Page 7 of 17
RD7.4 | Imaging in Appendicitis — SDL Guide
Learning Objectives
- Recognise that acute appendicitis is largely a clinical diagnosis and identify when imaging is indicated.
- Select the appropriate first-line imaging modality for appendicitis according to patient group (child, young adult, pregnant woman, obese adult).
- Identify the ultrasound and CT findings of acute appendicitis and its complications.
- Integrate described imaging findings into the surgical management of appendicitis.
- Apply the principle of radiation stewardship (ALARA) when choosing imaging in children and pregnancy.
INSTRUCTIONS
Acute appendicitis is the commonest surgical emergency of the abdomen, and although the classic case is diagnosed clinically, atypical presentations are common — especially in children, pregnant women, the elderly and the obese — and these are where imaging changes management. Choosing the right modality is not arbitrary: it is governed by accuracy in the specific patient and by the duty to avoid unnecessary radiation in the young and the pregnant. This module, aligned to competency RD7.4, trains you to decide when and what to image, to read the inflamed appendix on ultrasound and CT, and to integrate those findings into a surgical decision.
References
- Sutton's Textbook of Radiology, 6th edition, Chapter on the Acute Abdomen (textbook)
- Grainger & Allison's Diagnostic Radiology, 6th edition, Chapter on the Gastrointestinal Tract (textbook)
- Alvarado A. A practical score for the early diagnosis of acute appendicitis, Ann Emerg Med 1986 (guideline)
- World Society of Emergency Surgery (WSES) Jerusalem guidelines for diagnosis and treatment of acute appendicitis (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 9-year-old girl is brought to casualty with a day of central abdominal pain that has now settled into the right lower abdomen, with vomiting, low-grade fever and a reluctance to walk or jump. The surgical team is fairly confident this is appendicitis, but the picture is not textbook and the parents are anxious about 'radiation from a CT scan'. What is the right first investigation? Not a CT — in a child, the answer is an ultrasound, which can show the inflamed appendix without any ionising radiation. The same clinical question in a 60-year-old obese man would be answered best by CT. The modality you choose for suspected appendicitis is not one-size-fits-all; it depends on who the patient is, and getting that choice right protects a child from needless radiation while still securing the diagnosis.
WHY THIS MATTERS
Appendicitis carries a lifetime risk of around 7–8%, making it something every clinician will encounter repeatedly. As a final-year student and intern on the surgical and emergency firms, you will assess right-iliac-fossa pain constantly, and you will be asked which scan — if any — to request. Competency RD7.4 requires you to integrate imaging findings into the surgical management of appendicitis, which means understanding not only what an inflamed appendix looks like on ultrasound and CT, but also why the first-line modality differs for a child, a pregnant woman and an obese adult. This is applied radiology with direct stakes: the right modality reduces negative appendicectomy rates and avoids irradiating children, while a missed or delayed diagnosis risks perforation, abscess and peritonitis.
RECALL
Before reading further, recall:
- Appendix anatomy (from AN): the appendix arises from the posteromedial caecum where the three taeniae coli converge; its tip position is variable (retrocaecal most common, also pelvic, subcaecal), which explains atypical presentations. McBurney's point lies a third of the way from the anterior superior iliac spine to the umbilicus.
- Pathophysiology (from Pathology): appendicitis typically begins with luminal obstruction (often by a faecolith/appendicolith or lymphoid hyperplasia), causing distension, bacterial overgrowth, mucosal ischaemia, transmural inflammation and ultimately gangrene and perforation if untreated.
- Migratory pain (from Surgery): early visceral peri-umbilical pain (from midgut innervation) shifts to somatic right-iliac-fossa pain once the inflamed appendix irritates the adjacent parietal peritoneum — a classic and useful clinical sign.
- ALARA principle (from RD-foundation): 'As Low As Reasonably Achievable' — ionising radiation should be minimised, especially in children and pregnancy, which is the rationale for preferring ultrasound and MRI over CT in these groups.
Clinical Scenario — Right Iliac Fossa Pain and When to Image
The starting point — and a frequent examination theme — is that acute appendicitis is largely a clinical diagnosis, and a patient with a classic presentation in whom the surgeon is confident may proceed to appendicectomy without imaging at all. The classic story is migratory pain (central to the right iliac fossa), anorexia, low-grade fever, nausea and vomiting, with localised tenderness and guarding at McBurney's point, and signs such as Rovsing's, psoas and obturator signs. Clinical probability can be formalised with the Alvarado score, which combines migratory pain, anorexia, nausea, RIF tenderness, rebound, fever, leucocytosis and a left shift; a high score supports operating, a low score supports observation, and an intermediate score is exactly where imaging helps most.
Imaging is therefore indicated in defined circumstances rather than for every patient:
- Equivocal or atypical presentations: an intermediate Alvarado score, an unclear clinical picture, or a presentation complicated by an unusual appendix position (e.g. retrocaecal or pelvic) that blunts the typical signs.
- Specific populations in whom the differential is wide: women of reproductive age (where ovarian and tubal pathology mimics appendicitis), the elderly (broad differential, higher complication rate), and the very young (difficult history and examination).
- Suspected complications: a palpable mass, prolonged symptoms or signs of an abscess, phlegmon or perforation that would change the operative plan.
The overarching principle is one of selective imaging: do not delay an obvious case for a scan, but use the right investigation to resolve genuine diagnostic uncertainty and to detect complications. Crucially, the choice of investigation is then dictated by the patient — chiefly by age, body habitus and pregnancy — because both diagnostic accuracy and the duty to limit radiation depend on who is in front of you.
Imaging Strategy — Ultrasound First in the Young, CT and MRI by Population
When imaging is needed, modality selection in appendicitis is the clearest example in this whole topic of matching the test to the patient, balancing diagnostic accuracy against radiation stewardship. The same disease is best imaged differently in a child, a pregnant woman and an obese adult, and the final-year student is expected to know the rationale, not merely the rule. The unifying logic is: use the most accurate test that avoids unnecessary ionising radiation in those most vulnerable to it (children and pregnant women), and reserve CT for the patients in whom it is both most accurate and least harmful.
Ultrasound (USG) — first-line in children, young/thin adults and pregnancy:
Graded-compression ultrasound is the first-line investigation in children, young or thin adults, and pregnant women because it uses no ionising radiation, is quick and bedside-available, and is accurate when the appendix is seen. Its principal limitation is operator dependence and reduced sensitivity in obese patients and when the appendix is retrocaecal or not visualised. A negative or non-visualising ultrasound in a patient with persisting suspicion does not exclude appendicitis and should prompt further imaging or observation.
CT abdomen/pelvis — more sensitive and specific in adults, the obese and equivocal cases:
Contrast-enhanced CT is the most sensitive and specific investigation overall and is preferred in adults, obese patients, and equivocal cases where ultrasound has failed to visualise the appendix. It reliably demonstrates the inflamed appendix and, importantly, its complications (abscess, perforation, phlegmon) and alternative diagnoses, which makes it the workhorse for the older adult with an uncertain acute abdomen. Its drawback is ionising radiation, which is why it is not the first choice in the young.
MRI — in pregnancy when ultrasound is inconclusive:
MRI uses no ionising radiation and is the investigation of choice in pregnant women in whom ultrasound is inconclusive, allowing the appendix to be assessed without irradiating the fetus. It is limited by availability and cost rather than by safety.
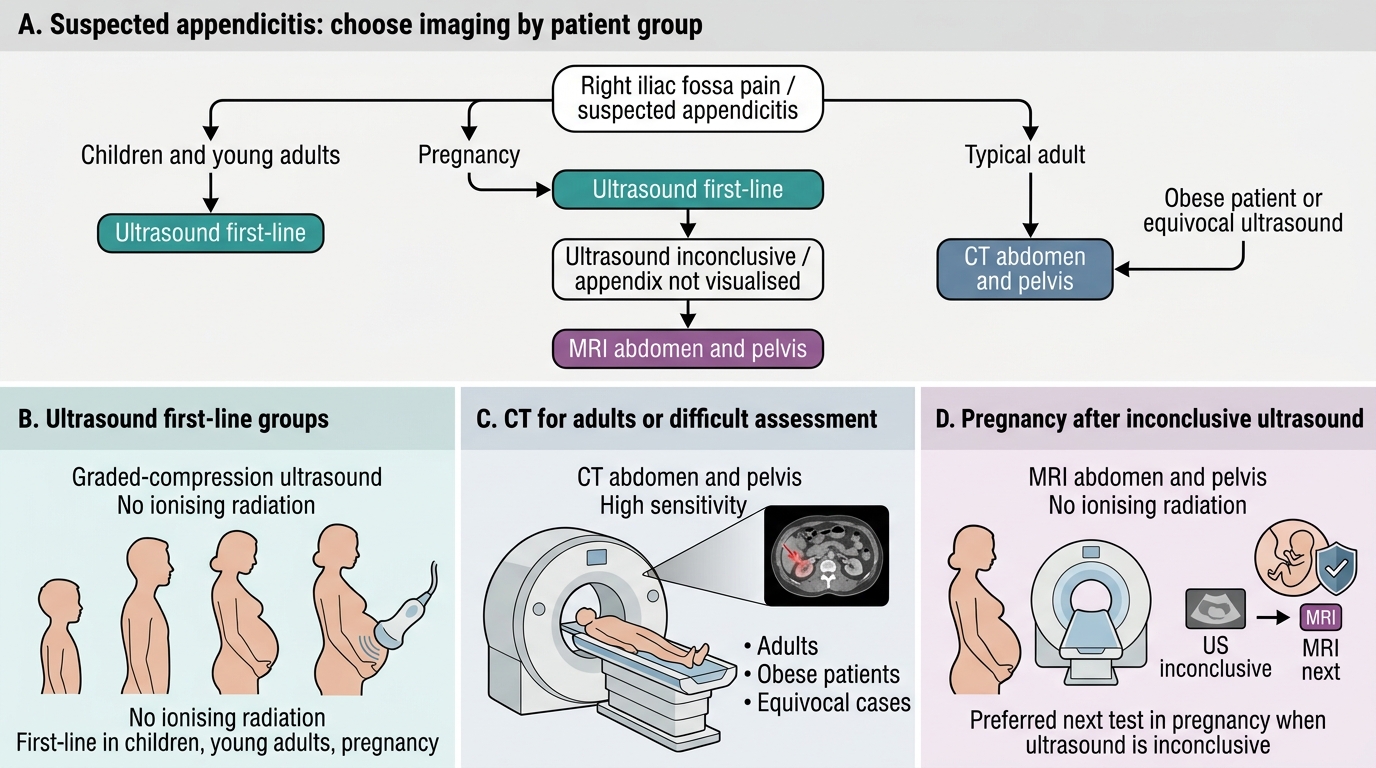
Imaging Pathway for Suspected Appendicitis
SELF-CHECK
A 24-year-old woman at 22 weeks of pregnancy has right-sided abdominal pain suspicious for appendicitis. A graded-compression ultrasound is performed but cannot visualise the appendix and is inconclusive. The surgical team needs to confirm or exclude appendicitis. What is the most appropriate next imaging investigation?
A. Contrast-enhanced CT abdomen and pelvis, as it is the most sensitive test overall
B. MRI abdomen and pelvis, because it avoids ionising radiation to the fetus and can assess the appendix when ultrasound is inconclusive
C. Repeat the same ultrasound daily until the appendix is seen
D. No further imaging; proceed directly to diagnostic laparoscopy in all cases
Reveal Answer
Answer: B. MRI abdomen and pelvis, because it avoids ionising radiation to the fetus and can assess the appendix when ultrasound is inconclusive
In pregnancy, ultrasound is first-line, but when it is inconclusive, MRI is the preferred next investigation because it provides excellent assessment of the appendix without ionising radiation to the fetus. CT, while highly sensitive, exposes the fetus to ionising radiation and is avoided when an alternative exists. Repeating an unhelpful ultrasound wastes time, and proceeding straight to laparoscopy in every inconclusive case is not the standard imaging pathway when MRI can clarify the diagnosis non-invasively.
Imaging Findings — The Inflamed Appendix on Ultrasound and CT
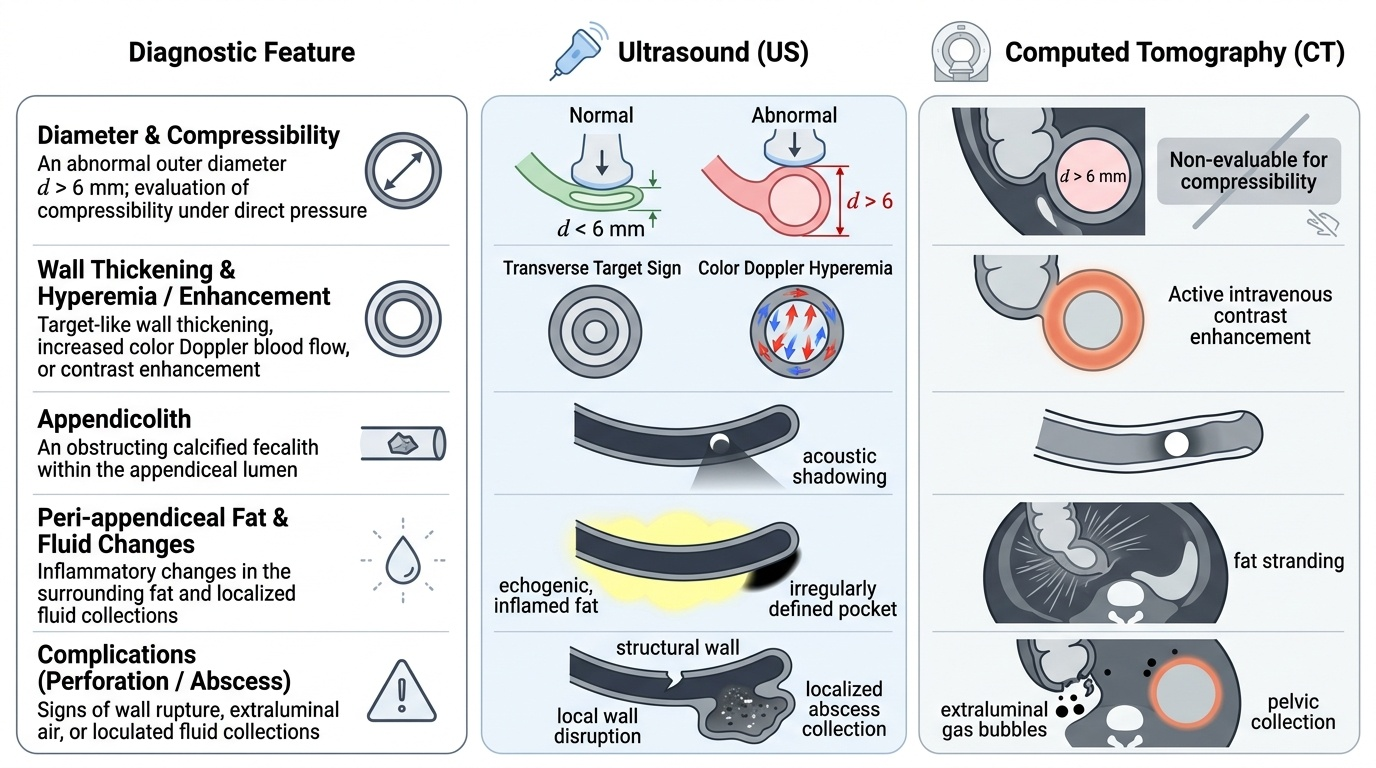
Recognising the inflamed appendix on imaging is a directly applied skill, because the report a clinician acts on is built from a small set of reproducible signs that are worth knowing in their own right. Across both ultrasound and CT the central observation is an abnormally dilated appendix: a normal appendix measures up to about 6 mm in outer diameter, and a diameter greater than 6 mm that is non-compressible and inflamed is the cornerstone finding. Around this central sign cluster the secondary features of inflammation — wall thickening and hyperaemia, peri-appendiceal fluid and fat changes, an obstructing appendicolith — and, critically, the signs of complication that change the operation. The same disease produces a recognisable but modality-specific signature on ultrasound and on CT, so the reader must know both vocabularies and translate confidently between them.
The key ultrasound findings of acute appendicitis are:
- A non-compressible, blind-ending tubular structure in the right iliac fossa arising from the caecum, with an outer diameter greater than 6 mm.
- A target (or 'bull's-eye') sign on transverse section — concentric layers of the inflamed wall.
- An appendicolith (echogenic focus with acoustic shadowing) within the lumen.
- Peri-appendiceal fluid and increased echogenicity of the surrounding fat.
- Increased mural blood flow on colour Doppler (hyperaemia of the inflamed wall).
- Localised tenderness over the appendix during the scan.
The key CT findings of acute appendicitis are:
- A dilated appendix (>6 mm) with a thickened, enhancing wall after intravenous contrast.
- Peri-appendiceal fat stranding (haziness of the surrounding fat from inflammation).
- An appendicolith and free fluid in the right iliac fossa or pelvis.
- Signs of complication: a localised abscess or phlegmon (an inflammatory mass), extraluminal gas or a focal wall defect indicating perforation, and caecal wall thickening.
A normal appendix that is fully visualised, of normal calibre, with no surrounding inflammatory change, argues strongly against appendicitis and may direct attention to an alternative diagnosis. The presence and pattern of complications — particularly whether there is a contained abscess versus free perforation — is exactly the information that determines whether the patient goes to immediate surgery or is managed first by drainage and antibiotics.
Provided image
SELF-CHECK
A graded-compression ultrasound in a 10-year-old with right iliac fossa pain shows a non-compressible, blind-ending tubular structure of 9 mm outer diameter arising from the caecum, with an echogenic shadowing focus in the lumen and increased wall flow on colour Doppler. How do you interpret these findings?
A. Normal appendix; no further action needed
B. Acute appendicitis — a dilated (>6 mm), non-compressible appendix with an appendicolith and mural hyperaemia
C. Mesenteric adenitis with a normal appendix
D. Intussusception of the small bowel
Reveal Answer
Answer: B. Acute appendicitis — a dilated (>6 mm), non-compressible appendix with an appendicolith and mural hyperaemia
A non-compressible, blind-ending tubular structure greater than 6 mm in diameter, with an appendicolith (echogenic shadowing focus) and increased wall flow on Doppler, is diagnostic of acute appendicitis on ultrasound. A normal appendix is compressible and ≤6 mm. Mesenteric adenitis would show enlarged nodes with a normal appendix, and intussusception produces a 'target'/'pseudokidney' mass elsewhere, not a blind-ending tubular structure from the caecum.