Page 4 of 17
RD5.2 | Age Estimation Using X-ray Reference Standards — SDL Guide
Learning Objectives
- Explain when radiographic age estimation is clinically and medico-legally indicated.
- Distinguish bone (skeletal) age from chronological age and explain why reference standards are population-dependent.
- Describe the method of each major approach — ossification-centre appearance, hand–wrist atlases (Greulich-Pyle, Tanner-Whitehouse) and epiphyseal-fusion sequence.
- Select the appropriate reference standard and region to image for a given subject's likely age band and purpose.
- Interpret skeletal maturity into a defensible age RANGE with stated limitations, using Indian reference values where appropriate.
INSTRUCTIONS
Estimating a person's age from a radiograph is a skill that sits at the intersection of radiology, paediatrics and forensic medicine. It is requested when a documented age is unavailable or disputed — for legal proceedings, for verifying eligibility, or to evaluate a child whose growth seems out of step with their stated age. The core competency RD5.2 is deliberately worded around 'selecting and using appropriate reference standards', because the central skill is not memorising a single number but choosing the right method for the subject's age band and population, and then reporting an honest age range rather than a false-precision point estimate. This module builds that judgement: it explains skeletal maturation, walks through each reference method, and stresses the population-bias and confidence-interval caveats that separate a defensible estimate from a dangerous one.
References
- Sutton's Textbook of Radiology and Imaging, 7th edition, Skeletal Maturation and Bone Age (textbook)
- Grainger & Allison's Diagnostic Radiology, 7th edition, Skeletal Development and Age Assessment (textbook)
- The Essentials of Forensic Medicine and Toxicology (Reddy's), Age Estimation — Indian reference values for ossification and epiphyseal fusion (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 16-year-old boy is brought to a government hospital by the police. He is accused in a criminal matter, but he has no birth certificate and his apparent age is disputed — if he is below 18 he must be dealt with under the juvenile justice framework, not as an adult. The investigating officer asks for a radiological age estimation. The casualty medical officer's first instinct is to order 'an X-ray to find his age,' but which X-ray, matched against which standard? A single hand–wrist film read against an atlas, the fusion status of late-fusing epiphyses such as the iliac crest and medial clavicle, or both? And crucially: can the report state '16 years' as a fact, or must it state a RANGE with a margin of error? The boy's legal status — and the integrity of the medico-legal opinion — depend on the doctor selecting the appropriate reference standard and reporting the estimate honestly. Age estimation is never a single magic number; it is the disciplined matching of skeletal maturity to the right reference, reported with its limits.
WHY THIS MATTERS
Radiographic age estimation is one of the few imaging tasks an MBBS graduate may be asked to perform or interpret in a medico-legal capacity, and errors carry real consequences — wrongful treatment of a juvenile as an adult, or vice versa, and challenges to expert opinion in court. The NMC competency RD5.2 specifically frames the skill as 'age estimation from X-rays by selecting and using appropriate reference standards,' signalling that the examinable and clinically defensible core is the SELECTION of the right standard, not rote recall of a single fusion age. Beyond the forensic setting, the same skeletal-maturity reading underpins paediatric practice: a bone age that lags or leads chronological age is a key clue in short stature, constitutional delay, precocious puberty and endocrine disorders, and it guides decisions such as growth-hormone therapy and the timing of orthopaedic intervention. Because the request usually justifies only a low-dose film (often a single hand–wrist radiograph), ALARA is satisfied, but the interpretive responsibility — choosing the standard, applying it correctly and reporting a range — falls on the clinician. This makes age estimation a compact, high-stakes example of disciplined, standard-anchored interpretation.
RECALL
Before reading further, recall the developmental and normal-radiograph foundations this skill builds on:
- Skeletal development (AN/PY, and RD5.1): long bones develop from a primary ossification centre (the shaft, present at birth) and secondary ossification centres (the epiphyses, appearing postnatally at predictable ages); growth occurs at the cartilaginous physis (growth plate), which eventually ossifies and fuses.
- The normal paediatric film (RD5.1): the radiolucent growth plate and the separate ossified epiphysis are NORMAL findings; their appearance and disappearance (fusion) over time is exactly what age estimation exploits.
- Bone age concept: skeletal maturity advances in a broadly orderly sequence that correlates with — but is not identical to — chronological age; the gap between them is informative in disease.
- Forensic context (FM): Indian medico-legal practice uses Indian reference values for fusion and ossification because Western atlas data can misestimate in Indian populations; corroborative markers (dental, clavicular) strengthen an opinion.
If the sequence of ossification and fusion is unclear, a quick review of skeletal development now will make the reference-standard methods below much easier to apply.
Why Radiographic Age Estimation Matters and When It Is Requested
Radiographic age estimation is requested whenever a person's age must be inferred from the body because documentary evidence is absent, unreliable or disputed, and the answer carries weight. Understanding WHEN it is indicated is the first part of the skill, because the indication shapes which method and which region to image. There are three broad contexts. The first is medico-legal age determination: in criminal justice (e.g. distinguishing a juvenile from an adult under the Juvenile Justice framework), in suspected child marriage or trafficking, in employment or sporting-eligibility disputes, and in immigration. Here the request typically comes from a legal authority, the opinion must be defensible in court, and the result must be reported as a range with a stated margin of error. The second is clinical paediatric assessment: a 'bone age' is requested to evaluate a child whose growth is abnormal — short stature, suspected constitutional growth delay, precocious or delayed puberty, and endocrine disorders — where the gap between skeletal and chronological age guides diagnosis and the timing of treatment. The third is research and population studies of growth and maturation.
The indication determines the imaging strategy and standard:
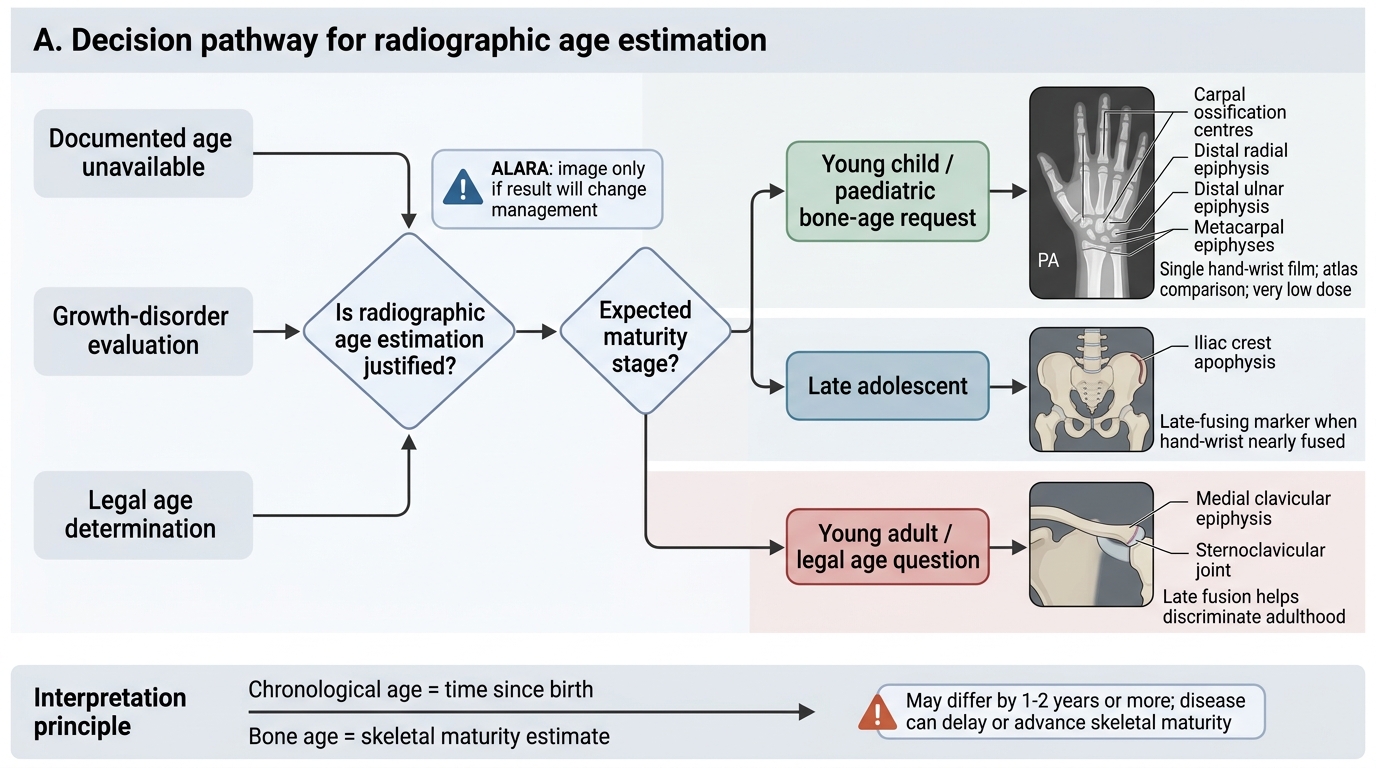
Radiographic Age Estimation Decision Pathway
- For young children and most paediatric bone-age requests, a single hand–wrist film read against an atlas is the workhorse — it samples many ossification centres in one low-dose image.
- For late adolescents and young adults in whom the hand–wrist centres have already fused, late-fusing epiphyses (iliac crest, medial clavicle) become the discriminating markers.
- Throughout, ALARA applies: the dose must be justified, which is why a single hand–wrist film (very low dose) is preferred wherever it answers the question.
Governing Principles — Bone Age vs Chronological Age and the Logic of Reference Standards
Two governing principles make age estimation defensible, and confusing either is the commonest source of error. The first is the distinction between bone (skeletal) age and chronological age. Skeletal maturity — the appearance of ossification centres and the progressive fusion of epiphyses — advances in a broadly orderly biological sequence. Bone age is an estimate of that maturity expressed in years; chronological age is the actual time elapsed since birth. In a healthy child the two are close, but they can diverge by 1–2 years or more in normal variation, and far more in disease: bone age LAGS chronological age in constitutional growth delay, hypothyroidism and chronic illness, and LEADS it in precocious puberty and some endocrine disorders. The clinical value in paediatrics comes precisely from this gap; the forensic risk comes from forgetting that bone age is an estimate of maturity, not a direct readout of calendar age.
The second principle is why the standard must be selected appropriately rather than applied blindly. Every reference standard was built from a particular population at a particular time, and maturation differs by sex (girls mature skeletally ahead of boys), by population/ethnicity and nutrition, and by secular trend (children mature earlier in better-nourished cohorts).
Provided image
- The widely used Greulich-Pyle (GP) atlas was derived from a 20th-century North American cohort (predominantly white, higher socioeconomic status). Applying it uncritically to a different population can systematically over- or under-estimate age — a recognised bias and the reason the competency stresses 'appropriate' standards.
- In Indian medico-legal practice, Indian reference values for ossification and epiphyseal fusion (per Reddy's) are preferred over Western atlas values, because the latter can misestimate in Indian children.
- A sound estimate always uses a SEX-appropriate standard and, where possible, a population-appropriate one, and corroborates across more than one marker.
SELF-CHECK
A paediatrician requests a 'bone age' on a 7-year-old girl with short stature. The hand–wrist film is read against the Greulich-Pyle atlas and reported as a bone age of 5 years. What is the most accurate interpretation?
A. The child's true chronological age is 5 years; the parents are mistaken
B. Skeletal maturity lags chronological age by about 2 years, which can occur in constitutional growth delay, hypothyroidism or chronic illness and warrants evaluation
C. Bone age and chronological age are always identical, so the film must be technically inadequate
D. The Greulich-Pyle atlas cannot be used in girls
Reveal Answer
Answer: B. Skeletal maturity lags chronological age by about 2 years, which can occur in constitutional growth delay, hypothyroidism or chronic illness and warrants evaluation
Bone age estimates skeletal MATURITY, not chronological age. A bone age lagging chronological age by ~2 years indicates delayed skeletal maturation, seen in constitutional growth delay, hypothyroidism and chronic illness — it is a diagnostic clue, not proof of the child's calendar age. Bone and chronological age are not always identical even in health. The Greulich-Pyle atlas has sex-specific reference plates and is used in both sexes.
Method — Ossification Centres, Hand–Wrist Atlases and Fusion Sequences
There are three complementary methods, and the central skill is matching the method to the subject's likely age band rather than applying one technique to everyone. Each method reads a different phase of the same underlying maturation process — the appearance of ossification centres in the youngest children, atlas-matched overall maturity through childhood and adolescence, and the orderly fusion of epiphyses in late adolescence and early adulthood. The hand and wrist are the preferred single region for paediatric assessment because a single low-dose film samples many ossification centres and epiphyses simultaneously, satisfying ALARA while giving a rich maturity picture. As the subject grows older and those hand–wrist centres fuse, the informative signal moves to later-fusing sites elsewhere in the skeleton, which is why no single film or method spans the whole age range. Keep this age-band logic in mind as each method is described below.
Provided image
Provided image
1. Appearance of ossification centres (infancy–early childhood). Primary centres (shafts) are present at birth; secondary centres (epiphyses and the carpal/tarsal bones) appear postnatally in a predictable order and at predictable ages. Reading WHICH centres have appeared estimates age in the youngest children, before atlas matching is informative.
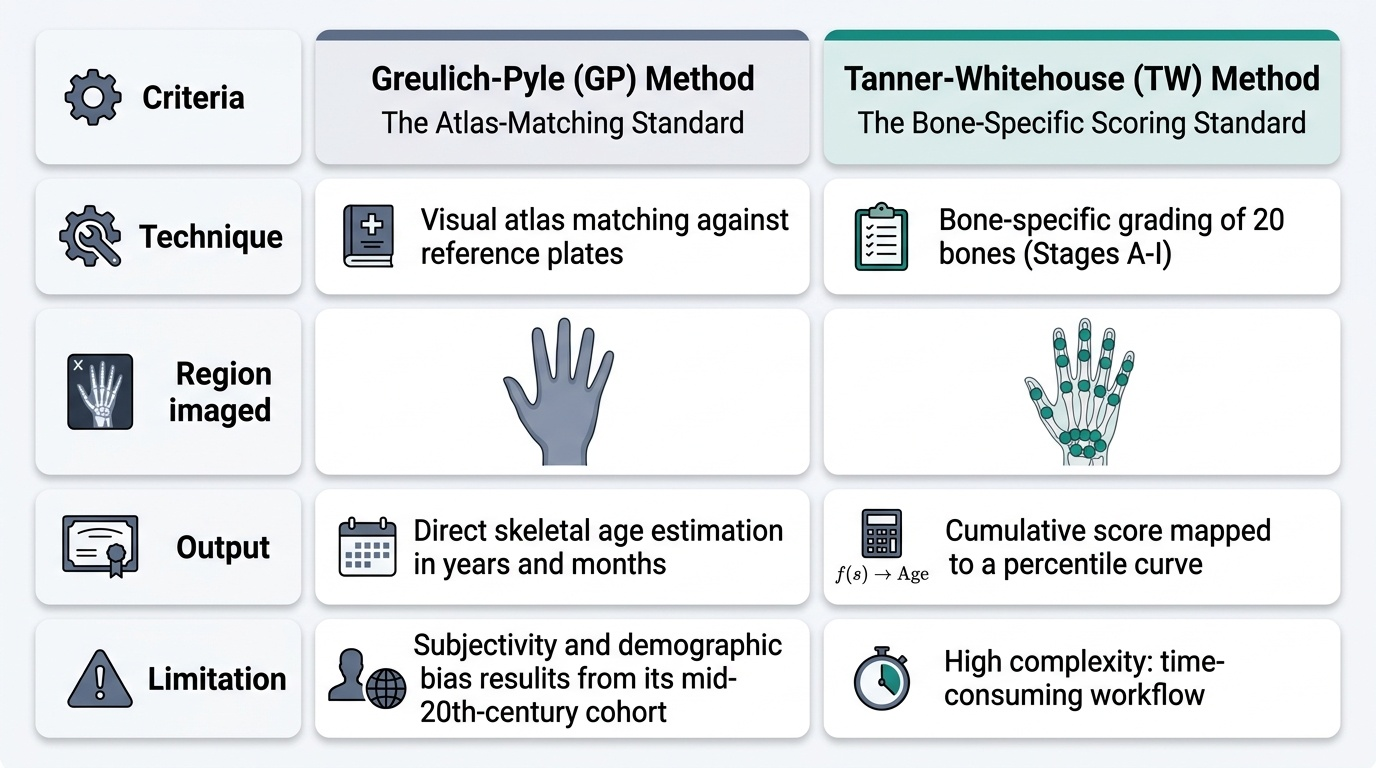
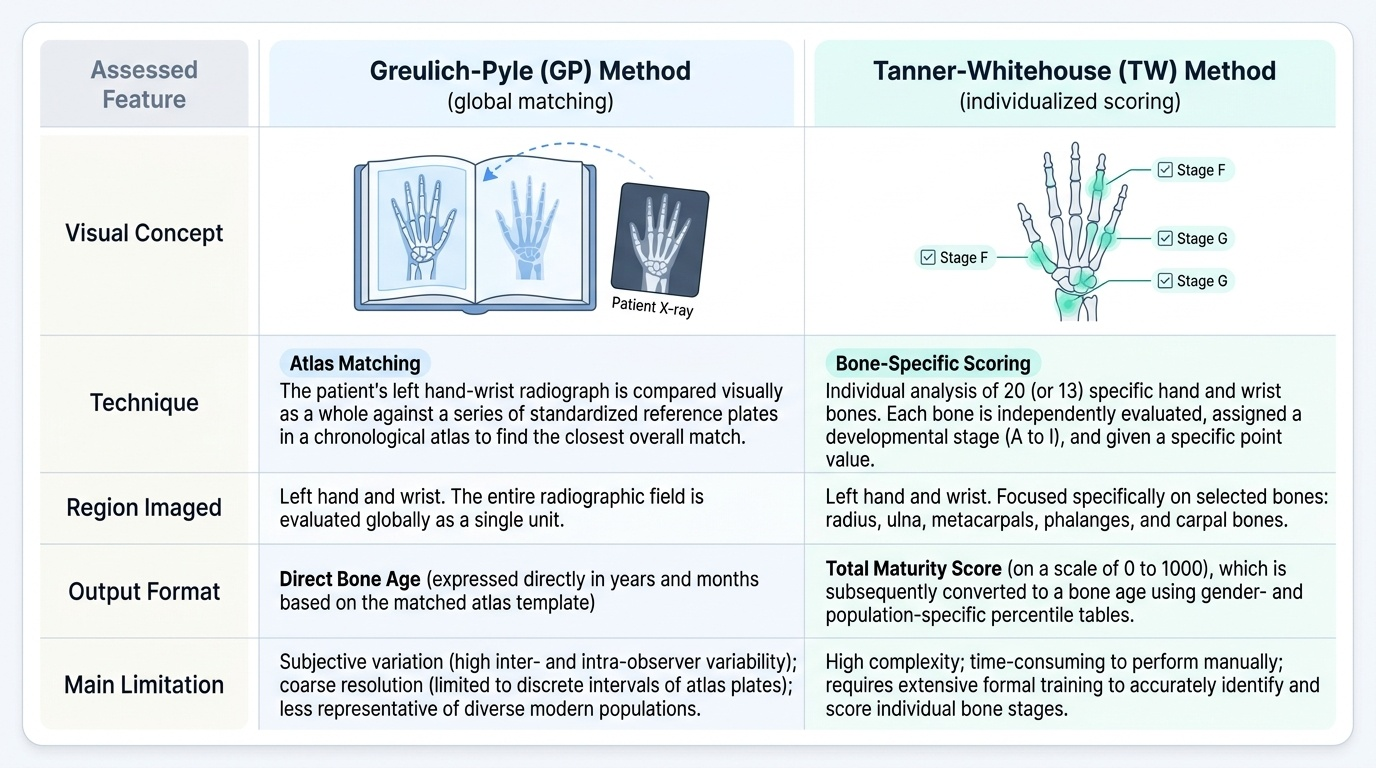
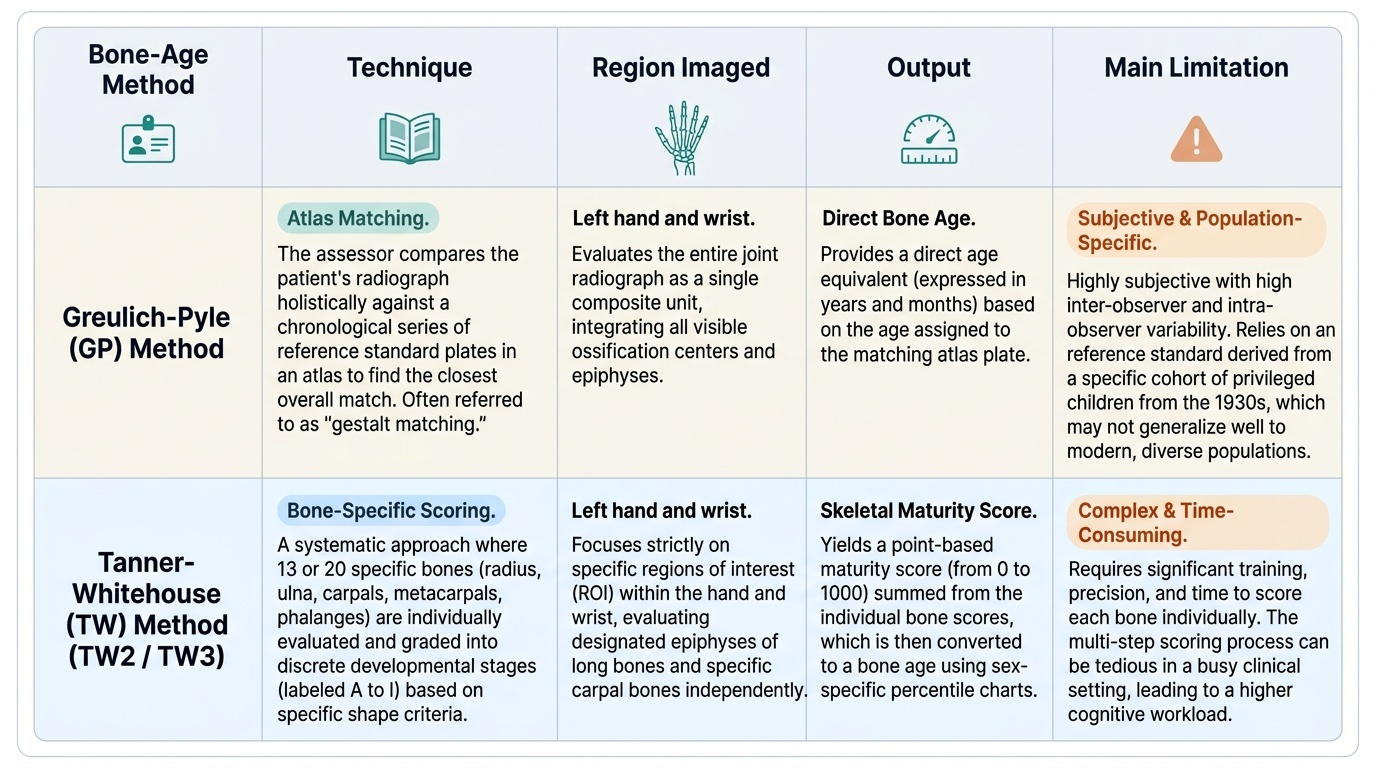
2. Hand–wrist atlas methods (childhood–adolescence). Two approaches are standard:
- Greulich-Pyle (GP) — atlas MATCHING: the subject's single hand–wrist film is compared as a whole against a series of sex-specific reference plates, and the closest-matching plate gives the bone age. It is fast but observer-dependent and carries the population bias noted above.
- Tanner-Whitehouse (TW2/TW3) — bone-specific SCORING: each of a defined set of hand–wrist bones is assigned a maturity stage, the stages are summed into a maturity score, and the score is converted to a bone age. It is more reproducible and granular but slower.
3. Epiphyseal fusion sequence (adolescence–early adulthood). As maturity advances, epiphyses fuse to their metaphyses in an orderly sequence. Once the hand–wrist centres have largely fused (limiting atlas methods), LATE-fusing sites are imaged: the iliac crest apophysis (Risser sign, used in scoliosis) fuses around the early twenties, and the medial (sternal) end of the clavicle fuses LATEST of all (well into the early-to-mid twenties), making it the key marker for distinguishing a late adolescent from an adult. Per Reddy's Indian reference values, the iliac crest apophysis fuses at approximately 20–21 years and the medial clavicular epiphysis around 18–25 years; these Indian figures, not Western atlas values, are used in Indian medico-legal opinions.