Page 1 of 17
RD7.4 | Imaging in Head Injury — SDL Guide
Learning Objectives
- Apply a validated clinical decision rule (Canadian CT Head Rule / NICE) to decide which head-injury patient requires an emergency CT head.
- Justify non-contrast CT head as the modality of choice for acute traumatic brain injury and state when CT cervical spine and MRI are added.
- Recognise the CT appearances of extradural, subdural, subarachnoid haemorrhage, cerebral contusion and skull fracture, and the signs of mass effect.
- Integrate a described set of imaging findings into the surgical management of a head-injured patient (neurosurgical evacuation vs conservative management).
- Identify the imaging features that mandate urgent neurosurgical referral.
INSTRUCTIONS
Head injury is one of the commonest reasons a surgical or casualty team requests emergency imaging, and the decision is genuinely consequential: an unrecognised expanding extradural haematoma can kill a patient who was talking an hour earlier, while scanning every minor bump wastes resources and irradiates patients needlessly. This module trains you to apply a validated decision rule to choose who is scanned, to understand why non-contrast CT is the first investigation, to read the principal traumatic appearances, and — at the integrate (KH) level demanded by competency RD7.4 — to turn those findings into a surgical management plan.
References
- Sutton's Textbook of Radiology, 6th edition, Chapter on Neuroimaging and Trauma (textbook)
- Grainger & Allison's Diagnostic Radiology, 6th edition, Chapter on Cranial Trauma (textbook)
- NICE NG232 Head injury: assessment and early management (2023) (guideline)
- Stiell IG et al. The Canadian CT Head Rule for patients with minor head injury, Lancet 2001 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 24-year-old man is brought to casualty after falling from a motorcycle. He briefly lost consciousness at the scene but on arrival is fully alert, joking with the paramedics, GCS 15. The surgical houseman is tempted to observe and send him home. Forty minutes later he is found deeply unconscious with a fixed, dilated right pupil. This is the classic 'talk and deteriorate' presentation of an extradural haematoma — arterial blood from a torn middle meningeal artery stripping the dura off the skull, expanding silently behind an initially normal examination. The single decision that changes this story is whether a non-contrast CT head was ordered while the patient still looked well. The imaging request you make in the first quiet hour after a head injury — not the dramatic hour after deterioration — is what saves the brain.
WHY THIS MATTERS
Traumatic brain injury is a leading cause of death and disability in young adults, and in India road-traffic trauma drives an enormous head-injury burden. The surgical and casualty teams you will join as a final-year student and intern carry the front-line responsibility of deciding who needs imaging and who needs a neurosurgeon. Competency RD7.4 requires you to integrate imaging findings into the management of head injuries — not merely to name a haematoma, but to read its shape, size and mass effect and act on it. Over-scanning irradiates and overloads the CT suite; under-scanning misses surgically remediable bleeds. A validated, reproducible decision rule replaces guesswork, and the ability to interpret the resulting scan is the difference between timely craniotomy and a preventable death.
RECALL
Before reading further, recall:
- Meningeal anatomy (from AN): the dura is firmly attached to the skull, especially at sutures. The middle meningeal artery runs in a groove on the inner table of the temporal bone near the pterion and is the classic source of an extradural bleed. The bridging veins cross the subdural space and tear in a subdural bleed.
- CT attenuation physics: fresh clotted blood is hyperdense (bright, ~50–80 Hounsfield units) because protein-rich haemoglobin absorbs X-rays strongly; brain is ~30–40 HU, CSF ~0–15 HU, bone is very bright, and air/fat are dark. This is why acute haemorrhage stands out on non-contrast CT.
- Glasgow Coma Scale (GCS) (from IM/Surgery): eye (4), verbal (5), motor (6) responses, total 3–15; it stratifies severity (mild 13–15, moderate 9–12, severe ≤8) and is the trigger threshold in head-injury imaging rules.
- Monro–Kellie doctrine (from PY): the rigid skull holds a fixed volume; an expanding haematoma raises intracranial pressure, shifts midline structures, and ultimately causes herniation — the anatomical basis of the CT signs of mass effect.
Clinical Scenario — The Head-Injury Call and Who Needs a Scan
The first decision in head injury is not which scan to do but whether to scan at all, and this is precisely where students go wrong — either reflexively scanning every patient or, more dangerously, observing a patient who harbours a surgical bleed. The discipline here is to apply a validated clinical decision rule rather than instinct. Two widely used, well-validated rules govern practice: the Canadian CT Head Rule and the NICE head-injury criteria. Both were derived and validated in large prospective cohorts of patients with minor head injury (GCS 13–15) presenting after blunt trauma with witnessed loss of consciousness, amnesia or disorientation, and both are designed to be highly sensitive for clinically important traumatic brain injury so that the cost of a missed bleed is minimised. The casualty officer applies the rule at the bedside, and a positive criterion converts a 'wait and watch' patient into an 'image now' patient.
The Canadian CT Head Rule identifies high-risk features (mandating CT to exclude a neurosurgical lesion) and medium-risk features (predicting any brain injury on CT):
- High-risk: GCS <15 at 2 hours after injury; suspected open or depressed skull fracture; any sign of basal skull fracture (haemotympanum, 'panda' periorbital bruising, CSF rhinorrhoea/otorrhoea, Battle's sign); two or more episodes of vomiting; age ≥65 years.
- Medium-risk: amnesia for events more than 30 minutes before impact; dangerous mechanism (pedestrian struck, ejection from vehicle, fall from height).
The NICE criteria similarly mandate a CT head within 1 hour for any of: GCS <13 on initial assessment; GCS <15 at 2 hours; suspected open/depressed or basal skull fracture; post-traumatic seizure; focal neurological deficit; more than one episode of vomiting. Patients on anticoagulants with any head injury are also imaged. The unifying principle is that a patient who looks well can still be developing a lethal bleed, so an objective rule — not reassurance from a normal initial examination — decides imaging.
- FAST danger signs that always prompt urgent CT: deteriorating GCS, new focal deficit, unequal or fixed pupils, seizure, or any sign of a basal skull fracture.
- Cervical spine: a significant head injury frequently coexists with a cervical-spine injury — assess for C-spine imaging in the same breath as the head CT.
Imaging Strategy — Why Non-Contrast CT First, Cervical Spine and MRI
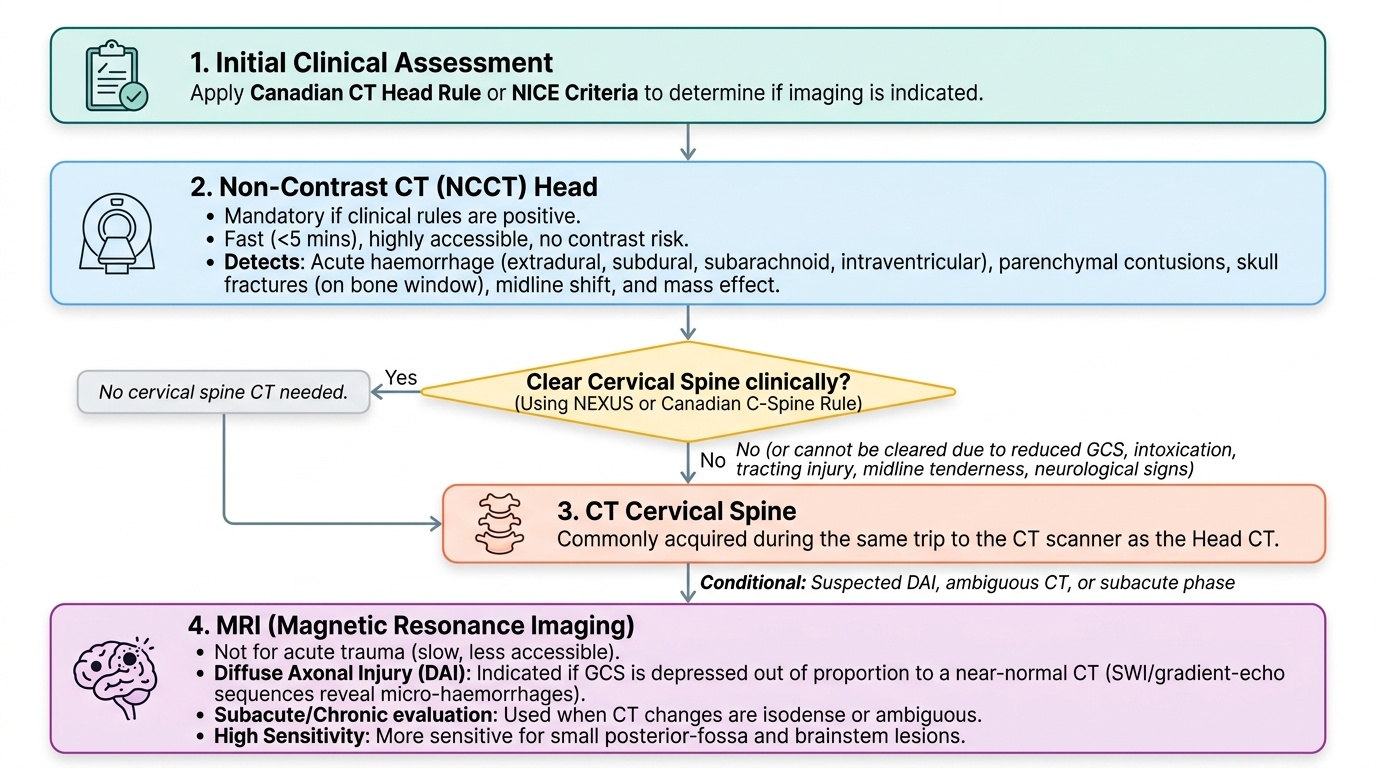
Once a patient meets a criterion for imaging, the modality choice in acute head trauma is settled and almost never debated: non-contrast CT (NCCT) head is the modality of choice. The reasoning is the same logic that drives all acute neuro-imaging — the immediate clinical questions are 'is there blood, a fracture, or mass effect that needs a neurosurgeon now?', and NCCT answers all three faster and more reliably than any alternative. NCCT is available in essentially every emergency department, acquires in under five minutes, requires no contrast (so no delay for renal-function checks and no contrast risk in a potentially unstable trauma patient), and is exquisitely sensitive for acute haemorrhage and for bony injury. Contrast adds nothing in acute trauma and is therefore not used; the bright signal of acute blood is intrinsic and needs no enhancement.
Non-contrast CT head — first-line, mandatory when a rule is positive:
NCCT detects extradural, subdural, subarachnoid and intraventricular haemorrhage, parenchymal contusions, mass effect, midline shift, herniation and skull fractures (reviewed on bone windows). It is reviewed systematically on brain windows (for blood and parenchyma), bone windows (for fractures) and subdural windows (to avoid missing thin collections against the skull).
CT cervical spine — when indicated:
Because blunt head trauma transmits force to the neck, the cervical spine is cleared clinically (e.g. NEXUS or the Canadian C-spine rule) or imaged with CT when the patient cannot be cleared — for example reduced GCS, intoxication, distracting injury, midline tenderness or neurological signs. A head CT and a neck CT are commonly acquired in the same trip to the scanner.
MRI — for diffuse axonal injury and subacute injury:
MRI is not the acute trauma tool — it is slow, less accessible, and harder to perform in an unstable or restless patient. Its role is specific: diffuse axonal injury (DAI), where a patient has a depressed conscious level out of proportion to a near-normal CT (MRI gradient-echo/SWI sequences reveal micro-haemorrhages at grey–white junctions, the corpus callosum and brainstem), and the evaluation of subacute or chronic injury where CT changes have become isodense or ambiguous. MRI is also more sensitive for small posterior-fossa and brainstem lesions where CT suffers beam-hardening artefact.
Provided image
SELF-CHECK
A 30-year-old man with an isolated head injury is GCS 15 and neurologically normal, but his partner reports he is on warfarin for a metallic heart valve. He has no other Canadian CT Head Rule criteria. What is the correct imaging decision?
A. Discharge with head-injury advice as he has no high-risk or medium-risk rule criteria and a normal GCS
B. Arrange a non-contrast CT head because anticoagulation itself is an indication to image after head injury
C. Order an MRI head as it is more sensitive than CT for detecting small bleeds
D. Observe for 4 hours and scan only if the GCS falls
Reveal Answer
Answer: B. Arrange a non-contrast CT head because anticoagulation itself is an indication to image after head injury
Patients on anticoagulants (warfarin, DOACs) who sustain any head injury are at substantially increased risk of delayed intracranial haemorrhage and should have a non-contrast CT head, even when the GCS is 15 and they meet no other rule criterion — this is an explicit indication in NICE guidance. MRI is slower, less available, and not the acute tool; the fast, sensitive investigation for acute blood is NCCT. Simple observation risks missing a bleed that can expand abruptly under anticoagulation.
CT Findings in Head Injury — Reading the Traumatic Brain
Interpreting the head-injury CT is a core skill, because the management pathway pivots directly on the pattern, size and mass effect of what you see — and the junior doctor is often the first to view the images overnight. Traumatic intracranial haemorrhage takes several characteristic forms, and they are distinguished by their shape, their relationship to the skull sutures and the midline, and their typical cause. All acute traumatic blood is hyperdense (bright, ~50–80 HU) on the initial scan; over days it becomes isodense and then hypodense, which is why timing matters in interpretation. Beyond the blood itself, the clinician must read the secondary signs — effacement of sulci and ventricles, midline shift, and herniation — because these signs of raised intracranial pressure are frequently what determine surgical urgency, sometimes more than the volume of blood itself.
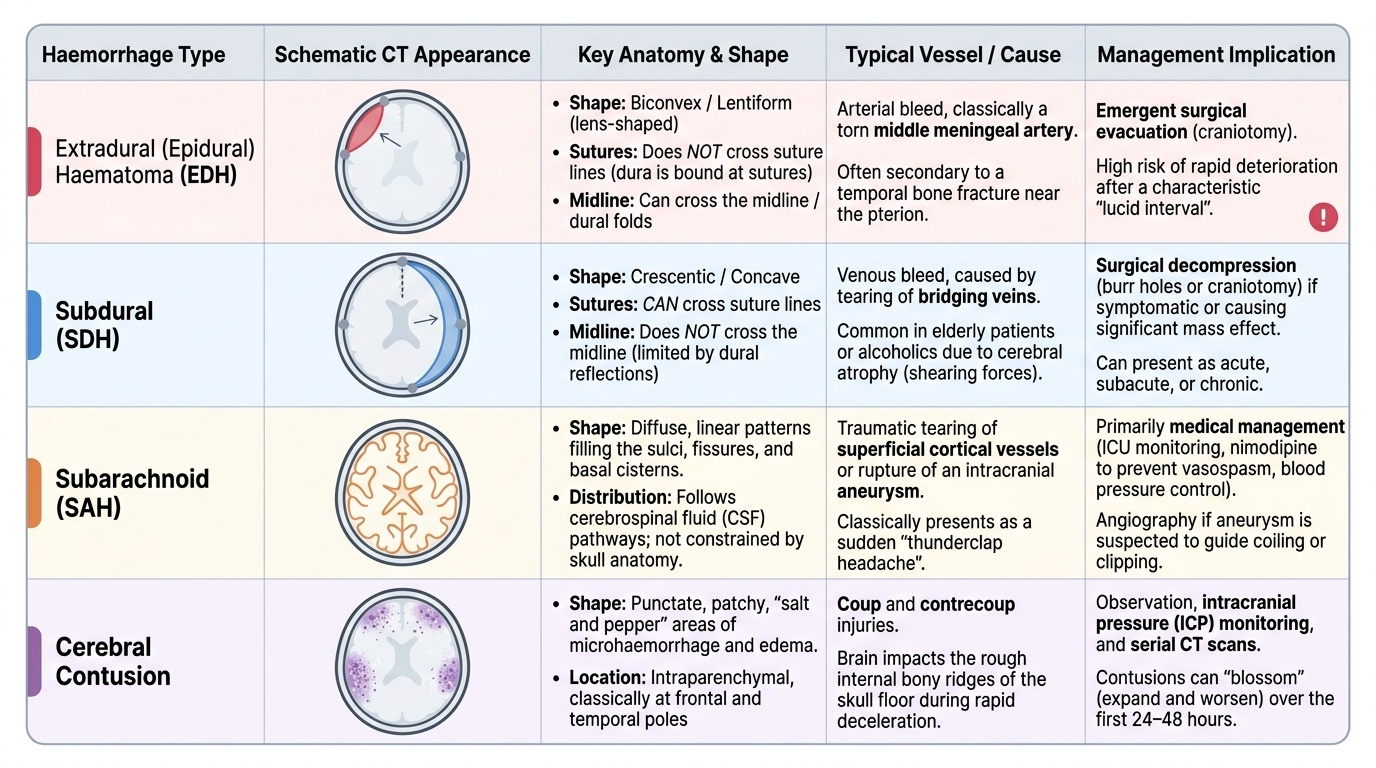
The principal traumatic appearances are:
- Extradural (epidural) haematoma (EDH): a biconvex (lentiform/lens-shaped) hyperdense collection between the skull and dura that does NOT cross suture lines (the dura is bound at sutures) but can cross the midline. Classically arterial, from a torn middle meningeal artery after temporal-bone fracture near the pterion. The 'lucid interval' followed by deterioration is its clinical signature; it is the most time-critical surgical emergency.
- Subdural haematoma (SDH): a crescentic (concave) hyperdense collection between the dura and arachnoid that crosses suture lines but NOT the midline (the falx limits it). Usually venous, from torn bridging veins; common in the elderly and in shaken/decelerated brains. Acute SDH is hyperdense; chronic SDH becomes hypodense; subacute may be isodense and easily missed.
- Traumatic subarachnoid haemorrhage (SAH): hyperdensity tracking along the sulci, fissures and basal cisterns; common after significant trauma.
- Cerebral contusion: patchy 'salt-and-pepper' areas of haemorrhage and oedema in the cortex, classically at the frontal and temporal poles (coup and contre-coup); may blossom (enlarge) over 24–48 hours.
- Skull fracture: a lucent line on bone windows; a depressed fracture (inward bone fragments) or an open fracture needs surgical assessment; a basal skull fracture may show air (pneumocephalus) or fluid levels.
- Mass effect / midline shift / herniation: sulcal and ventricular effacement, shift of the septum pellucidum across the midline, and the cisternal changes of uncal or subfalcine herniation — the radiological emergencies.
Provided image
SELF-CHECK
A 19-year-old struck on the temple has a non-contrast CT showing a biconvex (lens-shaped) hyperdense collection over the right temporal region that does not cross the coronal suture, with an adjacent temporal-bone fracture. Which lesion is this and what is its classic source?
A. Subdural haematoma from torn bridging veins
B. Extradural haematoma from the middle meningeal artery
C. Traumatic subarachnoid haemorrhage from cortical vessels
D. Chronic subdural haematoma from atrophy-related vein stretching
Reveal Answer
Answer: B. Extradural haematoma from the middle meningeal artery
A biconvex (lentiform) hyperdense collection that does NOT cross suture lines, associated with a temporal-bone fracture, is the classic extradural (epidural) haematoma, typically arterial from a torn middle meningeal artery at the pterion. A subdural haematoma is crescentic, crosses sutures but not the midline, and is usually venous from bridging veins. Recognising the biconvex shape and the temporal fracture is critical because an arterial EDH can expand rapidly and is a neurosurgical emergency.