds absent or abnormal flow, and thrombus may be directly visible in the lumen. The correlation is exact — thrombus physically fills and fixes the lumen, so the vein cannot be squeezed shut.
Acute cholecystitis. The anatomy is the gallbladder, cystic duct and common bile duct; the pathophysiology is usually cystic-duct obstruction by a gallstone, causing gallbladder distension, wall inflammation and oedema. The first-line modality is ultrasound. The cardinal findings are: gallstones (echogenic foci with posterior acoustic shadowing); gallbladder wall thickening (>3 mm in a fasted, non-contracted gallbladder); pericholecystic fluid; and the sonographic Murphy sign — maximal tenderness elicited when the transducer is pressed directly over the sonographically localised gallbladder, which is more specific than the clinical Murphy sign because the point of tenderness is confirmed to be the gallbladder itself. Each sign follows from the mechanism: the stone is the obstruction, the thick wall and pericholecystic fluid are the inflammatory response, and the focal tenderness is the inflamed organ under the probe.
Provided image
SELF-CHECK
A 55-year-old immobile post-operative patient has a swollen, tender left calf. Wells score is moderate-to-high and D-dimer is positive. Compression ultrasonography is performed. Which single finding is the cardinal sign confirming deep vein thrombosis?
A. A fully compressible popliteal vein that collapses under probe pressure
B. A non-compressible vein segment that will not collapse under probe pressure, indicating intraluminal thrombus
C. Increased echogenicity of the surrounding subcutaneous fat
D. A thickened arterial wall on the same side
Reveal Answer
Answer: B. A non-compressible vein segment that will not collapse under probe pressure, indicating intraluminal thrombus
The cardinal sign of DVT on compression ultrasonography is loss of compressibility — a vein filled with thrombus will not collapse under gentle probe pressure, whereas a normal vein compresses completely. This follows directly from the pathophysiology: thrombus physically fills and fixes the lumen. A fully compressible vein argues against DVT; subcutaneous fat echogenicity and arterial wall thickening are not the diagnostic sign for venous thrombosis.
Applied Practice — Correlating and Communicating Across the Interface
The final step in clinico-radiological correlation is to assemble anatomy, pathophysiology and the expected imaging sign into a single clinical narrative and then to communicate that narrative precisely to the radiologist, because correlation done silently in your own head does not help the patient unless it shapes the request and the discussion. A well-correlated request names the specific question, gives the radiologist the clinical reasoning, and states what you expect the study to show — which both directs the search and lets the radiologist add value by confirming, refuting or refining your hypothesis.
Worked applied case — correlating and communicating. A 58-year-old woman presents with right-upper-quadrant pain and fever for a day, with a positive clinical Murphy sign. Correlate: the anatomy (gallbladder/cystic duct), the likely pathophysiology (cystic-duct obstruction with inflammation), and the modality of choice (ultrasound). Then communicate the correlation in the requisition: '?acute cholecystitis — RUQ pain and fever 24 h, clinical Murphy positive; please assess for gallstones, gallbladder wall thickening, pericholecystic fluid and a sonographic Murphy sign. Not pregnant. Urgent — same day.' This single line carries the question, the reasoning and the expected signs, so the sonographer knows exactly what to look for and the report comes back addressing your actual concern.
Principles for communicating the correlation across the interface:
- State the specific question and your provisional correlation, not just a body part — '?DVT left calf, Wells 2, D-dimer positive' rather than 'leg USG'.
- Give the relevant pathophysiological context (immobility for DVT, positive Murphy for cholecystitis) so the radiologist can weigh pre-test probability.
- Name the signs you expect where helpful, inviting the radiologist to confirm or refute and to report mismatch.
- Read the report back against your correlation: if the imaging contradicts a strong clinical suspicion, discuss it with the radiologist rather than dismissing either the clinic or the image — the resolution of clinical-radiological mismatch is a shared, two-way conversation.
This closed correlation-and-communication loop is the full expression of RD4.3: reasoning from anatomy and pathophysiology to the image, and back into a precise inter-disciplinary dialogue.
CLINICAL PEARL
Pearl 1 — Treat the patient, not the X-ray, in osteoarthritis. Radiographic severity and symptom severity correlate poorly; a dramatic film may be near-silent and a bland film may accompany severe pain. Management follows the clinical picture.
Pearl 2 — In DVT, the diagnostic sign is what the vein will NOT do. A normal vein compresses completely; a thrombosed vein will not collapse under the probe. Loss of compressibility is the cardinal sign — and pair the scan with Wells + D-dimer, which decide who even needs it.
Pearl 3 — The sonographic Murphy sign beats the clinical one. Tenderness elicited with the transducer directly over the sonographically localised gallbladder is more specific than bedside Murphy, because the point of pain is confirmed to be the gallbladder itself. Wall thickening >3 mm, stones and pericholecystic fluid complete the picture.
Pearl 4 — Correlation is a two-way conversation. When a strong clinical suspicion and the imaging disagree, talk to the radiologist; resolving clinical-radiological mismatch together is the skill, not choosing one over the other by reflex.
Self-Assessment — Clinico-radiological Correlation
Use these scenarios to test whether you can correlate anatomy, pathophysiology and imaging and communicate the result. Write your answer before reading the discussion.
Scenario A: A 70-year-old man's knee X-ray is reported as 'severe osteoarthritis with marked joint-space loss and osteophytes', but he reports only mild ache and walks well. The surgical team asks whether the X-ray indicates joint replacement. How do you correlate and advise?
Discussion: The X-ray shows the cardinal LOSS signs of osteoarthritis, but radiographic severity correlates poorly with symptoms; decisions about intervention such as arthroplasty are driven by symptoms, function and quality of life, not by the radiographic grade. Correct correlation here is to treat the patient, not the film: with mild symptoms and good function, conservative management is appropriate, and the marked X-ray changes alone do not justify surgery. This is the textbook clinical-radiological mismatch the competency highlights.
Scenario B: A 48-year-old woman with a swollen tender calf has a LOW Wells score and a negative high-sensitivity D-dimer. The intern wants to book compression ultrasonography anyway. What does correct correlation suggest?
Discussion: Clinical reasoning precedes imaging in DVT. A low pre-test probability (Wells) combined with a negative high-sensitivity D-dimer can exclude DVT without imaging, so routine compression ultrasonography is not required in this low-probability, D-dimer-negative patient. Correlation means using the validated pre-test pathway to decide who needs the scan — ordering ultrasound reflexively in a low-probability, D-dimer-negative patient is poor resource use and is not what the algorithm supports. (A raised probability or positive D-dimer would direct the patient to ultrasound.)
Scenario C: A febrile patient with right-upper-quadrant pain has an ultrasound showing gallstones, a 5 mm gallbladder wall, pericholecystic fluid and a positive sonographic Murphy sign. Correlate each finding with its mechanism and write the one-line correlation you would communicate.
Discussion: Each finding maps to the pathophysiology of cystic-duct obstruction and inflammation: gallstones are the obstructing cause; wall thickening >3 mm (here 5 mm) and pericholecystic fluid are the inflammatory response; the sonographic Murphy sign localises maximal tenderness to the inflamed gallbladder. A communicated correlation: 'US confirms acute calculous cholecystitis — gallstones, GB wall 5 mm, pericholecystic fluid, sonographic Murphy positive; correlates with the clinical RUQ pain and fever.' This integrates anatomy, mechanism and image into one inter-disciplinary statement, exactly as RD4.3 requires.