Page 2 of 14
RD3.{1,3} | Radiation Types, Biological Hazards and Dose Awareness — SDL Guide (Part 2)
Measuring and Monitoring Radiation — Units and Dosimeters
Knowing that radiation causes harm is only half of competency RD3.3; the other half is being able to quantify exposure in the correct units and to know how an individual worker's exposure is tracked over time. Imprecise use of radiation units — saying 'Gray' when you mean 'Sievert' — is a common and consequential error, because the two units answer fundamentally different questions about the same exposure. The units exist precisely because the same amount of physical energy deposited in tissue can carry very different biological risk depending on the type of radiation delivering it and the radiosensitivity of the tissue it strikes. A clear grasp of the three dose quantities, and of the device that records a worker's cumulative exposure, is therefore essential before any dosimeter report or examination dose can be interpreted sensibly rather than recited mechanically.
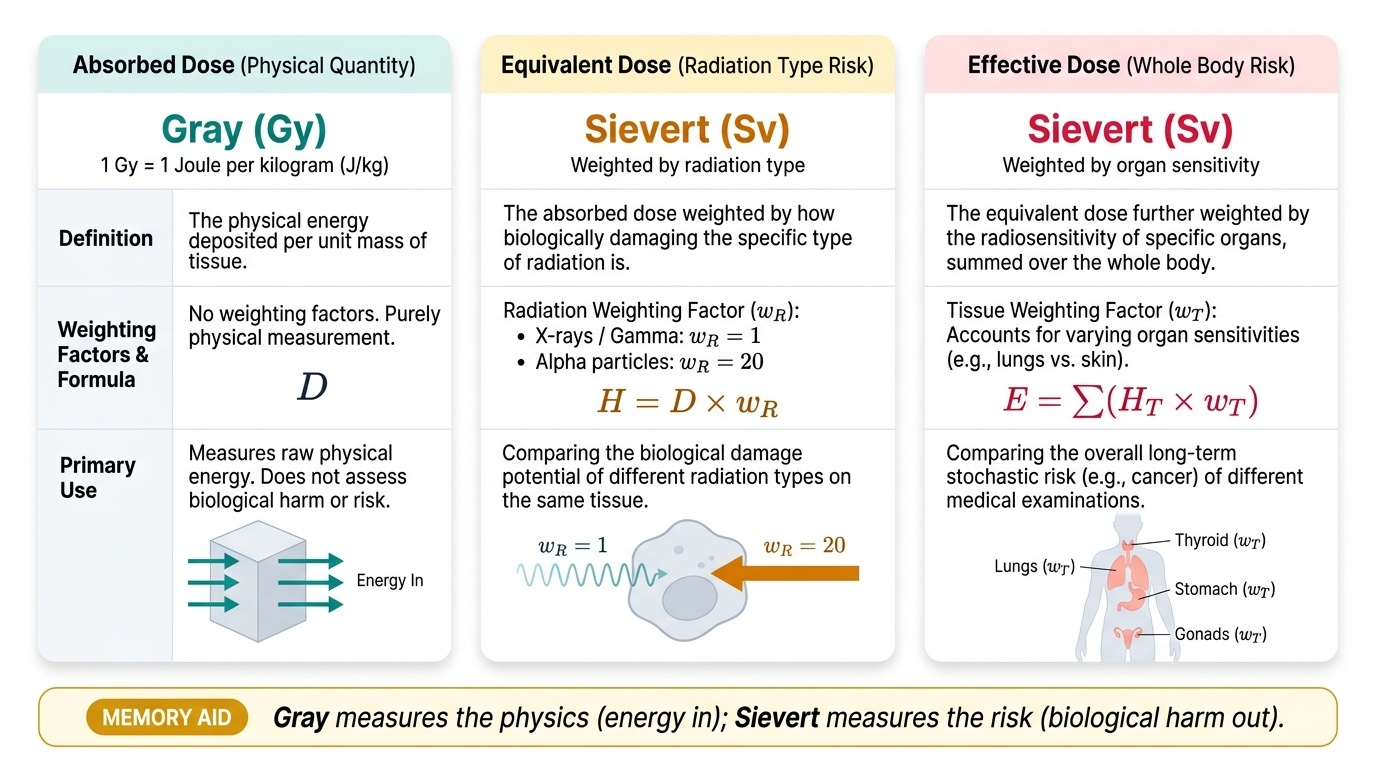
Three dose quantities, with two units, must be distinguished:
- Absorbed dose — the physical energy deposited per unit mass of tissue (joules per kilogram). Its unit is the Gray (Gy). This is a purely physical quantity and says nothing about biological risk.
- Equivalent dose — the absorbed dose weighted by a radiation weighting factor that accounts for how biologically damaging that type of radiation is (X-rays and gamma rays have a factor of 1; alpha particles, far higher). Its unit is the Sievert (Sv).
- Effective dose — the equivalent dose further weighted by tissue weighting factors that account for the differing radiosensitivity of organs, then summed over the whole body. Its unit is also the Sievert (Sv). Effective dose (usually quoted in millisieverts, mSv) is the quantity used to compare the stochastic risk of different examinations.
A useful memory aid: Gray measures the physics (energy in); Sievert measures the risk (biological harm out).
Monitoring an individual worker's accumulated dose requires a personal dosimeter worn during working hours. The principal devices are:
- Thermoluminescent dosimeter (TLD) — the primary occupational monitor in most modern services. It contains a crystal (e.g. lithium fluoride) that stores energy when irradiated; when later heated in a reader, it releases that energy as light, and the amount of light is proportional to the accumulated dose. TLDs are accurate, re-usable and tissue-equivalent.
- Film badge — an older device in which a photographic film darkens in proportion to dose; filters in the holder allow the type and energy of radiation to be estimated. It provides a permanent record but is single-use and less precise than a TLD.
- Pocket dosimeter (direct-reading) — gives an immediate readout of accumulated dose, useful when a real-time check is needed, though less accurate for the legal cumulative record.
- Optically stimulated luminescence (OSL) dosimeters are an increasingly used modern alternative to the TLD, read out by laser light rather than heat.
The dosimeter is worn at collar or chest level over a 1–3 month wear period; the reading is the worker's official exposure record against which occupational dose limits are checked.
Provided image
SELF-CHECK
A medical physicist reports that a worker's thermoluminescent dosimeter shows an accumulated effective dose for the quarter. In which unit should this effective dose be expressed, and what does the device fundamentally measure?
A. Gray; the TLD measures absorbed physical energy only
B. Sievert; the TLD stores energy in a crystal that emits light proportional to dose when heated, used to track the worker's biologically weighted exposure
C. Becquerel; the TLD measures the radioactivity administered to the worker
D. Gray; the TLD darkens a photographic film in proportion to dose
Reveal Answer
Answer: B. Sievert; the TLD stores energy in a crystal that emits light proportional to dose when heated, used to track the worker's biologically weighted exposure
Effective dose (and equivalent dose) is expressed in Sieverts (Sv), because it is biologically weighted for radiation type and tissue radiosensitivity — the quantity used to track occupational risk. Absorbed dose in Gray (Gy) is the purely physical quantity. A thermoluminescent dosimeter (TLD) works by storing energy in a crystal (e.g. lithium fluoride); heating it in a reader releases stored energy as light proportional to the dose received. Darkening a photographic film describes the older FILM badge, not a TLD. Becquerel is the unit of radioactivity (decays per second), not personnel dose.
Clinical and Applied Significance — Dose Awareness in Practice
The applied value of all this theory is the ability to attach a realistic sense of magnitude to the investigations you order, and to act correctly on a dosimeter report. Dose awareness means carrying an approximate mental scale of how much radiation each common test delivers, expressed in effective dose (mSv), so that the choice between, say, repeating a plain film and proceeding to CT is informed by the radiation cost as well as the diagnostic gain. A clinician with no sense of these magnitudes treats a CT as casually as a chest X-ray, when in fact the CT delivers several hundred times the dose.
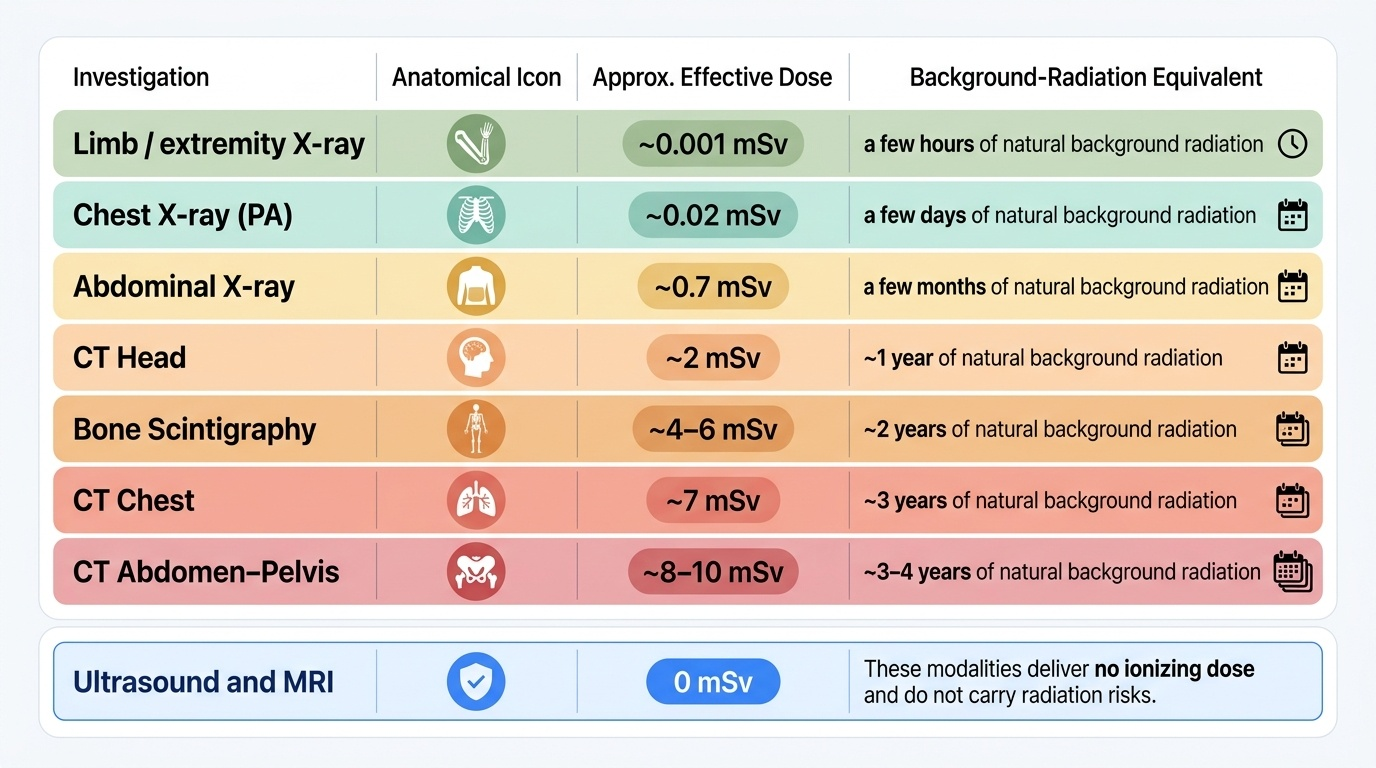
Approximate effective doses worth committing to memory (and expressing relative to natural background radiation, which is roughly 2–3 mSv per year in India):
| Investigation | Approx. effective dose | Background-equivalent |
|---|---|---|
| Chest X-ray (PA) | ~0.02 mSv | a few days |
| Limb / extremity X-ray | ~0.001 mSv | hours |
| Abdominal X-ray | ~0.7 mSv | a few months |
| CT head | ~2 mSv | ~1 year |
| CT chest | ~7 mSv | ~3 years |
| CT abdomen–pelvis | ~8–10 mSv | ~3–4 years |
| Bone scintigraphy | ~4–6 mSv | ~2 years |
Ultrasound and MRI deliver no ionising dose and do not appear on this scale at all.
Three applied principles follow from dose awareness:
- Special populations: the fetus and children are more radiosensitive because of rapidly dividing cells and a longer lifespan over which a stochastic cancer can manifest. Pregnancy must be considered before any abdominal/pelvic ionising study, and paediatric protocols deliberately reduce dose. Justification and optimisation are heightened in both groups.
- Occupational monitoring obligations: staff who work with ionising radiation are 'radiation workers' who must wear a personal dosimeter (TLD or equivalent), and their cumulative readings are checked against occupational dose limits. A reading trending upward triggers a review of working practice (positioning, shielding, technique) — not a diagnosis of illness, because at occupational levels the concern is the stochastic risk, not an acute injury.
- Repeat-examination discipline: an unnecessary repeat film is pure added dose with no new information. Dose awareness makes 'is this repeat truly needed?' a routine question.
This quantitative sense — not memorising every number, but holding the orders of magnitude — is what converts radiation theory into safer clinical behaviour.
Provided image
CLINICAL PEARL
Pearl 1 — Stochastic vs deterministic in one line: Stochastic = no threshold, dose changes the probability (cancer, hereditary effects, late). Deterministic (= non-stochastic = tissue reaction) = has a threshold, dose changes the severity (skin erythema, cataract, sterility, acute radiation syndrome, early). If a question describes a clear threshold and graded severity, it is deterministic; if it describes 'no safe dose', it is stochastic.
Pearl 2 — Gray vs Sievert: Gray = energy (physics in); Sievert = risk (biological harm out). Effective dose for comparing examinations is always in mSv (Sievert). Quoting an examination dose in Gray is a unit error.
Pearl 3 — The TLD is the workhorse: the thermoluminescent dosimeter is the standard personal monitor — a heated crystal that emits light proportional to accumulated dose. A 'well-looking worker with a high badge reading' is a stochastic-risk concern (review practice), not an acute-illness concern.
Self-Assessment — Hazards, Units and Monitoring
Use these scenarios to test your grasp of radiation hazards, units and monitoring. Write your answer before reading the discussion — active recall consolidates these high-yield distinctions far better than re-reading.
Scenario A: An interventional cardiologist who has worked in the catheterisation laboratory for twenty years develops bilateral posterior subcapsular cataracts. A colleague claims this 'proves there is no safe dose of radiation'. Is the colleague's reasoning correct?
Discussion: No — the reasoning confuses the two effect categories. Cataract is a deterministic (tissue-reaction) effect: it occurs only above a threshold dose, and its severity increases with dose. It does not illustrate the no-threshold ('no safe dose') principle, which applies to stochastic effects (cancer, hereditary effects). The cataract instead illustrates that chronic occupational exposure can exceed a deterministic threshold — which is exactly why ICRP lowered the occupational lens-of-eye equivalent-dose limit to 20 mSv/year (averaged over 5 years) and why interventionalists must use lead eyewear and ceiling-suspended shields.
Scenario B: A junior doctor writes in the notes that a CT abdomen 'delivered 8 Gray to the patient'. The radiographer corrects the entry. What was wrong, and what is the correct statement?
Discussion: The unit is wrong by three orders of magnitude and the wrong quantity. A CT abdomen delivers an effective dose of approximately 8–10 millisieverts (mSv), not 8 Gray. Gray is the unit of absorbed dose (physical energy); for comparing the stochastic risk of an examination we use effective dose in Sieverts. '8 Gray' would be a massive, potentially lethal whole-body absorbed dose — a deterministic-injury level, not a diagnostic CT.
Scenario C: A new radiographer asks how her radiation exposure will be tracked and what she should do if she ever feels unwell after a busy day of fluoroscopy. What do you tell her?
Discussion: Her exposure is tracked by a personal dosimeter — typically a thermoluminescent dosimeter (TLD) (or OSL/film badge) worn during working hours and read out periodically; the reading is her official occupational record, checked against dose limits. Feeling unwell after a normal working day is not a radiation effect — occupational diagnostic doses are far below any deterministic threshold for acute symptoms. The genuine occupational concern is the long-term stochastic risk, which is managed by keeping cumulative dose low (good technique, shielding, distance) rather than by watching for symptoms.