Page 5 of 17
RD5.2 | Age Estimation Using X-ray Reference Standards — SDL Guide (Part 2)
Interpretation of Findings — Converting Skeletal Maturity into an Age Estimate with Limits
Interpreting skeletal maturity into an age estimate is where honesty about uncertainty separates a defensible opinion from a dangerous one. The cardinal rule is that the output is an age RANGE with a stated margin, never a single false-precision number. The width of that range depends on the method, the age band and individual biological variation, and a competent report states it explicitly (for example, 'the skeletal findings are consistent with an age of approximately X to Y years'). Three interpretive disciplines govern the conversion. First, choose a SEX-appropriate (and where possible population-appropriate) standard, because girls mature ahead of boys and the wrong-sex plate biases the estimate. Second, where the subject's age band straddles the limits of a method (very young, or after hand–wrist fusion), switch to the appropriate marker — ossification-centre appearance at the bottom and late-fusing epiphyses at the top — rather than forcing an out-of-range method. Third, corroborate: agreement across more than one marker (and dental findings in the forensic setting) tightens the estimate and strengthens the opinion.
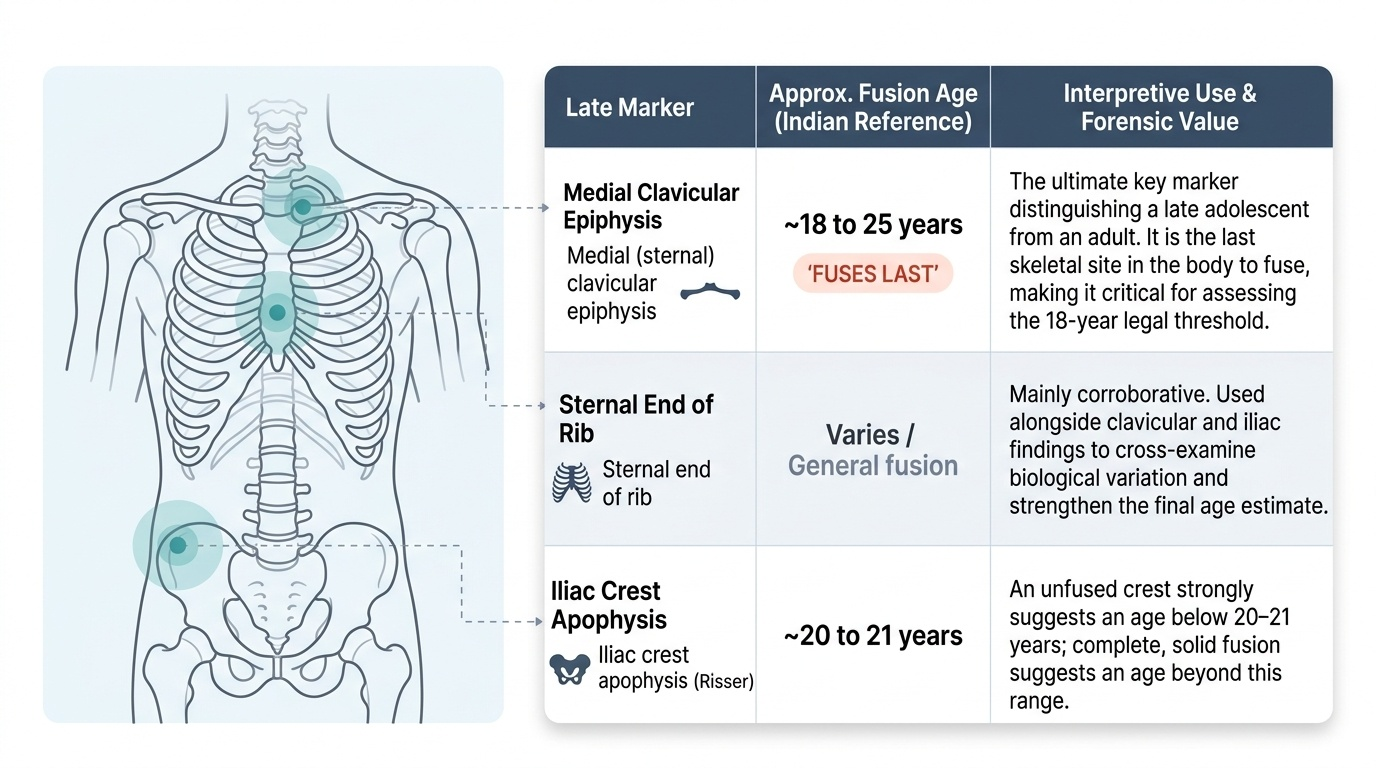
The scenario that most often confuses learners is the late adolescent whose hand–wrist plates have ALREADY fused — the atlas can no longer discriminate, so the estimate must come from the late-fusing sites:
Provided image
| Late marker | Approx. fusion age (Indian reference, per Reddy's) | Interpretive use |
|---|---|---|
| Iliac crest apophysis (Risser) | ~20–21 years | An unfused crest suggests age below ~20–21; complete fusion suggests beyond it |
| Medial (sternal) clavicular epiphysis | ~18–25 years (fuses LAST) | The key marker distinguishing a late adolescent from an adult; the last to fuse |
| Sternal end of rib / general fusion | varies | Corroborative, used alongside the above |
The interpretive limits to state in every report are: the population-bias of Western atlases (use Indian values for Indian subjects); the divergence of bone age from chronological age in disease and normal variation; the loss of discrimination at the extremes; and the resulting necessity of reporting a range, not a point. An estimate offered as a single exact year is, by itself, a red flag for an unsound interpretation.
Applied Practice — Selecting and Using the Appropriate Standard in a Worked Case
Applied practice means walking a real request from its indication through to a reported age range, choosing the standard deliberately at each step rather than reflexively ordering 'an X-ray for age.' The selection logic follows the subject's likely age band, because each method has an effective window: ossification-centre appearance informs the very young, hand–wrist atlases inform children and adolescents, and late-fusing epiphyses inform the late adolescent and young adult once the wrist has fused. At every step the clinician also fixes the sex-appropriate and population-appropriate standard (Indian reference values in the Indian medico-legal context) and commits in advance to reporting a range with a margin of error. Holding all of this together — indication, age band, correct standard, honest range — is the applied skill the competency is testing. Work through the decision pathway and the three worked cases below as you would for a real referral.
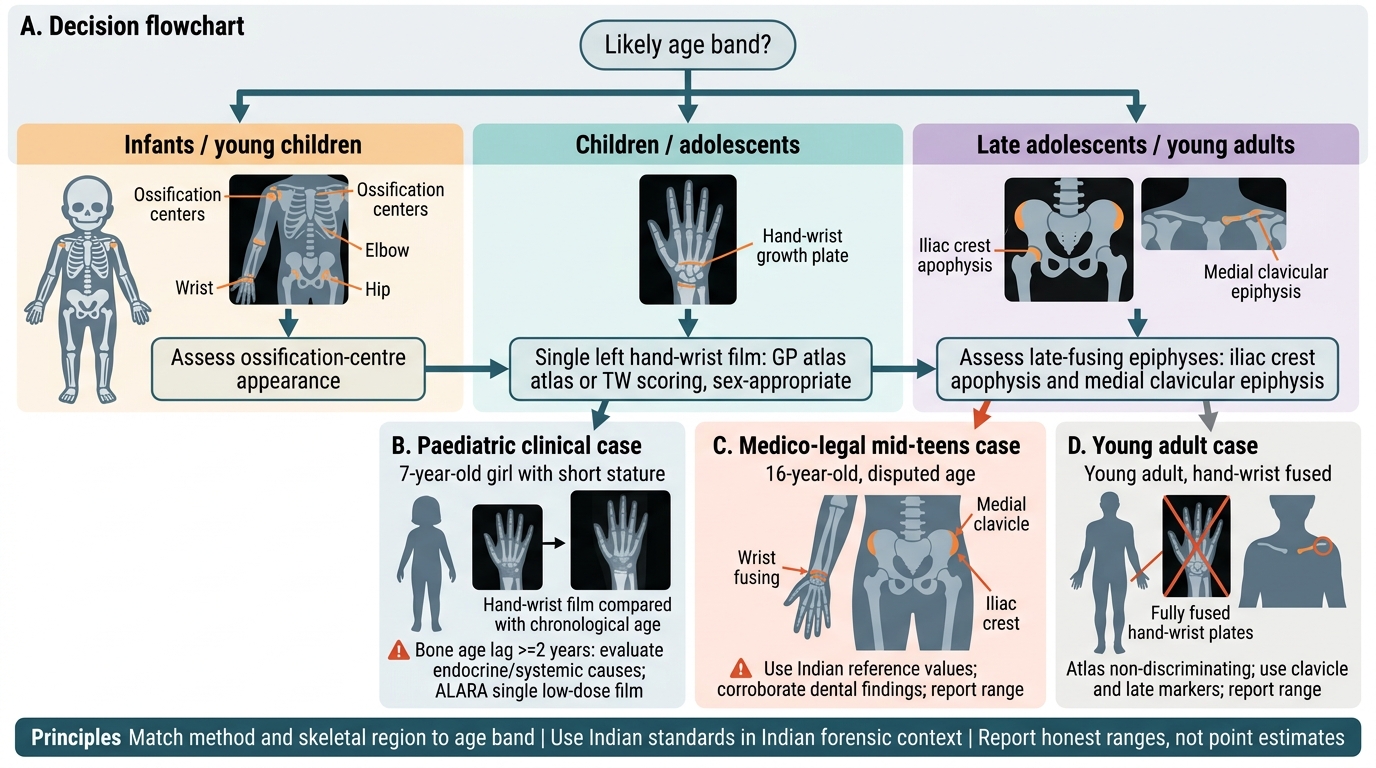
Radiological Age Estimation: Choosing the Correct Method
Worked case 1 — paediatric clinical (short stature). A 7-year-old girl with short stature: the appropriate standard is a single hand–wrist film read against a SEX-appropriate atlas (GP) or scored by TW. Report the bone age and compare it with chronological age; a lag of ≥2 years prompts endocrine/systemic evaluation. The low-dose single film satisfies ALARA.
Worked case 2 — medico-legal, mid-teens. The 16-year-old of the hook, with a disputed age around the juvenile/adult boundary: a hand–wrist film alone may be ambiguous if the wrist is fusing, so image the LATE-fusing sites — the iliac crest apophysis and the medial clavicular epiphysis — using INDIAN reference values, and corroborate with dental findings. Report the estimate as a RANGE with its margin of error, and state the standard used.
Worked case 3 — young adult. A subject whose hand–wrist plates are fully fused: the atlas is non-discriminating; rely on the medial clavicular epiphysis (the last to fuse) and other late markers, and report a range. The key applied skill across all three is choosing the standard and region to match the age band, using Indian values in the Indian forensic context, and never reporting a point estimate where a range is honest. A common applied error to avoid is forcing a hand–wrist atlas onto a subject whose wrist has already fused — at that point the atlas gives no information and the late markers must be used instead.
SELF-CHECK
A medico-legal age estimation is requested on a young man in India whose hand and wrist radiograph shows that all the distal radial and ulnar epiphyses are already fully fused. Which approach is most appropriate?
A. Report his age as exactly 19 years based on the fused wrist
B. Image late-fusing sites such as the medial clavicular epiphysis and iliac crest, use Indian reference values, and report an age range
C. Repeat the hand–wrist film with the Greulich-Pyle atlas to get a precise bone age
D. Conclude that age cannot be estimated once the wrist is fused
Reveal Answer
Answer: B. Image late-fusing sites such as the medial clavicular epiphysis and iliac crest, use Indian reference values, and report an age range
Once the hand–wrist epiphyses are fused, the atlas methods can no longer discriminate, so the estimate must come from LATE-fusing sites — the medial (sternal) clavicular epiphysis (the last to fuse, ~18–25 years) and the iliac crest apophysis (~20–21 years) — using Indian reference values in the Indian medico-legal context. The result must be reported as a RANGE, not an exact year. Re-doing the hand–wrist atlas adds nothing once those plates have fused, and age can still be estimated using the appropriate late markers.
SELF-CHECK
Which statement best explains why the Greulich-Pyle atlas should be applied with caution when estimating the age of an Indian child?
A. The atlas only works for fractures, not for age estimation
B. The atlas was derived from a 20th-century North American cohort, so population, nutritional and secular differences can bias the estimate in other populations
C. The atlas cannot be used in children under 10 years
D. The atlas gives chronological age directly with no margin of error
Reveal Answer
Answer: B. The atlas was derived from a 20th-century North American cohort, so population, nutritional and secular differences can bias the estimate in other populations
The Greulich-Pyle atlas was built from a 20th-century North American (predominantly white, higher socioeconomic) population. Skeletal maturation differs with population/ethnicity, nutrition and secular trend, so applying GP uncritically to a different population can systematically over- or under-estimate age. This is why the competency stresses selecting an APPROPRIATE standard and why Indian reference values are preferred for Indian subjects. The atlas estimates skeletal maturity (a range), not chronological age directly.
CLINICAL PEARL
Pearl 1 — Bone age is maturity, not calendar age. Always report a RANGE, and remember bone age can lag (constitutional delay, hypothyroidism, chronic illness) or lead (precocious puberty) chronological age. A single exact year is a red flag for an unsound opinion.
Pearl 2 — Match the method to the age band. Ossification-centre appearance for the very young; hand–wrist atlas (GP or TW) for children/adolescents; late-fusing epiphyses (medial clavicle last of all, iliac crest) once the wrist has fused. Do not force a hand–wrist atlas onto a subject whose wrist is already fused.
Pearl 3 — Use the appropriate population standard. In Indian medico-legal practice use INDIAN reference values (Reddy's), not the Western Greulich-Pyle atlas, because the latter can misestimate in Indian children. Corroborate across markers and, in forensic work, with dental findings.
Self-Assessment — Reference-Standard Selection and Reporting
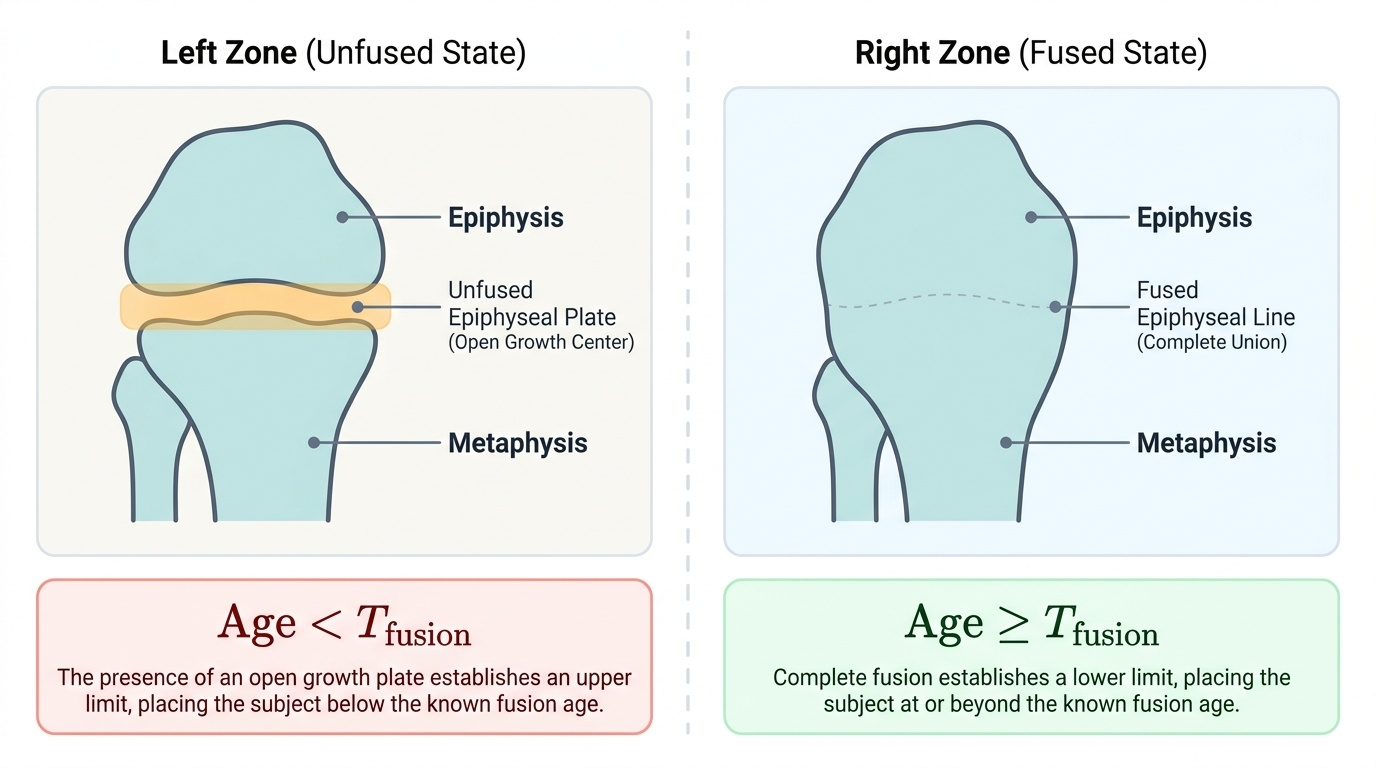
Use these scenarios to test your reference-standard selection and your discipline in reporting an honest age range. Each one turns on the same recurring decisions: which method suits the subject's age band, which sex- and population-appropriate standard applies, what to do when the hand–wrist plates have already fused, and how the gap between bone age and chronological age should be interpreted clinically. Decide your answer for each before reading the discussion, exactly as you would when a court or a paediatrician puts the request in front of you, and notice in particular how fusion status itself narrows an estimate. The accompanying figure contrasts an unfused with a fused epiphysis to make that point concrete, since an unfused growth centre places the subject below its fusion age while a fully fused one places them beyond it.
Provided image
Scenario A: A court requests age estimation on a girl who appears to be in early adolescence. Which standard and region do you choose, and how do you report?
Discussion: For an early adolescent, a hand–wrist radiograph read against a SEX-appropriate standard is the workhorse — girls mature ahead of boys, so the female reference must be used. In the Indian context, prefer Indian reference values; corroborate with another marker if the result is near a legally important boundary. Report as a range with a stated margin, not an exact age, and name the standard used.
Scenario B: A radiographer hands you a hand–wrist film on a subject whose wrist epiphyses are clearly all fused, and asks for the bone age 'from the atlas.' What is your response?
Discussion: Explain that once the hand–wrist epiphyses are fused the atlas methods have reached their ceiling and give no further discrimination. The estimate must come from LATE-fusing sites — the medial clavicular epiphysis (the last to fuse) and the iliac crest apophysis — using Indian reference values, and the result reported as a range. Forcing the atlas here would produce a false-precision answer.
Scenario C: A bone age in an 8-year-old boy reads 11 years. What does this suggest, and what would you advise?
Discussion: A bone age LEADING chronological age by ~3 years suggests advanced skeletal maturation — seen in precocious puberty and some endocrine/adrenal disorders. This is a clinical clue, not a statement that the child is 11; advise paediatric/endocrine evaluation. The case illustrates the core principle that bone age estimates maturity and its divergence from chronological age is diagnostically meaningful.