Page 2 of 17
RD7.4 | Imaging in Head Injury — SDL Guide (Part 2)
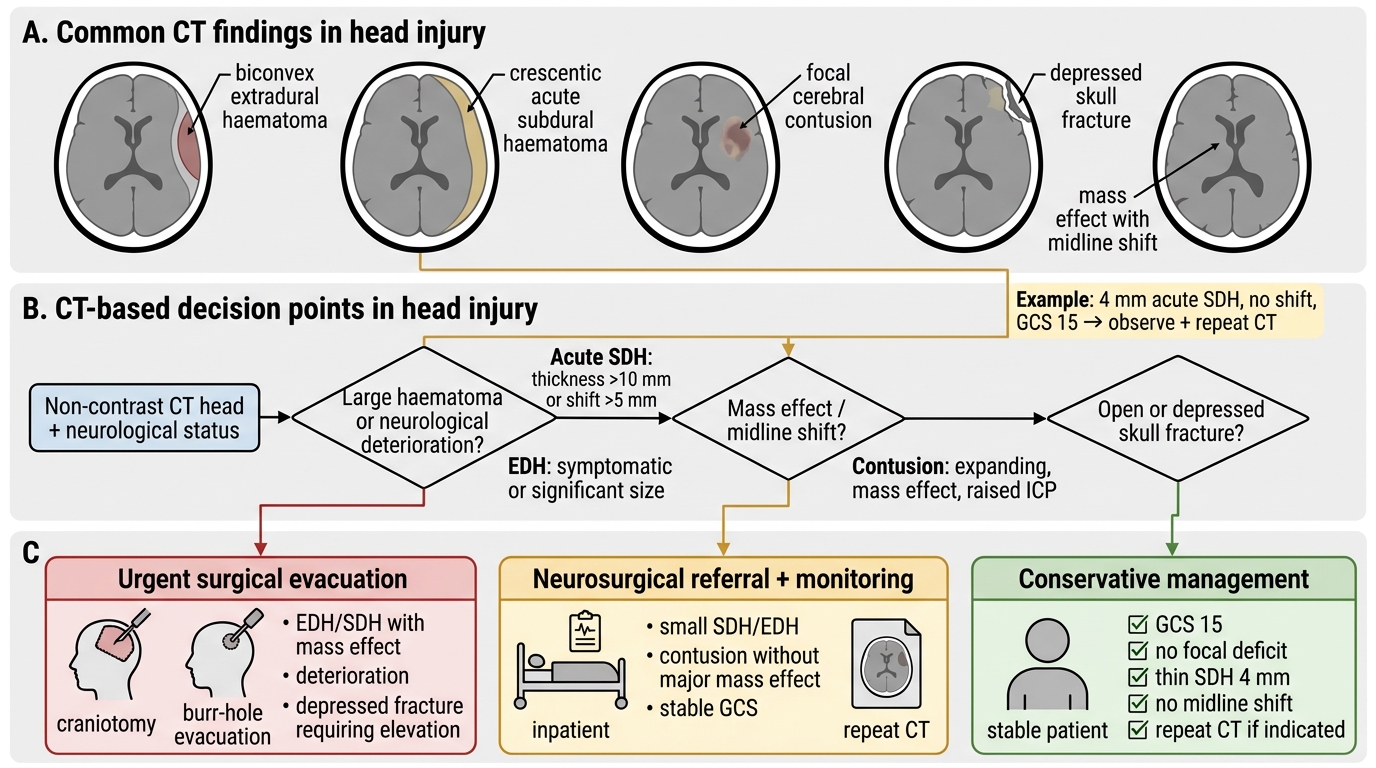
Impact on Management — Integrating Findings into Surgical Decisions
This is the integrate (KH) heart of competency RD7.4: given a described set of CT findings, the clinician must construct a management plan, because in head injury the imaging report and the surgical decision are almost the same act. The CT does not merely label a lesion — it sizes it, locates it, and quantifies its mass effect, and each of those numbers feeds a specific management threshold. The applied skill is to read a finding and immediately ask: does this need theatre now, neurosurgical referral and close observation, or conservative management with a repeat scan? Three broad pathways follow from the imaging, and the same scan often informs all three at once because trauma patients harbour mixed injuries.
Pathway 1 — Urgent surgical evacuation (craniotomy):
An extradural haematoma with significant volume or any neurological deterioration is the prototypical surgical emergency — arterial bleeding expands fast, and early evacuation in a patient who has not yet herniated gives excellent outcomes, which is why the 'talk and deteriorate' patient must reach theatre quickly. A large acute subdural haematoma (commonly cited surgical thresholds are a clot thickness greater than ~10 mm or a midline shift greater than ~5 mm, or any clot with a depressed conscious level) is evacuated. A depressed skull fracture that is open, or significantly depressed below the inner table, needs surgical elevation and debridement. Mass effect with herniation on CT is an immediate call to the neurosurgeon.
Pathway 2 — Neurosurgical referral, monitoring and medical control of intracranial pressure:
Smaller haematomas, contusions and traumatic SAH without surgical mass effect are admitted for neurological observation, often with intracranial-pressure monitoring in severe injury (GCS ≤8). Medical measures protect the brain while it is watched: head-up positioning, maintenance of oxygenation and blood pressure to preserve cerebral perfusion, avoidance of hyponatraemia, treatment of seizures, and urgent reversal of anticoagulation (e.g. prothrombin complex concentrate and vitamin K for warfarin) when a bleed is present. Contusions in particular may 'blossom', so a repeat CT at 6–24 hours, or sooner if the patient deteriorates, is standard.
Pathway 3 — Conservative management with safety-netting:
A patient with a normal CT and a recovered GCS who meets discharge criteria can go home with written head-injury advice and a responsible adult, because a normal acute CT has a high negative predictive value for a lesion needing surgery. The caveat is the anticoagulated patient and the patient with persistent symptoms, for whom a period of observation or a delayed scan is prudent.
What CT cannot do: a normal CT does not exclude diffuse axonal injury — a patient with a depressed conscious level and a near-normal CT needs MRI. CT also underestimates very early or small contusions that later blossom, which is the rationale for repeat imaging in the deteriorating patient.
CT-Based Head-Injury Management Pathway
SELF-CHECK
A 72-year-old on no anticoagulants falls and has a CT showing a 4 mm-thick crescentic acute subdural haematoma over the left hemisphere with no midline shift; he is GCS 15 with no focal deficit. Integrating these findings, what is the most appropriate management?
A. Immediate craniotomy regardless of size because all acute subdural haematomas are evacuated
B. Admit for neurological observation with conservative management and a repeat CT, reserving surgery for clot >~10 mm, midline shift >~5 mm, or deterioration
C. Discharge home immediately as the GCS is 15
D. Start anticoagulation to prevent venous thrombosis
Reveal Answer
Answer: B. Admit for neurological observation with conservative management and a repeat CT, reserving surgery for clot >~10 mm, midline shift >~5 mm, or deterioration
A thin (4 mm) acute subdural haematoma without midline shift in a neurologically intact patient is managed conservatively with admission, observation and a repeat scan; surgical evacuation is reserved for clot thickness greater than about 10 mm, midline shift greater than about 5 mm, or any neurological deterioration. Immediate craniotomy is not indicated for every acute subdural haematoma. Discharging an elderly patient with an acute intracranial bleed is unsafe, and starting anticoagulation in the presence of fresh intracranial haemorrhage would be dangerous.
CLINICAL PEARL
Pearl 1 — Biconvex vs crescentic: Lock in the shape rule. Extradural = biconvex (lens), does NOT cross sutures (arterial, middle meningeal artery). Subdural = crescentic, crosses sutures but NOT the midline (venous, bridging veins). This single distinction is the most examinable and most clinically useful fact in trauma neuroimaging.
Pearl 2 — The lucid interval is a warning, not reassurance: A head-injury patient who is currently talking and well can be in the lucid interval of an expanding extradural bleed. Apply the decision rule and scan the at-risk patient while they look well — the deterioration, when it comes, is abrupt.
Pearl 3 — Normal CT does not exclude DAI: When the conscious level is far worse than the CT appearance suggests, think diffuse axonal injury and request MRI (gradient-echo/SWI). A 'normal' acute CT in a deeply unconscious patient is itself an abnormal finding that demands explanation.
Pearl 4 — Always anticoagulant-check and C-spine: Any anticoagulated head injury is scanned; any significant head injury raises the question of a coexisting cervical-spine injury. Make both checks reflexive.
Self-Assessment — Head-Injury Imaging Decisions
Work through these scenarios as the surgical or casualty doctor on call. Write your reasoning, integrating the imaging findings into a management plan, before reading the discussion.
Scenario A: A 21-year-old assaulted with a blow to the side of the head had a brief loss of consciousness, then was fully alert (GCS 15) for an hour, and has now become drowsy (GCS 12) with a sluggish right pupil. What imaging do you order, what finding do you expect, and what is the management?
Discussion: This is the classic lucid-interval presentation of an extradural haematoma. Order an urgent non-contrast CT head (and assess the C-spine). Expect a biconvex hyperdense collection that does not cross sutures, likely temporal with an associated fracture, from the middle meningeal artery. Integrating the deteriorating GCS, the dilating pupil and the expanding arterial bleed, this is an immediate neurosurgical emergency requiring urgent craniotomy and evacuation — alert the neurosurgeon before the scan if necessary.
Scenario B: An 80-year-old on warfarin (for atrial fibrillation) has a minor fall, hits her head, and is GCS 15 with no focal deficit. The houseman wants to discharge her. What do you do, and why?
Discussion: Do not discharge. Anticoagulation is itself an indication for a non-contrast CT head after any head injury, because warfarin substantially raises the risk of delayed intracranial haemorrhage and an elderly brain bleeds readily (the same population at risk of subdural haematoma from bridging-vein tears). If the CT shows blood, integrate the finding into management: admit, reverse the warfarin urgently (prothrombin complex concentrate and vitamin K), neurosurgical referral, and a repeat scan. If the CT is normal, a period of observation is prudent given the anticoagulation.
Scenario C: A 34-year-old ejected from a car is deeply unconscious (GCS 6) on arrival. The non-contrast CT head is reported as showing only minor scattered punctate high-densities at the grey–white junction and in the corpus callosum, with no large haematoma and no significant mass effect. The conscious level seems far worse than the CT. How do you reconcile this, and what is the next imaging step?
Discussion: The mismatch between a profoundly depressed GCS and a near-normal CT is the signature of diffuse axonal injury (DAI) from rotational/shearing forces in high-energy trauma; the punctate haemorrhages at the grey–white junction and corpus callosum are the visible tip of widespread axonal damage. The next imaging step is MRI (gradient-echo/SWI and DWI), which is far more sensitive for DAI. Management is supportive neuro-intensive care with intracranial-pressure control; there is no clot to evacuate, and the prognosis is determined by the extent of axonal injury.