Page 5 of 17
RD7.3 | Imaging in Pulmonary Embolism — SDL Guide (Part 2)
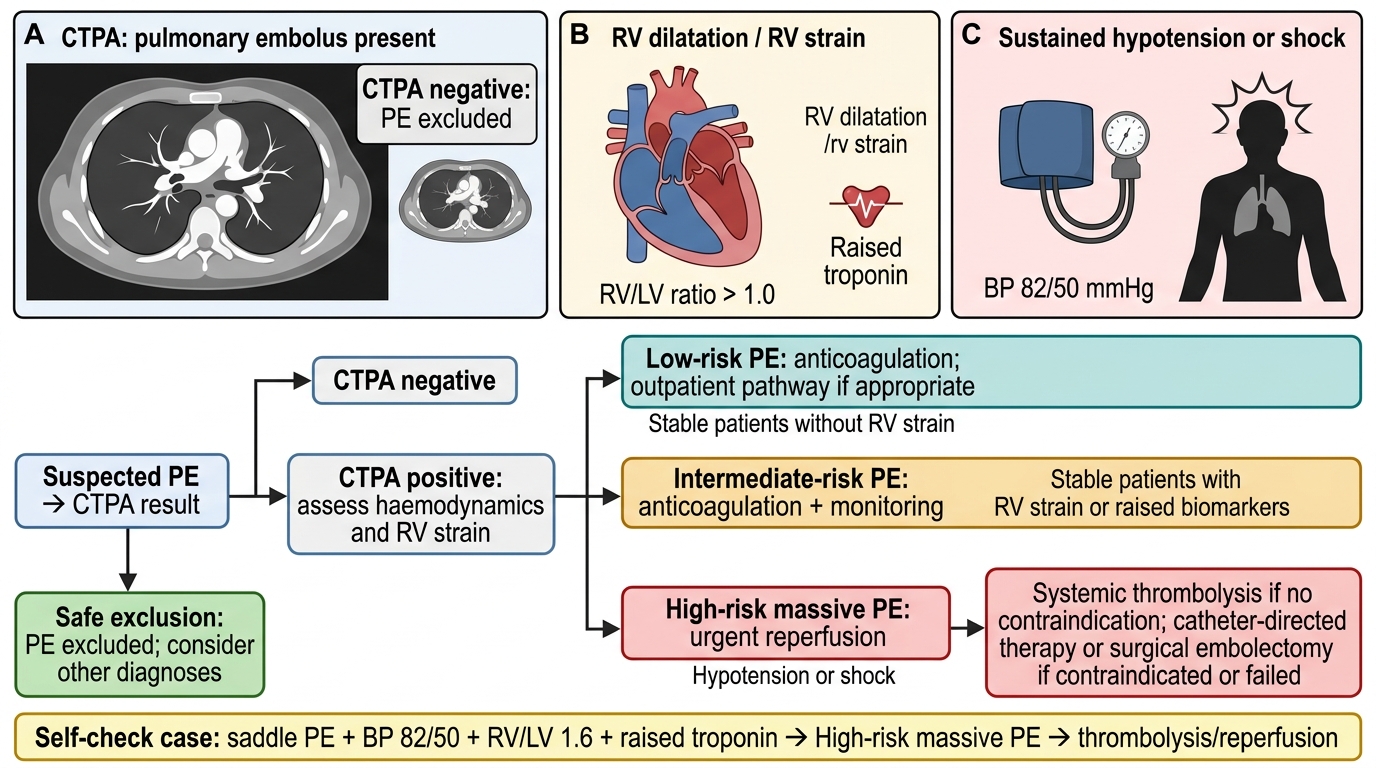
Impact on Management — From Image to Anticoagulation and Beyond
The clinical value of imaging in pulmonary embolism lies in how directly the result, combined with an assessment of right-ventricular function and haemodynamics, determines treatment. A confirmed PE is not a single disease with a single treatment; the imaging and physiological findings together place the patient on a severity spectrum that ranges from a small subsegmental clot in a well patient to a saddle embolus causing obstructive shock, and the treatment escalates accordingly. This is the integrative reasoning at the centre of competency RD7.3: the radiological diagnosis is only useful when it is fused with the clinical picture to choose between simple anticoagulation, reperfusion therapy, or — when imaging is negative — confident exclusion and a search for an alternative cause.
Confirmed PE — anticoagulation is the default:
The majority of patients with confirmed PE who are haemodynamically stable are treated with anticoagulation, increasingly with a direct oral anticoagulant (DOAC) or low-molecular-weight heparin. The CTPA result confirms the diagnosis and triggers prompt anticoagulation, which prevents clot propagation and recurrence while the body's own fibrinolysis resolves the existing embolus.
High-risk (massive) PE — reperfusion therapy:
When the patient is haemodynamically unstable (sustained hypotension/shock) — typically with imaging or echocardiographic evidence of right-ventricular strain — the patient has high-risk PE and may require systemic thrombolysis (or catheter-directed therapy or surgical embolectomy where thrombolysis is contraindicated or fails). Here the RV/LV ratio on CTPA and the echocardiographic strain findings are pivotal: they identify the patient for whom rapid reperfusion is life-saving.
Risk stratification of the normotensive patient:
Not every confirmed PE carries the same risk. In normotensive patients, tools such as the simplified Pulmonary Embolism Severity Index (sPESI), cardiac troponin (a marker of RV myocardial injury) and the imaging RV/LV ratio stratify patients into low and intermediate risk. This determines whether a patient can be considered for early/ambulatory management or needs monitored inpatient care.
Negative imaging — safe exclusion:
A negative CTPA (or a normal-to-very-low-probability V/Q scan) in a patient with appropriate clinical probability safely excludes PE, allowing anticoagulation to be withheld and the clinician to pursue the true alternative diagnosis — the very value that makes CTPA so useful, because it often reveals that alternative directly.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
CTPA and RV Strain Pathway for Pulmonary Embolism Management
SELF-CHECK
A 60-year-old man has a CTPA confirming a saddle pulmonary embolism. He is hypotensive (BP 82/50 mmHg) with a dilated right ventricle (RV/LV ratio 1.6) and raised troponin. He has no contraindication to thrombolysis. What is the most appropriate management category?
A. Low-risk PE; discharge on a direct oral anticoagulant with outpatient follow-up
B. High-risk (massive) PE; consider systemic thrombolysis (or catheter-directed/surgical reperfusion)
C. Intermediate-risk PE; standard anticoagulation alone is sufficient with no escalation
D. PE excluded; the haemodynamic findings indicate cardiogenic shock from another cause
Reveal Answer
Answer: B. High-risk (massive) PE; consider systemic thrombolysis (or catheter-directed/surgical reperfusion)
This patient has confirmed PE with sustained hypotension/shock plus imaging and biochemical evidence of right-ventricular strain (RV/LV ratio >1.0 and raised troponin) — the definition of high-risk (massive) PE. The integration of the CTPA finding (saddle embolus) with the haemodynamic and RV-strain assessment routes him to urgent reperfusion: systemic thrombolysis, or catheter-directed therapy / surgical embolectomy if thrombolysis is contraindicated or fails. Standard anticoagulation alone is inadequate for high-risk PE, and the diagnosis is confirmed, not excluded.
CLINICAL PEARL
Pearl 1 — The chest X-ray cannot exclude PE. A normal chest radiograph is the rule, not the exception, in pulmonary embolism. Its job is to find an alternative explanation (pneumonia, pneumothorax) — never to rule PE in or out. Do not let a 'normal CXR' falsely reassure you in a breathless, hypoxic patient.
Pearl 2 — Score first, scan second. Always anchor the decision in a validated pre-test probability (Wells/Geneva) and the appropriate D-dimer. A normal D-dimer in a low-probability patient excludes PE without any imaging, sparing radiation and contrast; in patients over 50 use the age-adjusted cut-off (age × 10 ng/mL) to avoid unnecessary scans.
Pearl 3 — Contrast and the kidney. CTPA is first-line, but iodinated contrast is generally avoided when the eGFR is below 30 mL/min/1.73m². In that situation, in contrast allergy, and often in pregnancy, the V/Q (or perfusion-only) scan is the safer route — and in pregnancy a leg ultrasound showing DVT may confirm VTE and avoid chest imaging entirely.
Self-Assessment — PE Imaging Decisions
Work through these scenarios as if you are the admitting clinician. Decide your imaging pathway and reasoning before reading each discussion, then check whether your sequence — score, D-dimer where appropriate, definitive imaging, integration with treatment — matches the recommended approach. The goal of this self-assessment is to consolidate the habit of reasoning from pre-test probability to the correct modality and then to management, which is exactly the integrative skill competency RD7.3 is testing. Treat each scenario as a real decision with real consequences for radiation, contrast exposure and timely treatment.
Scenario A: A 35-year-old man presents with pleuritic chest pain after a minor calf injury. He has no tachycardia, normal oxygen saturation, and his two-tier Wells score classifies PE as 'unlikely'. His age-adjusted D-dimer is normal. Does he need a CTPA?
Discussion: No. In a patient with 'unlikely' clinical probability and a normal (age-adjusted) D-dimer, PE is safely excluded without any imaging. Proceeding to CTPA here would expose him to needless radiation and contrast. This is the central efficiency of the diagnostic pathway: the score and the D-dimer together can confidently rule out PE in the low-risk patient.
Scenario B: A 28-year-old woman who is 30 weeks pregnant develops sudden breathlessness and a raised heart rate. Her chest radiograph is normal. How should she be investigated?
Discussion: In pregnancy, D-dimer is physiologically elevated and is much less useful. Many units begin with bilateral lower-limb compression ultrasound — if a DVT is found, VTE is confirmed and chest imaging can be avoided. If chest imaging is needed and the chest radiograph is normal, a perfusion-only (Q) scan is often preferred because it delivers a lower breast radiation dose than CTPA while still detecting the perfusion defect; CTPA remains an acceptable alternative. The choice balances maternal and fetal radiation against diagnostic certainty.
Scenario C: A 70-year-old woman with confirmed PE on CTPA is normotensive but has an RV/LV ratio of 1.2 and a mildly raised troponin. Is anticoagulation alone adequate, or does she need thrombolysis?
Discussion: She is normotensive, so she does not meet the criterion for high-risk (massive) PE that mandates reperfusion. However, the right-ventricular dilatation and raised troponin place her in the intermediate-risk category. She should receive anticoagulation with close monitoring rather than routine thrombolysis; thrombolysis in intermediate-risk PE is reserved for those who subsequently deteriorate. This illustrates how the imaging RV/LV ratio and biomarkers refine management even when blood pressure is preserved.