Page 8 of 17
RD7.4 | Imaging in Appendicitis — SDL Guide (Part 2)
Impact on Management — Integrating Findings into Surgical Decisions
The integrate (KH) heart of RD7.4 is to turn the imaging picture into a management plan, and in appendicitis the most consequential distinction the imaging draws is between uncomplicated appendicitis, which is treated promptly, and complicated appendicitis (perforation, abscess, phlegmon), which often follows a different, sometimes initially non-operative, pathway. The clinician reads the scan to answer the surgeon's questions: is this appendicitis at all, is it perforated or contained, and is there a drainable collection? Each answer routes the patient differently, and the same scan frequently also excludes or reveals an alternative diagnosis that takes the patient out of the operating theatre entirely.
Pathway 1 — Uncomplicated appendicitis confirmed:
When imaging confirms an inflamed, dilated appendix without perforation or abscess, the standard treatment is appendicectomy (usually laparoscopic), with peri-operative antibiotics. In selected adults with uncomplicated appendicitis, antibiotic-first (non-operative) management is an evidence-supported alternative, and imaging that confirms the absence of an appendicolith and of complications helps select such patients. The imaging finding here confirms the diagnosis and supports timely, definitive treatment.
Pathway 2 — Complicated appendicitis (abscess, phlegmon, perforation):
When imaging shows a contained appendiceal abscess or an inflammatory phlegmon, many surgeons favour initial non-operative management — intravenous antibiotics and, for a sizeable abscess, image-guided (ultrasound- or CT-guided) percutaneous drainage — followed by consideration of an interval appendicectomy weeks later once inflammation has settled. This is a clear instance of imaging directly changing the operative strategy: a contained collection may be drained rather than operated acutely. Free perforation with generalised peritonitis, by contrast, mandates urgent surgery and washout.
Pathway 3 — Normal appendix or an alternative diagnosis:
When the appendix is normal and the scan reveals another cause (ovarian pathology, ureteric calculus, mesenteric adenitis, ileitis), management is redirected accordingly and an unnecessary appendicectomy is avoided — one of the main benefits of pre-operative imaging in equivocal cases, especially in women of reproductive age.
Throughout, the choice of modality made earlier feeds back into this stage: a CT that maps a complication enables a precise plan, whereas a non-visualising ultrasound in a child with persisting symptoms may require either further imaging or a period of active observation before committing to surgery.
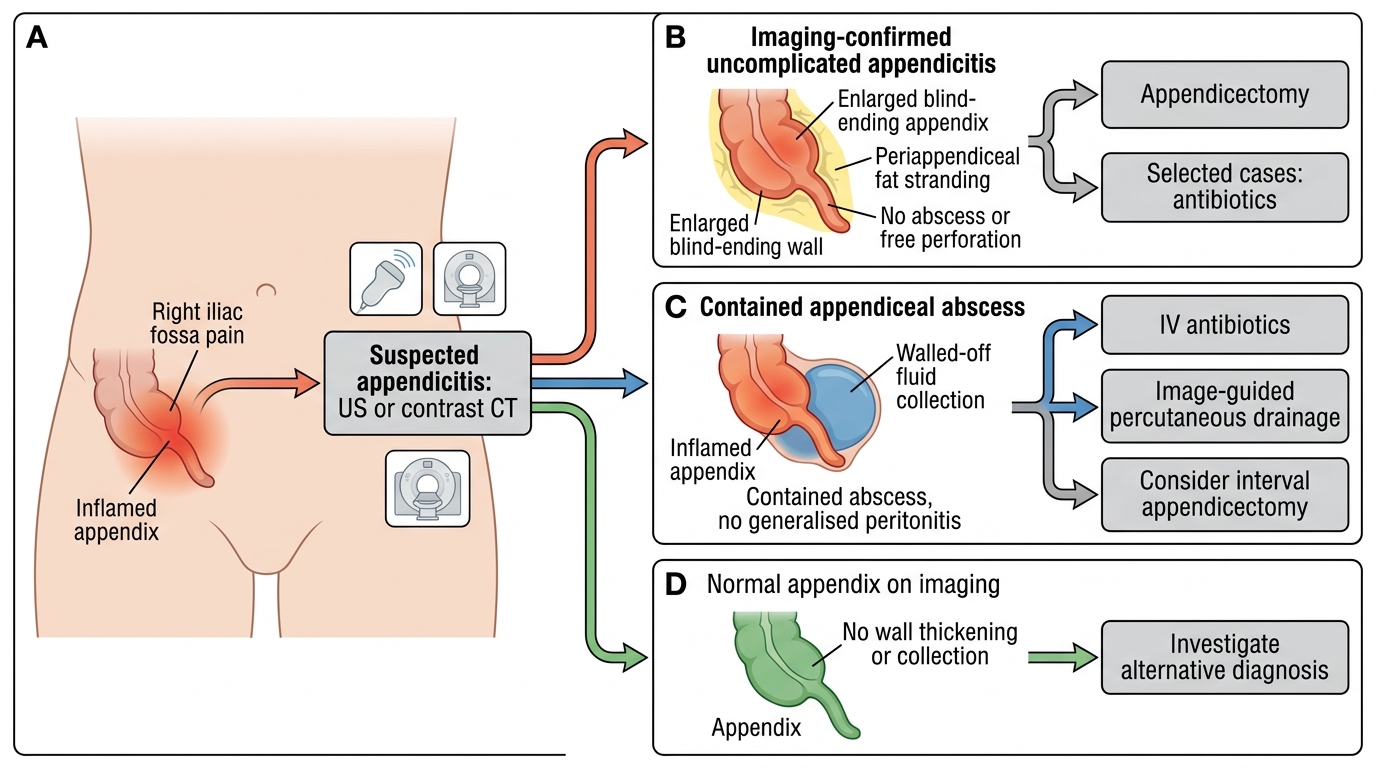
Imaging-Guided Management Pathway for Appendicitis
SELF-CHECK
A 55-year-old man presents late with several days of right iliac fossa pain and a tender mass. Contrast-enhanced CT shows an appendiceal abscess measuring 6 cm, with no free perforation or generalised peritonitis. Integrating these findings, what is a widely accepted initial management approach?
A. Immediate open appendicectomy with extensive resection in all cases
B. Intravenous antibiotics with image-guided percutaneous drainage of the abscess, and consideration of interval appendicectomy later
C. Discharge home on oral antibiotics with no imaging follow-up
D. Urgent laparotomy and washout because all abscesses require emergency surgery
Reveal Answer
Answer: B. Intravenous antibiotics with image-guided percutaneous drainage of the abscess, and consideration of interval appendicectomy later
A contained appendiceal abscess without free perforation or generalised peritonitis is commonly managed initially non-operatively with intravenous antibiotics and image-guided (US- or CT-guided) percutaneous drainage of a sizeable collection, followed by consideration of an interval appendicectomy once inflammation settles. Immediate appendicectomy in a dense inflammatory mass is technically difficult and carries higher morbidity. Free perforation with generalised peritonitis would require urgent surgery, but that is not the case here.
CLINICAL PEARL
Pearl 1 — Match the modality to the patient: Ultrasound first in children, young/thin adults and pregnancy (no radiation); CT in adults, the obese and equivocal cases (most sensitive/specific); MRI in pregnancy when ultrasound is inconclusive (no radiation). This patient-specific logic is the single most examinable point in appendicitis imaging.
Pearl 2 — The 6 mm rule: A non-compressible, blind-ending appendix greater than 6 mm in outer diameter is the cornerstone imaging sign on both ultrasound and CT. Anchor every interpretation to this measurement plus the inflammatory signs around it.
Pearl 3 — A non-visualised appendix is not a normal appendix: Failure to see the appendix on ultrasound (common in the obese or retrocaecal appendix) does NOT exclude appendicitis. If clinical suspicion persists, proceed to further imaging or active observation rather than reassuring the patient.
Pearl 4 — Imaging changes the operation in complicated disease: A contained abscess may be drained and treated with antibiotics (interval appendicectomy later) rather than operated acutely. Reading 'contained collection vs free perforation' on CT directly determines the surgical strategy.
Self-Assessment — Appendicitis Imaging Decisions
Work through these scenarios as the clinician on the surgical or emergency firm, integrating the imaging choice and findings into a management plan before reading the discussion.
Scenario A: An 8-year-old boy has migratory right-iliac-fossa pain, fever and an intermediate clinical probability of appendicitis. The team is unsure and is considering a CT. What imaging do you recommend and why, and what do you look for?
Discussion: In a child, the first-line investigation is graded-compression ultrasound, not CT, because it avoids ionising radiation (ALARA) and is accurate when the appendix is seen. Look for a non-compressible, blind-ending tubular structure greater than 6 mm, an appendicolith, peri-appendiceal fluid and increased Doppler flow. If the ultrasound is positive, proceed to appendicectomy; if it is non-visualising but suspicion persists, the next step is further imaging (e.g. MRI where available, or CT only if necessary) or active observation — a non-visualised appendix does not exclude appendicitis.
Scenario B: A 30-year-old woman has right iliac fossa pain; the differential includes appendicitis and ovarian pathology. Ultrasound shows a normal appendix and a haemorrhagic ovarian cyst. How does this change management?
Discussion: This illustrates a major value of imaging in women of reproductive age. A normal appendix with an identified alternative diagnosis (haemorrhagic ovarian cyst) redirects management away from appendicectomy toward gynaecological management, avoiding an unnecessary operation. The imaging finding of a normal appendix, when the appendix is fully visualised and of normal calibre with no inflammatory change, is reassuring and clinically decisive.
Scenario C: A 60-year-old obese man has 4 days of right-sided abdominal pain and a tender mass. Ultrasound is technically limited by body habitus. Contrast-enhanced CT shows a 5 cm peri-appendiceal abscess with an appendicolith but no free perforation or generalised peritonitis. What is your plan?
Discussion: CT is the appropriate modality here (obese patient, ultrasound limited, complication suspected). The finding of a contained appendiceal abscess without free perforation supports initial non-operative management: intravenous antibiotics and image-guided percutaneous drainage of the abscess, with interval appendicectomy considered later. Integrating the CT directly shapes the strategy — drainage rather than acute appendicectomy of a dense mass — while ongoing monitoring guards against deterioration toward free perforation, which would mandate urgent surgery.