Page 4 of 17
RD7.3 | Imaging in Pulmonary Embolism — SDL Guide
Learning Objectives
- Recognise the clinical presentations of suspected pulmonary embolism and use a validated pre-test probability score (Wells / revised Geneva) with D-dimer to decide who needs imaging.
- Justify CT pulmonary angiography (CTPA) as the first-line imaging modality of choice, and identify the situations in which a ventilation-perfusion (V/Q) scan is preferred.
- Describe the expected imaging findings of pulmonary embolism on CTPA, V/Q scintigraphy, chest radiograph and echocardiography.
- Integrate the imaging result with right-ventricular strain assessment to risk-stratify the patient and select anticoagulation, thrombolysis, or safe exclusion.
- Apply the imaging pathway to special populations including contrast allergy, renal impairment, pregnancy and the haemodynamically unstable patient.
INSTRUCTIONS
Pulmonary embolism (PE) is common, frequently missed, and potentially fatal — yet it is eminently treatable once diagnosed. The clinical signs are non-specific, so the diagnosis rests on a disciplined sequence of pre-test probability scoring, D-dimer testing and definitive imaging. As a final-year student and future clinician, you will repeatedly face the question 'could this breathlessness be a PE?'. This module teaches you how to move from suspicion to a safe, evidence-based imaging decision, how to read the key imaging findings, and how those findings drive treatment — the applied core of competency RD7.3.
References
- Sutton's Textbook of Radiology, 6th edition, Chapter on Cardiothoracic Imaging (textbook)
- Grainger & Allison's Diagnostic Radiology, 6th edition, Chapter on Pulmonary Vascular Disease and Pulmonary Embolism (textbook)
- ESC 2019 Guidelines for the Diagnosis and Management of Acute Pulmonary Embolism (guideline)
- PIOPED II (Stein PD et al, NEJM 2006); Christopher Study (JAMA 2006); ADJUST-PE age-adjusted D-dimer (Righini M et al, JAMA 2014) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 54-year-old woman returns from a long-haul flight and develops sudden pleuritic chest pain and breathlessness. Her oxygen saturation is 92% on room air, her heart rate is 110, and her chest radiograph is reported as 'essentially normal'. The casualty officer is reassured by the normal chest X-ray and is about to send her home. This is exactly how a fatal pulmonary embolism is missed. The chest radiograph in PE is usually normal or shows only subtle, non-specific changes — its main value is to exclude an alternative diagnosis such as pneumonia or pneumothorax, not to confirm or refute PE. The decision that actually matters is whether to order a CT pulmonary angiogram, and that decision is governed not by the chest X-ray but by a structured assessment of pre-test probability and a D-dimer. Getting that sequence right is what separates a safe discharge from a preventable death.
WHY THIS MATTERS
Pulmonary embolism is one of the most common preventable causes of in-hospital death, and venous thromboembolism (the combined burden of deep vein thrombosis and PE) affects surgical patients, pregnant women, cancer patients and immobilised medical patients alike. Because its symptoms — breathlessness, pleuritic pain, tachycardia, syncope — overlap with so many other conditions, PE is both over-investigated (exposing low-risk patients to unnecessary radiation and contrast) and under-diagnosed (missed in patients whose presentation was atypical). The NMC competency RD7.3 requires you to integrate imaging findings into the management of PE in the internal medicine setting. This is a daily, practical skill: every medical admission unit, every post-operative ward and every antenatal assessment will at some point ask you to reason through 'is this a PE, and how do I prove or exclude it safely?'. Knowing which test to order, when, and why is core clinical competence.
RECALL
Before reading further, recall the following foundations from your earlier years:
- Virchow's triad (from pathology): venous thrombosis arises from the interaction of venous stasis, endothelial injury, and hypercoagulability. Most pulmonary emboli are thrombi that have detached from a deep vein thrombosis (DVT) in the legs or pelvis and lodged in the pulmonary arteries — PE and DVT are two ends of one disease, venous thromboembolism (VTE).
- Pulmonary circulation (from physiology): the entire cardiac output passes through the low-pressure, low-resistance pulmonary vascular bed. A large embolus acutely obstructs this bed, raising right-ventricular afterload — the mechanism of right-heart strain and obstructive shock in massive PE.
- Dead-space ventilation (from physiology): an embolised lung segment is ventilated but not perfused, creating alveolar dead space — this physiological mismatch is exactly what a ventilation-perfusion (V/Q) scan is designed to detect.
- D-dimer: a degradation product of cross-linked fibrin; it rises whenever there is active clot formation and breakdown. It is sensitive but not specific — a normal D-dimer helps to exclude VTE in low-probability patients, but a raised D-dimer occurs in infection, malignancy, pregnancy, surgery and old age, so it can never confirm PE.
Clinical Scenario — When to Suspect PE and Who Needs Imaging
The first principle of imaging in pulmonary embolism is that imaging is never the starting point — it is the endpoint of a structured clinical assessment. Because the symptoms of PE are non-specific, simply scanning everyone with breathlessness would expose huge numbers of patients to unnecessary radiation and iodinated contrast while still missing atypical presentations. The internationally accepted approach is therefore to first estimate the pre-test (clinical) probability of PE using a validated scoring system, and only then to decide whether the patient needs a D-dimer, definitive imaging, or neither. This disciplined sequence — score, then D-dimer where appropriate, then image — is what makes the diagnostic pathway both safe and efficient, and it is precisely the reasoning that competency RD7.3 expects you to apply at the bedside before any scan is requested.
The clinical presentations that should raise suspicion of PE include:
- Acute breathlessness of unexplained or disproportionate degree, often of sudden onset.
- Pleuritic chest pain with or without haemoptysis (suggesting peripheral, often infarct-related, embolism).
- Tachycardia, tachypnoea and hypoxaemia without an obvious alternative cause.
- Syncope or haemodynamic instability/shock — these suggest a large, central (high-risk) PE causing acute right-ventricular failure.
- Unilateral leg swelling or pain indicating a coexisting DVT, the embolic source.
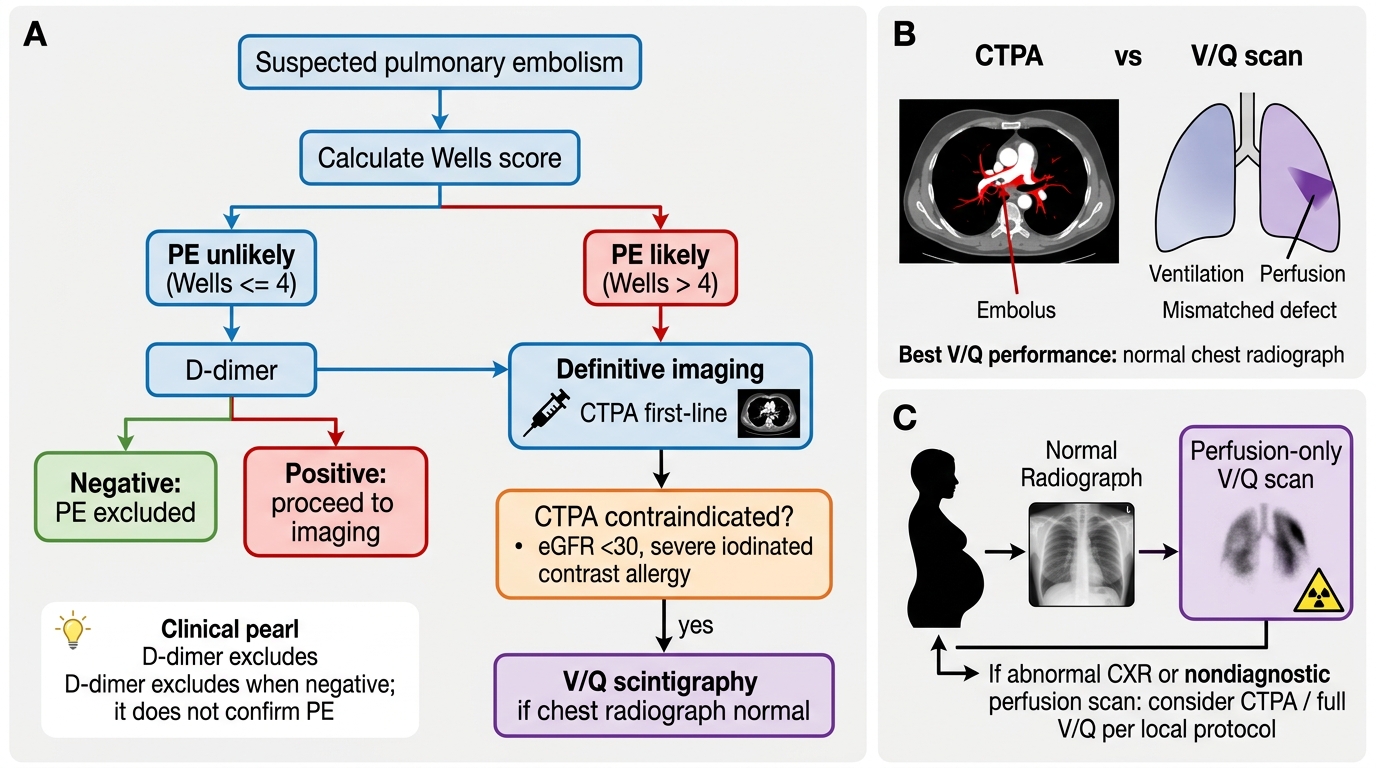
The pre-test probability is formalised using the Wells score (the most widely used) or the revised Geneva score. In the common two-tier Wells model, a score greater than 4 points classifies PE as 'likely' and the patient proceeds directly to CT pulmonary angiography; a score of 4 or fewer classifies PE as 'unlikely', and a D-dimer is performed first. A normal D-dimer in an 'unlikely' patient safely excludes PE without any imaging at all. In patients over 50 years, the age-adjusted D-dimer cut-off (age × 10 ng/mL, in fibrinogen-equivalent units) improves specificity and reduces unnecessary scans, as validated by the ADJUST-PE study. A raised D-dimer, or any 'likely' patient, proceeds to definitive imaging. This logic ensures that the patient who genuinely needs a scan gets one promptly, while the low-risk patient is spared it.
Imaging Strategy — CTPA First-Line, V/Q and Special Situations
Once the clinical pathway indicates that definitive imaging is required, the strategy is governed by a clear hierarchy in which one modality is first-line for almost every patient and a second exists specifically for those in whom the first is unsafe. Understanding why CT pulmonary angiography sits at the top of this hierarchy — and recognising the precise circumstances that displace it — is the heart of imaging strategy in PE. The choice is not arbitrary: it balances diagnostic accuracy, speed, availability, the ability to find alternative diagnoses, and patient-specific contraindications such as renal function, contrast allergy and pregnancy. Reasoning through this hierarchy, rather than reflexively ordering a single test, is what competency RD7.3 asks of the internal-medicine clinician.
CT pulmonary angiography (CTPA) — first-line, modality of choice:
CTPA acquires a contrast-enhanced CT of the pulmonary arteries during peak arterial opacification. It is fast (seconds of acquisition), almost universally available in emergency settings, and directly visualises the embolus as a filling defect within the contrast-filled vessel. In PIOPED II it demonstrated a sensitivity of approximately 83% and specificity of approximately 96%, and it has the major additional advantage of revealing alternative diagnoses (pneumonia, aortic dissection, pneumothorax, malignancy) when PE is absent. For these reasons it is the default investigation in the haemodynamically stable patient who needs imaging.
Ventilation-perfusion (V/Q) scintigraphy — the principal alternative:
V/Q scanning is chosen when CTPA is contraindicated. The two main triggers are iodinated contrast allergy and renal impairment, where contrast is generally avoided once the eGFR falls below 30 mL/min/1.73m². V/Q delivers no iodinated contrast and a lower radiation dose to the breast tissue. It performs best in patients with a normal baseline chest radiograph (a co-existing parenchymal abnormality degrades its specificity).
Pregnancy — a special pathway:
In pregnancy the imaging choice weighs fetal and maternal radiation dose. Both CTPA and V/Q are acceptable; many centres favour a perfusion-only (Q) scan in a woman with a normal chest radiograph because it delivers a lower breast radiation dose than CTPA while still detecting the perfusion defect. Bilateral lower-limb compression ultrasound is often performed first, because finding a DVT confirms VTE and may obviate chest imaging altogether.
Adjunct and bedside roles:
The chest radiograph is used chiefly to look for alternative diagnoses, not to confirm PE. Echocardiography is invaluable at the bedside in the unstable patient, where it can demonstrate acute right-ventricular strain and support immediate treatment when the patient is too unstable to travel to the CT scanner. Lower-limb compression ultrasonography detects the DVT source.
Imaging Pathway for Suspected Pulmonary Embolism
SELF-CHECK
A 68-year-old man with chronic kidney disease (eGFR 24 mL/min/1.73m²) presents with breathlessness and pleuritic chest pain. His Wells score classifies PE as 'likely'. A normal recent chest radiograph is available. Which is the most appropriate definitive imaging investigation?
A. CT pulmonary angiography, because it is always the first-line test regardless of renal function
B. Ventilation-perfusion (V/Q) scintigraphy, because iodinated contrast is best avoided at this eGFR and his chest radiograph is normal
C. D-dimer alone, because it can confirm the diagnosis non-invasively
D. No imaging; start anticoagulation empirically and review in 48 hours
Reveal Answer
Answer: B. Ventilation-perfusion (V/Q) scintigraphy, because iodinated contrast is best avoided at this eGFR and his chest radiograph is normal
CTPA is the first-line modality, but iodinated contrast is generally avoided when the eGFR is below 30 mL/min/1.73m² because of the risk of contrast-associated kidney injury. The principal alternative when CTPA is contraindicated is a V/Q scan, which uses no iodinated contrast and performs best when the baseline chest radiograph is normal — as it is here. A D-dimer is sensitive but non-specific and can never confirm PE. Empirical anticoagulation without confirming the diagnosis exposes the patient to bleeding risk and is not the correct pathway when safe imaging is available.
Imaging Findings — Recognising PE on CTPA and V/Q
Recognising the imaging signature of pulmonary embolism across the different modalities is a core interpretive skill, because the same disease produces characteristically different appearances depending on whether it is imaged by CT, by scintigraphy, by plain radiograph or by echocardiography. The unifying concept is that an embolus mechanically obstructs a pulmonary artery: on CTPA this is seen directly as a clot within the contrast column, on a V/Q scan it is seen indirectly as a region that is ventilated but not perfused, and on echocardiography it is seen functionally as strain on the overloaded right ventricle. Understanding the physical basis of each appearance allows you to interpret reports critically rather than accepting them as opaque conclusions, and it lets you appreciate why a 'normal chest X-ray' never excludes the diagnosis.
CTPA findings:
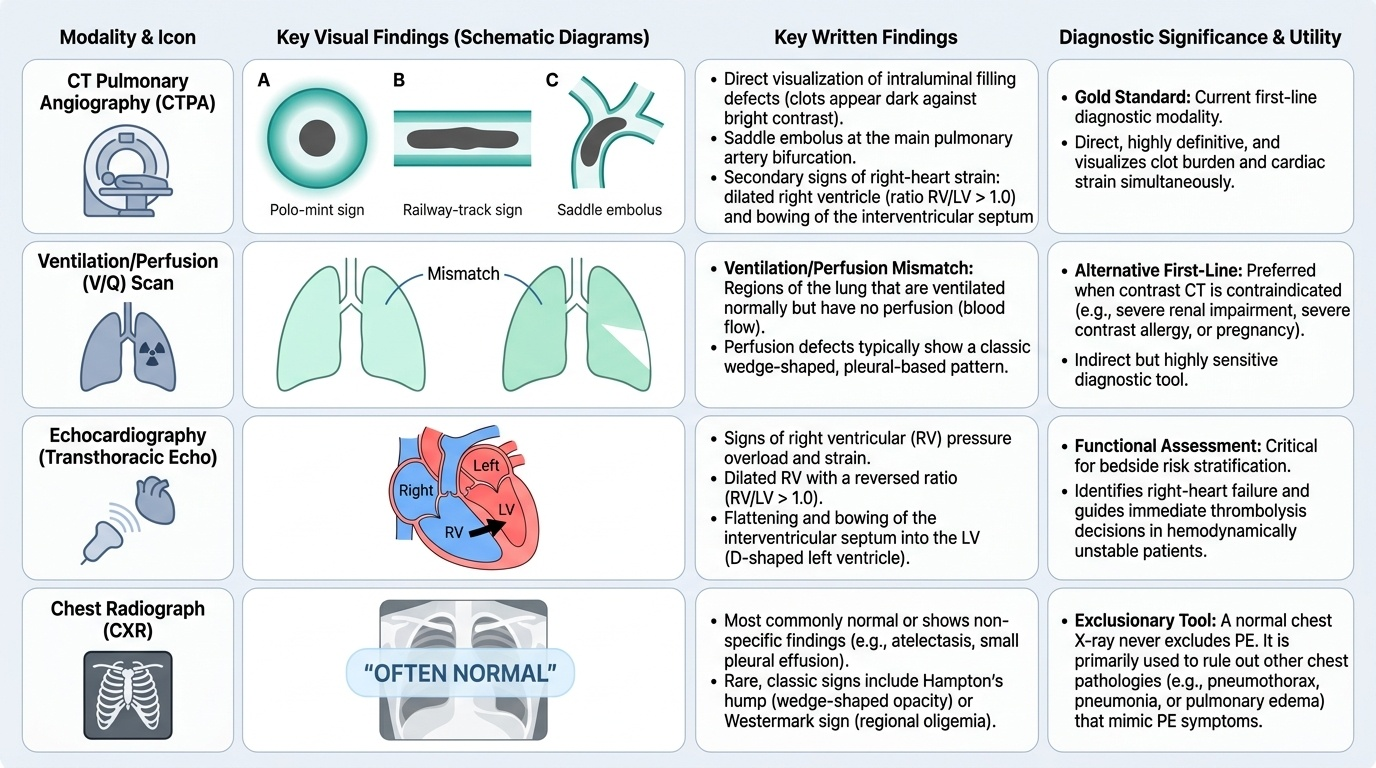
- Intraluminal filling defect: the embolus appears as a low-attenuation (dark) filling defect surrounded by bright contrast within a pulmonary artery — the direct and diagnostic sign.
- Polo-mint sign (clot surrounded by contrast on a vessel seen in cross-section) and the railway-track sign (clot outlined by contrast on a vessel seen along its length).
- Saddle embolus: a large clot straddling the bifurcation of the main pulmonary artery — a marker of central, potentially high-risk PE.
- Signs of right-heart strain: a dilated right ventricle with an increased RV/LV diameter ratio (>1.0), bowing of the interventricular septum toward the left ventricle, and reflux of contrast into the inferior vena cava and hepatic veins.
- Pulmonary infarct: a peripheral, wedge-shaped area of consolidation with its base against the pleura.
V/Q scan findings:
- A mismatched defect — a segment that is normally ventilated but shows absent or reduced perfusion — is the hallmark of PE. The result is reported as a probability (for example by the modified PIOPED or PISA-PED criteria) ranging from normal/very-low to high probability. A high-probability scan in a patient with high clinical probability confirms PE; a normal perfusion scan effectively excludes it.
Chest radiograph signs (insensitive, mostly historical eponyms):
- Westermark sign: regional oligaemia (an area of reduced vascular markings) distal to the occluded artery.
- Hampton's hump: a peripheral wedge-shaped pleural-based opacity of pulmonary infarction.
- Fleischner sign: a prominent (enlarged) central pulmonary artery.
Echocardiographic findings:
Acute right-ventricular dilatation and hypokinesia, septal flattening, tricuspid regurgitation and pulmonary hypertension, sometimes with the McConnell sign (RV free-wall hypokinesis with apical sparing). These functional signs guide urgent decisions in the unstable patient.
Provided image
SELF-CHECK
On a CT pulmonary angiogram, which single finding is the direct, diagnostic sign of acute pulmonary embolism?
A. A peripheral wedge-shaped pleural-based opacity (Hampton's hump)
B. An area of reduced vascular markings (regional oligaemia)
C. A low-attenuation intraluminal filling defect surrounded by contrast within a pulmonary artery
D. An enlarged central pulmonary artery
Reveal Answer
Answer: C. A low-attenuation intraluminal filling defect surrounded by contrast within a pulmonary artery
The direct, diagnostic sign of PE on CTPA is an intraluminal filling defect — the clot itself, seen as a low-attenuation (dark) defect surrounded by bright contrast within the pulmonary artery (the polo-mint and railway-track signs describe this clot-in-contrast appearance). Hampton's hump and regional oligaemia (Westermark sign) are insensitive chest-radiograph signs, and an enlarged central pulmonary artery (Fleischner sign) is also a non-specific radiographic finding. Only the visualised intraluminal clot on CTPA is diagnostic.