Page 1 of 14
RD3.{1,3} | Radiation Types, Biological Hazards and Dose Awareness — SDL Guide
Learning Objectives
- Distinguish ionising from non-ionising radiation used in diagnostic imaging and identify which modalities deliver each.
- Classify the biological effects of ionising radiation into stochastic and deterministic categories and give clinical examples of each.
- Explain how ionising radiation damages tissue through direct and indirect DNA damage and relate this to acute and long-term effects.
- State the units of radiation measurement — Gray for absorbed dose, Sievert for equivalent and effective dose — and use them correctly.
- Describe the devices used to monitor occupational radiation exposure in health-care workers, principally the thermoluminescent dosimeter (TLD).
INSTRUCTIONS
Every clinician who signs an imaging request shares responsibility for the radiation that request delivers. This module builds the scientific foundation for that responsibility: what radiation is, how it harms tissue, the two fundamentally different ways it can harm (stochastic and deterministic), how we quantify it, and how we monitor the staff who work with it daily. You cannot apply the ALARA principle or interpret a dosimeter report without first understanding these concepts, so this SDL is the prerequisite for the radiation-protection and regulatory material that follows.
References
- Sutton's Textbook of Radiology and Imaging, 7th edition, Chapter 1 (Physics and Radiation Protection) (textbook)
- Grainger & Allison's Diagnostic Radiology, 7th edition, Chapter on Radiation Protection and Dosimetry (textbook)
- Atomic Energy Regulatory Board (AERB) Safety Code for Medical Diagnostic X-ray Equipment and Installations, India (guideline)
- ICRP Publication 103 (2007 Recommendations of the International Commission on Radiological Protection) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A radiographer in your hospital has worn the same film badge on her lapel for three months. At the quarterly review, her cumulative reading is higher than her colleagues'. She feels completely well — no rash, no hair loss, no symptoms whatsoever. Should anyone be concerned? The answer lies in understanding that ionising radiation harms the human body in two utterly different ways. One kind of harm — a burn, hair loss, a cataract — needs a large dose and appears within days to months; her normal appearance rules it out. The other kind — a cancer that may surface fifteen years from now — has no safe lower limit, no immediate sign, and rises in probability with every millisievert she accumulates. Her badge is not measuring how she feels today; it is measuring a lifetime statistical risk. To protect her, and to protect every patient you image, you must first understand these two faces of radiation injury and how we measure the invisible dose that drives them.
WHY THIS MATTERS
Radiation awareness is not a radiology-department specialty; it is a core clinical safety skill that the NMC places squarely on the requesting doctor. Competency RD3.1 requires you to be aware of the different types of radiation and of the stochastic and non-stochastic hazards — acute and long-term — that ionising radiation poses to human beings. Competency RD3.3 requires you to understand how radiation exposure in health-care workers is monitored with dosimeters such as the thermoluminescent dosimeter (TLD), and to know the units in which radiation exposure is measured. These are examinable facts and, more importantly, they shape real decisions: whether to repeat a poor-quality film, whether to choose ultrasound over CT in a young patient, and how to respond when a colleague's dosimeter reading climbs. A clinician who confuses Gray with Sievert, or who believes a cancer risk only exists above some safe dose, will make unsafe choices. This SDL gives you the vocabulary and the conceptual map that the rest of radiation protection is built upon.
RECALL
Before reading further, bring back the relevant physics from your Year-1 biophysics:
- Ionisation: radiation is 'ionising' when each photon or particle carries enough energy to eject an electron from an atom, leaving a charged ion. X-rays and gamma rays cross this energy threshold; visible light, radio waves and ultrasound do not.
- The electromagnetic spectrum: X-rays and gamma rays sit at the high-energy, short-wavelength end. They differ in origin — X-rays come from electron interactions in an X-ray tube, gamma rays from the nucleus of a radioactive atom — but both are ionising.
- Sound is mechanical, not electromagnetic: ultrasound is a longitudinal pressure wave and carries no ionising energy at all.
- DNA is the critical target: the genetic material in the cell nucleus is the molecule whose damage matters most for both cancer and cell death.
- Energy deposited per unit mass: recall that energy (joules) delivered to a mass (kilograms) is the basic idea behind 'dose'.
If any of these are hazy, a five-minute review of your biophysics notes will make the mechanisms below far clearer.
Why Radiation Awareness Matters at the Point of Ordering
Medical imaging is the single largest man-made source of radiation exposure to the general population, and the decision that creates almost all of that exposure is the clinical decision to order an investigation. The radiologist optimises the technique and the radiographer operates the equipment, but the dose exists only because a clinician judged the examination necessary. This is why radiation awareness belongs to every doctor and not only to the radiology team: the justification for an ionising procedure is a clinical judgement, made at the moment of ordering, that the diagnostic benefit outweighs the radiation risk. You cannot make that judgement honestly without understanding what the risk actually is.
The first and most important distinction is between two families of radiation used in imaging:
- Ionising radiation — carries enough energy to ionise atoms and therefore to damage DNA. In diagnostic imaging this means X-rays (used in plain radiography, fluoroscopy, angiography and CT) and gamma rays (used in nuclear medicine, emitted by an administered radiopharmaceutical). Every one of these procedures delivers a measurable dose that must be justified.
- Non-ionising radiation — does not have enough energy to ionise atoms. Ultrasound uses mechanical sound waves; MRI uses radiofrequency pulses within a static magnetic field. Neither delivers an ionising dose, which is why both are preferred when they answer the clinical question — particularly in pregnancy and in children.
The clinical rule that flows from this is simple and powerful: when a non-ionising modality can answer the question, the ionising alternative requires explicit justification. Holding that rule in mind reframes every imaging request as a risk-benefit decision rather than a reflex.
Types of Radiation and How Ionising Radiation Damages Tissue
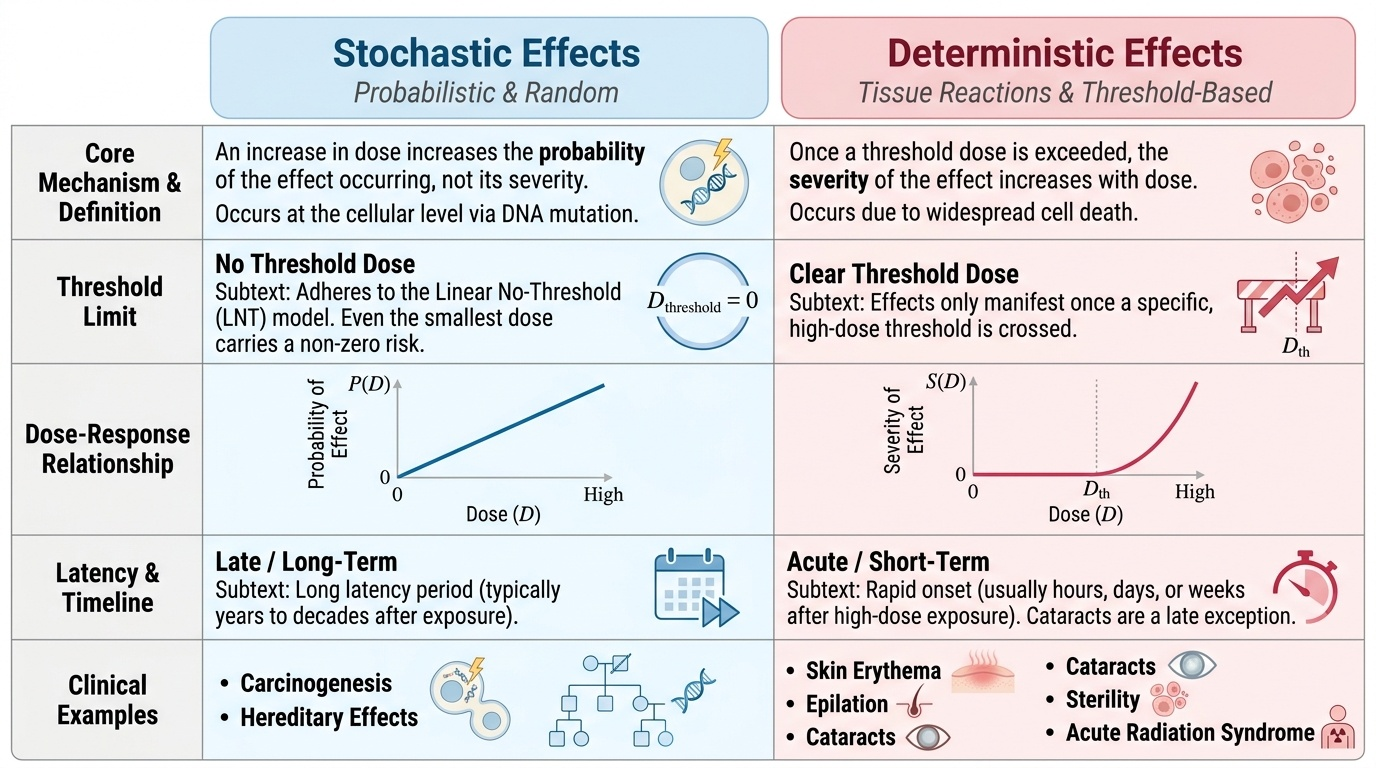
Having separated ionising from non-ionising radiation, we now turn to the central concept of this competency: ionising radiation injures human tissue in two biologically distinct ways, and confusing them is a classic source of clinical and examination error. The two categories are not points on a single spectrum — they obey different rules about dose, threshold and severity, and they produce different clinical pictures. Understanding the distinction is what allows you to reassure (or not reassure) a patient or a colleague correctly, and it is the scientific foundation for every dose-limiting practice you will later adopt.
Stochastic effects are probabilistic. The word 'stochastic' means random: as dose rises, it is the probability of the effect occurring that increases, not its severity. Crucially, stochastic effects are assumed to have no threshold dose — the linear-no-threshold (LNT) model holds that even the smallest dose carries some non-zero risk, derived largely from atomic-bomb survivor (Life Span Study) data. They are typically long-term (late) effects with a long latency. The two stochastic effects are:
- Carcinogenesis — radiation-induced cancer (a somatic-cell mutation), the dominant concern at diagnostic doses.
- Hereditary (genetic) effects — mutations in germ cells that may be passed to offspring.
Deterministic effects (also called non-stochastic or, in current ICRP terminology, tissue reactions) are different. They occur only above a threshold dose, and once that threshold is crossed, the severity of the effect rises with dose. They reflect the death of a large number of cells and are usually acute or sub-acute. Classic deterministic effects include:
- Skin erythema and desquamation (radiation burns)
- Epilation (hair loss)
- Cataract (lens opacity)
- Sterility (gonadal cell loss)
- Acute radiation syndrome (high whole-body doses)
The practical lesson, returning to the hook: a well-looking radiographer cannot have a deterministic injury, because those produce visible signs above a threshold — but her accumulated dose still contributes to a stochastic (cancer) risk that carries no threshold at all.
Provided image
SELF-CHECK
A patient asks whether the small dose from a single chest X-ray is 'safe' or whether it carries any cancer risk at all. Based on the accepted model of radiation effects, which statement is most accurate?
A. There is a safe threshold dose below which a chest X-ray carries no cancer risk whatsoever
B. Cancer induction is a stochastic effect with no assumed threshold, so even a small dose carries a small, non-zero probabilistic risk
C. A chest X-ray causes a deterministic effect, so the risk depends only on whether a threshold is exceeded
D. There is no cancer risk because chest X-rays use non-ionising radiation
Reveal Answer
Answer: B. Cancer induction is a stochastic effect with no assumed threshold, so even a small dose carries a small, non-zero probabilistic risk
Radiation-induced cancer is a stochastic effect: the probability rises with dose and there is no assumed safe threshold (the linear-no-threshold model). So a chest X-ray carries a very small but non-zero probabilistic risk — it is not 'zero', but it is extremely low (~0.02 mSv). It is NOT a deterministic effect (those need a threshold dose and produce graded severity, e.g. burns, cataract). And a chest X-ray uses X-rays, which ARE ionising. Honest counselling acknowledges the tiny non-zero risk while keeping it in perspective.
Mechanism — Direct and Indirect DNA Damage, Acute vs Long-term Effects
To understand why the same physical agent produces two such different categories of effect, we must look at how ionising radiation actually damages a cell. The damage begins with ionisation events scattered along the radiation track, but the biological target that matters most is the DNA in the cell nucleus, because it is the molecule whose corruption drives both cancer and cell death. Radiation reaches this target by two distinct routes, and the relative importance of each shapes the eventual clinical outcome. This mechanistic understanding is what connects the abstract dose number to the clinical effect you might see at the bedside, and it explains both the acute, threshold-dependent injuries and the late, probabilistic ones within a single coherent picture. Holding the mechanism in mind also prevents the common error of treating stochastic and deterministic effects as unrelated phenomena, when in fact both arise from the very same DNA-damage events differing only in scale.
There are two mechanisms of DNA damage:
- Direct action: an X-ray or gamma photon (or a secondary electron it sets in motion) deposits energy directly in the DNA molecule, breaking a strand. This is the dominant mechanism for densely ionising radiation.
- Indirect action: the photon ionises a water molecule (the cell is ~80% water), a process called radiolysis, generating highly reactive free radicals (notably the hydroxyl radical, ·OH). These free radicals then diffuse the short distance to the DNA and damage it chemically. For the low-LET (linear energy transfer) radiation used in diagnostic imaging — X-rays and gamma rays — indirect action via free radicals is the predominant route of damage.
The cell's fate then depends on how much DNA damage occurs and how well it is repaired:
- A small number of damaged cells with mis-repaired but viable DNA can survive carrying a mutation. If that mutation is in a somatic cell it may, years later, initiate a cancer; if in a germ cell, a hereditary effect. This is the origin of stochastic effects — a single sub-lethally damaged cell is enough, so there is no threshold, and the outcome appears only after a long latency (long-term effects).
- A large number of cells killed outright in a tissue overwhelms its capacity to function and regenerate. This requires a high dose (a threshold), and the more cells killed, the worse the clinical picture — producing deterministic effects such as skin burns and acute radiation syndrome (acute effects).
Thus a single mechanism (DNA damage) branches into two effect categories depending on whether the dominant consequence is a few surviving mutated cells (stochastic, late) or mass cell death (deterministic, early).
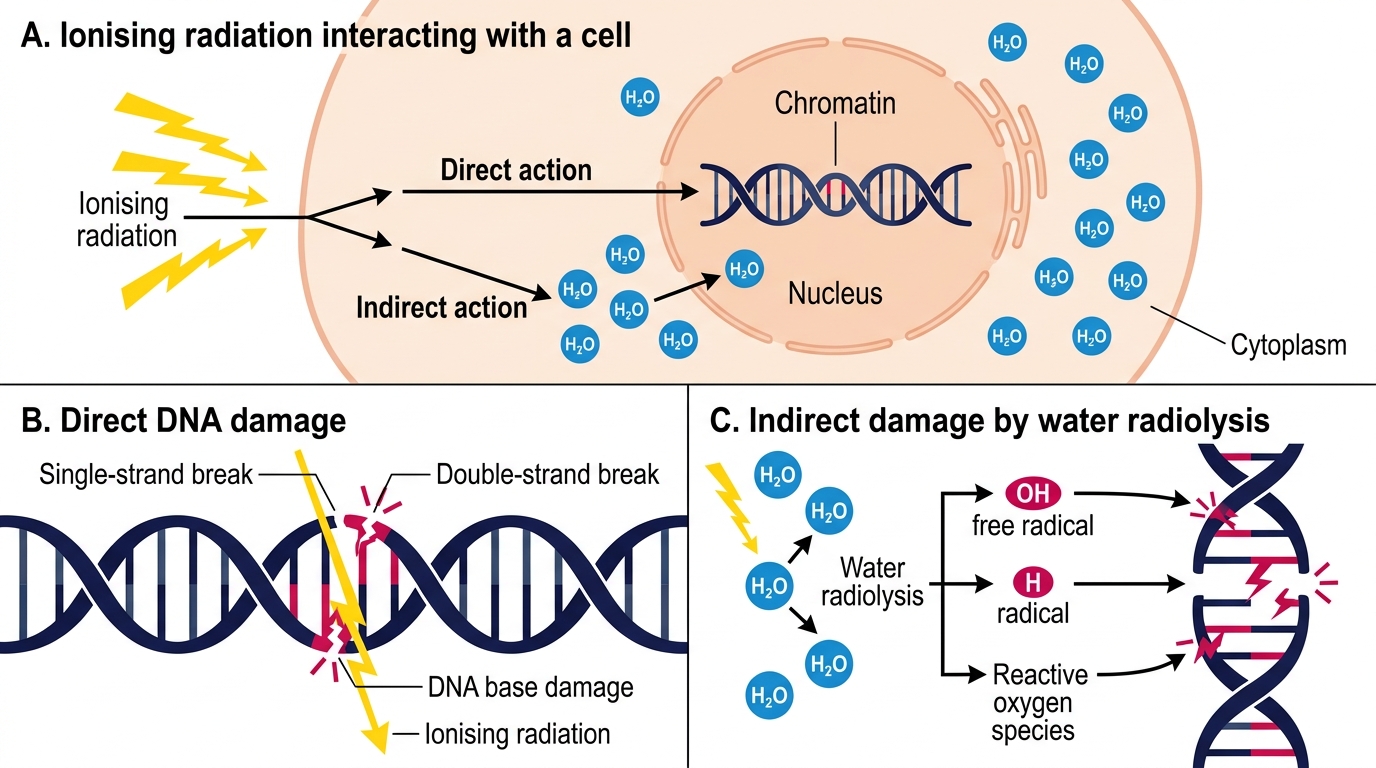
Direct and Indirect DNA Damage by Ionising Radiation