Page 4 of 14
RD4.2 | Safe Transport of Critically Ill Patients for Imaging — SDL Guide
Learning Objectives
- Explain why intra-hospital transport of a critically ill patient for imaging is a high-risk procedure and when it is justified versus portable imaging.
- State the governing principles of safe transport: justification, pre-transport stabilisation, continuity of monitoring and therapy, and a trained escort.
- Apply a systematic pre-transport checklist, including estimating whether the oxygen-cylinder reserve is adequate for the journey.
- Describe the MRI safety environment — Zones I to IV, the ferromagnetic projectile hazard, implant screening, and MRI-conditional versus MRI-unsafe equipment.
- Conduct a structured handover and respond to deterioration during transport.
INSTRUCTIONS
Moving a critically ill patient out of the controlled environment of the ICU or resuscitation room to the radiology department is one of the most hazardous routine tasks in hospital medicine. The patient leaves behind wall oxygen, full monitoring, and a team, and enters a corridor and a scanner room where deterioration is common and help is further away. NMC competency RD4.2 requires you to apply appropriate safety measures during this transport — checking the oxygen supply and observing the correct precautions in the MRI room being named explicitly. This module turns those requirements into a practical, checklist-driven skill so that the imaging study you ordered does not become the most dangerous part of the patient's day.
References
- Grainger & Allison's Diagnostic Radiology, 6th edition, Chapter 1 (Principles and Safety) (textbook)
- Sutton's Textbook of Radiology, 6th edition (MRI safety and the imaging environment) (textbook)
- Intensive Care Society / AAGBI guidelines for the transport of the critically ill adult (trained escort, monitoring continuity, pre-transport checklist) (guideline)
- ACR Manual on MR Safety — MRI zones, screening, and MR-conditional equipment (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 6-year-old boy needed a brain MRI. A nurse, hurrying, wheeled a standard steel oxygen cylinder into the magnet room to keep the sedated child supplied. As she crossed the threshold of the scanner, the 1.5-Tesla magnet seized the ferromagnetic cylinder and hurled it across the room into the bore at the patient's head. This is not a hypothetical: a real, widely reported fatality occurred in exactly this way, and similar projectile incidents recur wherever the MRI environment is not respected. Now picture a different journey: a ventilated adult with a head injury being wheeled to CT when, halfway down the corridor, the portable oxygen cylinder — never checked before departure — runs dry, and the team has no spare. Both disasters were entirely preventable. Both turn on the same truth: transporting a critically ill patient for imaging is itself a procedure with its own risks, and it must be performed with the same discipline as any other procedure.
WHY THIS MATTERS
Every time you send a sick patient to radiology, you are accepting a trade: the diagnostic information the scan provides against the real risk of moving the patient. NMC competency RD4.2 makes this an explicit competency — applying appropriate safety measures when transporting critically ill patients for imaging, with checking the adequacy of the oxygen cylinder and following correct precautions in the MRI room named specifically. Adverse events during intra-hospital transport are common and well documented: hypoxia from oxygen running out or a disconnected circuit, loss of monitoring, displaced lines and tubes, hypotension, and — uniquely in MRI — catastrophic ferromagnetic projectile injuries. These are not radiology-department problems; the requesting and transferring clinical team owns the patient's safety in transit. As a primary-care physician or junior doctor you will personally organise, accompany, or hand over these transfers, and the difference between a safe journey and a near-miss is almost always a checklist that was, or was not, completed before the trolley left the unit.
RECALL
Before reading further, recall the relevant background from the radiology foundation module and basic clinical care:
- MRI uses a powerful static magnetic field (typically 1.5-3 Tesla) that is always on, even when no scan is running. It exerts strong attractive force on ferromagnetic (iron-containing) objects.
- MRI has real contraindications and hazards — certain pacemakers/ICDs, cochlear implants, ferromagnetic intra-ocular foreign bodies, some aneurysm clips, and any loose ferromagnetic object that can become a projectile.
- Oxygen is a finite cylinder supply during transport: unlike wall oxygen, a portable cylinder holds a fixed volume that depletes with use and must be calculated against the journey time.
- Critically ill patients need continuous monitoring — at minimum oxygen saturation, ECG and blood pressure, plus capnography (end-tidal CO2) for any intubated patient.
- The controlled environment of an ICU/resus bay (wall gases, suction, full monitoring, immediate help) is left behind during transport and must be substituted by portable equivalents.
If the MRI physics or contraindications feel hazy, a quick review of the foundation module will make the MRI-room precautions below much clearer.
Why Moving a Critically Ill Patient Is Itself a Risk
The fundamental hazard of transporting a critically ill patient for imaging is that transport strips away the controlled environment that is keeping the patient alive and replaces it, temporarily, with a far more fragile portable setup. In the ICU or resuscitation room the patient has wall oxygen that never runs out, suction, full continuous monitoring, infusion pumps on mains power, and a team within arm's reach. The moment the trolley leaves the unit, every one of those becomes a portable, finite, fallible substitute: a cylinder that can empty, a battery that can die, a monitor that can be left behind, an infusion that can stop, and help that is now minutes rather than seconds away. It is unsurprising, then, that a substantial proportion of intra-hospital transfers are complicated by an adverse event, the majority of which are predictable and preventable.
This risk has two practical implications for the clinician:
- The transport must be justified. Before moving the patient, ask whether the imaging will change management enough to be worth the risk of the journey, and whether a portable alternative (bedside chest X-ray, bedside ultrasound) could answer the question without moving the patient at all. The safest transport is sometimes the one you do not undertake.
- If transport is justified, it must be prepared as a procedure. The deterioration that occurs en route is rarely novel — it is usually the patient's existing physiology behaving predictably once support is reduced. Anticipating it with stabilisation, a checklist, adequate portable support, and the right people is what converts a high-risk move into a controlled one.
The rest of this module builds that controlled procedure: the governing principles, the pre-transport checklist, the special case of the MRI room, and the handover.
Governing Principles of Safe Intra-Hospital Transport
Safe transport rests on a small set of governing principles that apply to every critically ill transfer regardless of destination, and which the detailed checklist later operationalises. The overarching principle is that the standard of care must not fall during the journey: the patient should receive essentially the same monitoring, oxygenation, and therapy in the corridor and the scanner as they were receiving in the unit. A second principle is that deterioration is to be anticipated and prepared for, not merely reacted to — the team carries the drugs, airway equipment and oxygen reserve needed to manage the most likely problems before they leave, rather than improvising once a problem has already developed in a corridor. A third principle is that the transfer is a planned team activity, not a solo errand: the right people, the right equipment, and the receiving department's readiness are arranged in advance so that the journey is as short and as supported as possible.
The governing principles, in order:
- Justify the transfer. Confirm the imaging will change management and that no adequate bedside alternative exists; an unjustified transfer is an unjustified risk.
- Stabilise before you move. Optimise airway, breathing and circulation in the relative safety of the unit first; a patient who is unstable at the bedside will be more unstable in a corridor.
- Continuity of monitoring and therapy. Maintain continuous SpO2, ECG and blood-pressure monitoring (and capnography if ventilated), and keep infusions and oxygen running without interruption throughout.
- A trained escort. At minimum, a competent practitioner able to manage the patient's airway and anticipated deterioration must accompany the patient; an unstable or ventilated patient typically requires a doctor plus a nurse or other trained staff.
- Adequate portable equipment and reserve. Sufficient oxygen (with a safety margin), a working transport monitor, emergency airway and resuscitation drugs, and secured lines and tubes.
- Communication. The receiving area (radiology) is told the patient is coming, their status, and any special needs; the journey is planned (lift availability, route) to minimise time outside the unit.
These principles are universal; the next section turns them into a concrete, do-not-skip checklist.
The Pre-Transport Checklist — Oxygen, Monitoring, Drugs, People
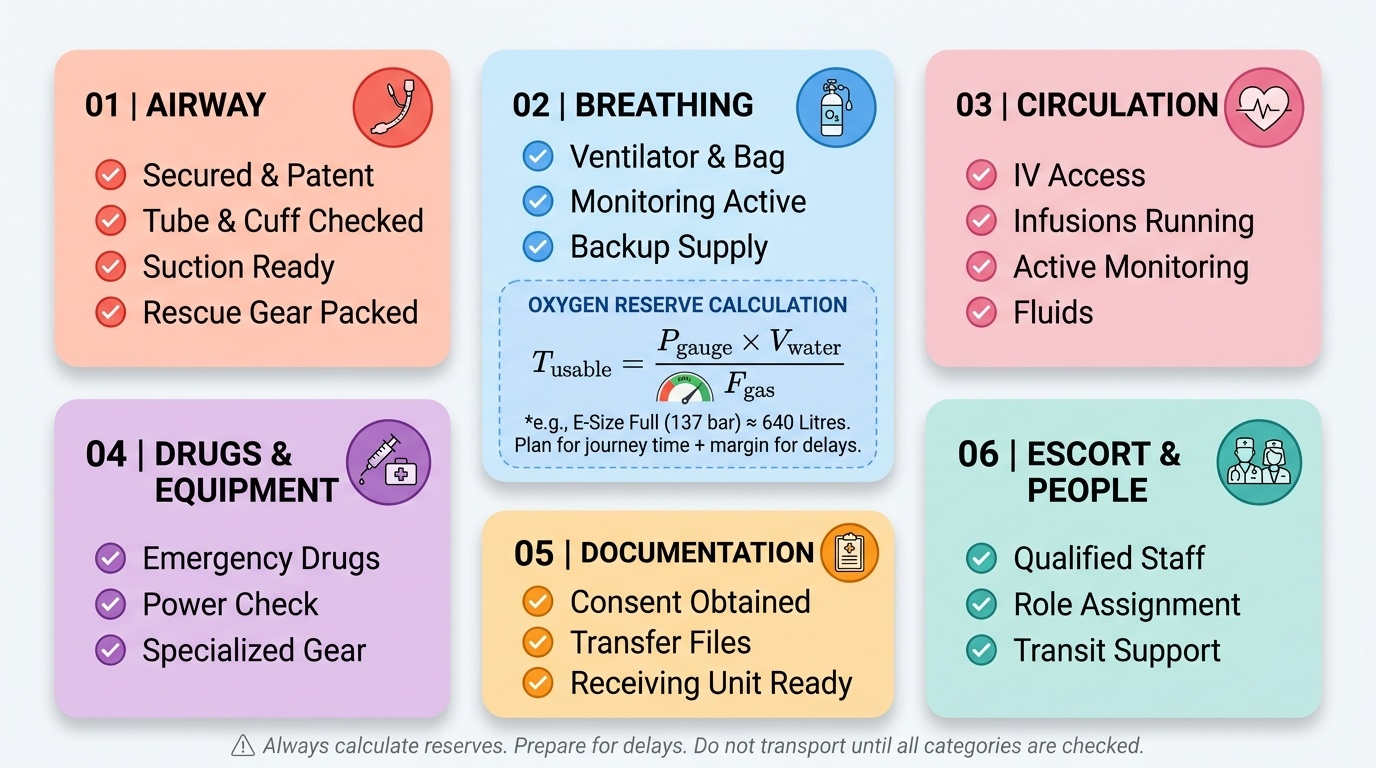
A checklist is the practical instrument that prevents the predictable transport disaster, because under time pressure even experienced staff forget a step, and the steps that get forgotten — checking the oxygen, charging the monitor — are exactly the ones that kill. The most clinically important single calculation is the oxygen reserve: a portable cylinder holds a fixed volume of gas, and you must confirm it exceeds the patient's anticipated consumption for the whole journey plus a margin for delays (a stuck lift, a queue at the scanner). A practical estimate of the gas remaining in a cylinder is the gauge pressure multiplied by the cylinder's water capacity; for example, a common E-size cylinder full at roughly 137 bar holds about 640 litres, and the usable time equals the available litres divided by the total fresh-gas flow in litres per minute. Always plan for more than the expected journey time — running out of oxygen in a corridor is a wholly avoidable emergency.
A systematic pre-transport checklist, organised ABCDE-style:
- Airway: airway secured and patent; tube position and cuff checked; suction available; airway rescue equipment (bag-valve-mask, spare tube, laryngoscope) packed.
- Breathing: oxygen-cylinder reserve calculated and confirmed adequate for journey + delay margin; spare cylinder considered; transport ventilator settings checked or self-inflating bag available; SpO2 and capnography (if ventilated) running.
- Circulation: secure IV access (ideally two points); infusions running on charged pumps with adequate drug volume; ECG and blood-pressure monitoring; fluids available.
- Drugs and equipment: emergency/resuscitation drugs (e.g. for sedation, vasopressors, the patient's running infusions), defibrillator if indicated, all equipment battery-charged.
- Documentation and Destination: notes, observation chart and any consent with the patient; the receiving area informed and ready; route and lift planned.
- Escort (People): a trained escort competent to manage the airway and anticipated deterioration; numbers matched to patient acuity (a ventilated patient needs a doctor plus assistant).
Provided image
SELF-CHECK
You are preparing to transport a ventilated patient from the ICU to the CT scanner. The portable oxygen cylinder gauge and your estimate suggest it holds enough gas for about 12 minutes at the current flow. The round trip, including a likely wait for the scanner, is expected to take about 25 minutes. What is the correct action?
A. Proceed; the cylinder will probably last because flows are usually overestimated
B. Proceed but disconnect oxygen during the corridor portion to conserve gas
C. Do not depart until oxygen supply (a fuller or additional cylinder) adequate for the journey plus a safety margin is secured
D. Reduce the patient's oxygen requirement by briefly hyperventilating before leaving
Reveal Answer
Answer: C. Do not depart until oxygen supply (a fuller or additional cylinder) adequate for the journey plus a safety margin is secured
The oxygen reserve must exceed the anticipated journey time with a margin for delays; a 12-minute supply for a 25-minute round trip is inadequate, so departure must wait until a fuller or additional cylinder is secured. Proceeding and hoping, disconnecting oxygen, or pre-hyperventilating are all unsafe — running out of oxygen in transit is a preventable emergency, and checking cylinder adequacy is the safety measure RD4.2 names explicitly.