Page 5 of 14
RD4.2 | Safe Transport of Critically Ill Patients for Imaging — SDL Guide (Part 2)
The MRI Environment — Zones, Projectile Hazard and MRI-Conditional Equipment
The MRI suite demands a layer of safety precautions that no other imaging environment requires, because the magnet is always on and exerts a powerful attractive force on ferromagnetic objects — a force that turns an ordinary steel oxygen cylinder, a pair of scissors, or a wheelchair into a lethal projectile. Interpreting the MRI environment correctly means understanding that safety is built around controlled access through a series of zones and around the strict separation of MRI-safe from MRI-unsafe equipment and implants. This is the precaution RD4.2 names specifically, and it is enforced by physical zoning so that nothing and no-one reaches the magnet without being screened first. The danger is invisible and counter-intuitive: there is no spark, no noise and no warning, the field cannot be switched off between patients, and the attractive force grows rapidly as an object nears the bore, so an item that feels safely held a few steps away can be wrenched from the hand and accelerated into the scanner without any chance to react.
The MRI safety framework:
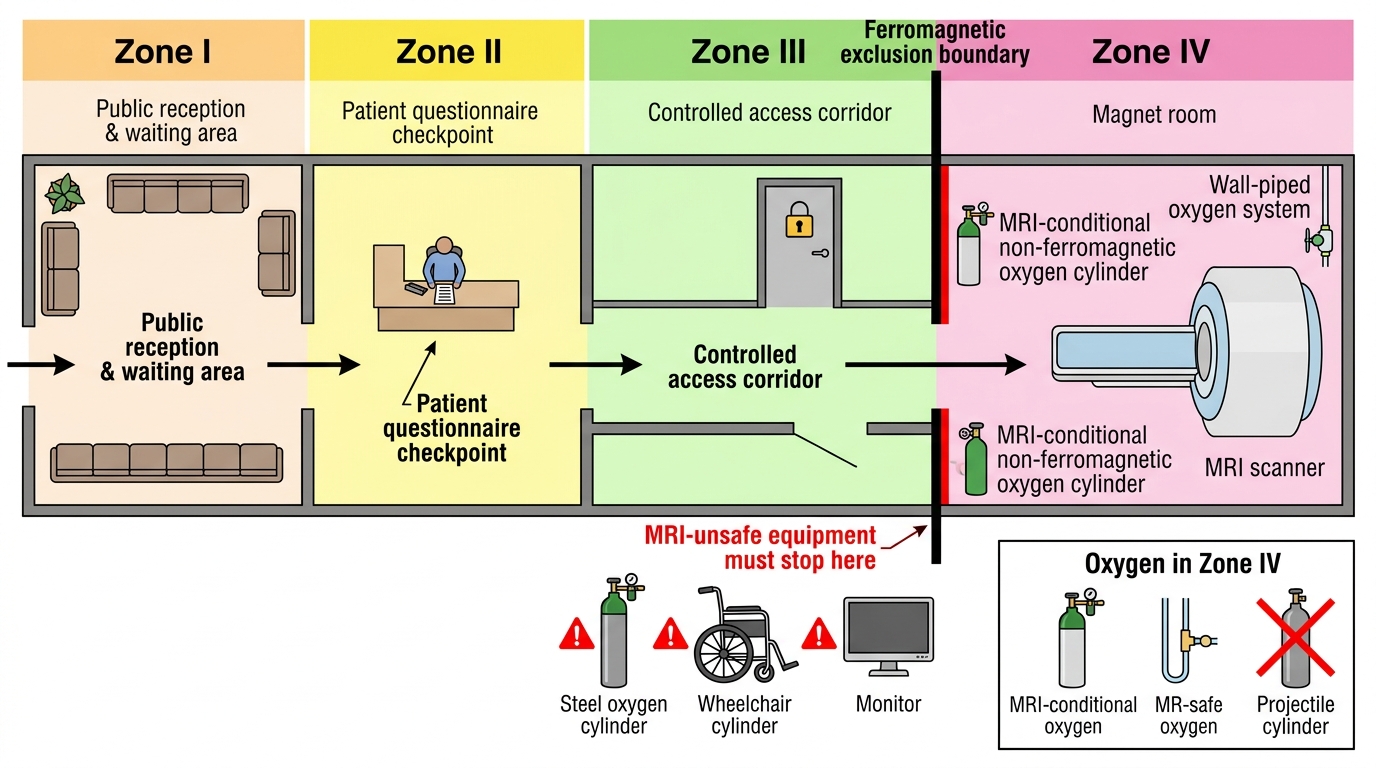
- The four safety zones: Zone I is freely accessible public space outside the MRI environment. Zone II is the interface where patients are greeted and screened (history, implant and metal screening). Zone III is a controlled, access-restricted region (including the control room) that ferromagnetic objects and unscreened people must not enter. Zone IV is the magnet (scanner) room itself — the area of greatest hazard, entered only after screening, and where MRI-unsafe equipment must never go.
- The ferromagnetic projectile hazard: any iron-containing object brought near the magnet can be pulled violently into the bore. Standard steel oxygen cylinders, conventional monitors, infusion pumps, ventilators, trolleys, scissors and pens are MRI-unsafe and must stop at the Zone III/IV boundary.
- MRI-conditional versus MRI-unsafe: MRI-conditional equipment (non-ferromagnetic/aluminium oxygen cylinders, MR-conditional monitors, ventilators and infusion pumps) may enter the magnet room under specified conditions; MRI-unsafe equipment may not. A critically ill patient can only go into Zone IV with MR-conditional support equipment.
- Implant and foreign-body screening: every patient and accompanying staff member is screened for pacemakers/ICDs, cochlear implants, aneurysm clips and ferromagnetic intra-ocular foreign bodies before entering Zone IV.
- Emergencies in the magnet room: in a cardiac arrest, the patient is removed from Zone IV to a safe area to resuscitate (standard resuscitation equipment is MRI-unsafe); a magnet quench (emergency rapid loss of the field) is reserved for situations where a person is pinned by a ferromagnetic object and the field must be killed.
MRI Safety Zones and Equipment Control
SELF-CHECK
A sedated, spontaneously breathing patient needs an urgent MRI brain and requires supplemental oxygen during the scan. What is the correct way to provide oxygen inside the magnet (Zone IV) room?
A. Wheel the standard steel oxygen cylinder from the ward into the magnet room
B. Use only an MRI-conditional (non-ferromagnetic) oxygen cylinder or the room's piped MR-safe oxygen supply
C. Disconnect oxygen for the duration of the scan to avoid bringing any cylinder in
D. Place the steel cylinder just inside the door, away from the centre of the magnet
Reveal Answer
Answer: B. Use only an MRI-conditional (non-ferromagnetic) oxygen cylinder or the room's piped MR-safe oxygen supply
Only MRI-conditional (non-ferromagnetic, e.g. aluminium) oxygen cylinders or the room's MR-safe piped oxygen may be used inside Zone IV; a standard steel cylinder is ferromagnetic and can be hurled into the magnet as a lethal projectile, regardless of where it is placed in the room. Withholding needed oxygen is unsafe for the patient. Respecting the MR-conditional-equipment rule is exactly the MRI-room precaution RD4.2 requires.
Applied Practice — Transport Scenario and Handover
Putting the principles, checklist and MRI precautions together, consider a worked transfer and the structured handover that completes it, because a safe journey ends not when the trolley arrives but when the patient is safely received and care is continuous. Deterioration en route must be anticipated with a contingency plan: the escort should know, before leaving, what they will do if the patient desaturates, becomes hypotensive, or arrests in a corridor or a scanner where help is not immediate.
Worked scenario — ventilated head-injury patient to CT. Justify (CT will determine neurosurgical management; no bedside alternative). Stabilise (sedation and ventilation optimised, blood pressure supported). Run the checklist: secured tube and capnography, oxygen reserve calculated for the round trip plus a margin and confirmed adequate (spare cylinder taken), charged transport monitor and infusion pumps, emergency drugs packed, doctor-plus-nurse escort, radiology informed. Plan the route and lift. During the scan the escort stays with the patient, monitoring continuously, ready to manage deterioration.
If the destination were MRI instead of CT, the additional precautions apply: screen the patient and all staff for implants and ferromagnetic foreign bodies, swap to MRI-conditional oxygen cylinder, monitor, ventilator and pumps, and never bring standard steel equipment past the Zone III/IV boundary. If the patient arrests in the magnet room, remove them from Zone IV before resuscitating.
Structured handover on arrival and return, using an SBAR-style format:
- Situation: who the patient is and current status.
- Background: diagnosis, relevant history, current support (ventilation, infusions).
- Assessment: stability, any events during transport.
- Recommendation/Request: ongoing needs, monitoring, and the plan for the return journey.
The transfer is complete only when the patient is back under full unit support with monitoring uninterrupted, the journey and any events documented, and a clear plan handed over — the same closed-loop discipline that governs the requisition applies to the transport.
CLINICAL PEARL
Pearl 1 — Calculate the oxygen, never guess it. Estimate cylinder contents (gauge pressure x water capacity) and divide by the fresh-gas flow to get usable minutes; confirm it exceeds the round-trip time PLUS a delay margin, and take a spare. Running out of oxygen in a corridor is a preventable arrest.
Pearl 2 — The MRI magnet is always on. It does not switch off between scans. Any ferromagnetic object — a steel cylinder, scissors, a standard monitor — becomes a projectile near the bore. Only MRI-conditional equipment crosses into Zone IV, and only after screening.
Pearl 3 — The safest transfer may be the one you don't do. Before moving a critically ill patient, ask whether a bedside chest X-ray or bedside ultrasound could answer the question without leaving the unit.
Pearl 4 — Resuscitate OUTSIDE the magnet. If a patient arrests in Zone IV, remove them from the magnet room first — standard resuscitation and defibrillation equipment is MRI-unsafe and cannot safely be used inside.
Self-Assessment — Transport Safety and the MRI Room
Use these scenarios to test your grasp of transport safety and MRI-room precautions. Write your answer before reading the discussion.
Scenario A: A junior doctor is asked to take a ventilated patient to CT alone, pushing the trolley while bagging the patient by hand, with a monitor that has 10% battery. Identify the safety failures and state what should happen instead.
Discussion: Failures: inadequate escort (one person cannot safely push, ventilate, and respond to deterioration — a ventilated patient needs a trained escort of at least a doctor plus an assistant); a transport monitor at 10% battery may die mid-journey; hand-bagging without confirmed oxygen reserve risks running out; no mention of a calculated oxygen supply or emergency drugs. Instead: a charged monitor, a calculated and adequate (plus spare) oxygen supply, secured ventilation, emergency drugs, and an appropriately staffed escort, with radiology informed — i.e. the full pre-transport checklist completed before departure.
Scenario B: During an MRI, a patient with an unscreened history is found afterwards to have had a cardiac pacemaker, and separately a porter nearly wheeled a steel wheelchair into the magnet room. What systemic precautions should have prevented both events?
Discussion: Both are zoning/screening failures. Every patient and accompanying person must be screened for implants and ferromagnetic objects in Zone II before entering, which would have identified the pacemaker (a potential MRI contraindication requiring device-specific assessment). The Zone III/IV access control and ferromagnetic screening should have stopped the steel wheelchair at the boundary; only MRI-conditional equipment crosses into Zone IV. Strict zoning plus screening of people and equipment is the system that prevents both the implant hazard and the projectile hazard.
Scenario C: Halfway to CT, a ventilated patient's SpO2 falls to 82% and capnography flattens. What is your structured response, and how does pre-transport preparation help?
Discussion: Treat it as a potential airway/oxygen problem: check the circuit and tube (disconnection, displacement), confirm oxygen is still flowing and the cylinder has not emptied, hand-ventilate with the self-inflating bag if needed, and call for help while continuing toward a safe area. Pre-transport preparation makes this manageable: a calculated oxygen reserve (so the cylinder has not run dry), a self-inflating bag and airway rescue kit packed, capnography running to detect the problem early, and a competent escort able to act. Anticipation, not improvisation, is what keeps a corridor desaturation from becoming an arrest.