Page 4 of 17
RD7.4 | Imaging in Strangulated Hernia — SDL Guide
Learning Objectives
- Recognise that strangulation of a hernia is primarily a clinical diagnosis and state when imaging adds value.
- Justify the choice between bedside ultrasound and contrast-enhanced CT abdomen/pelvis in suspected strangulated hernia.
- Identify the CT and ultrasound findings of bowel ischaemia, closed-loop obstruction and complications.
- Integrate described imaging findings into the emergency surgical management of a strangulated hernia.
- Distinguish, by imaging, a strangulated (ischaemic) hernia from a simple incarcerated (viable) hernia.
INSTRUCTIONS
A strangulated hernia is a surgical emergency in which the blood supply to the herniated contents is compromised, and delay leads to bowel infarction, perforation, peritonitis and death. The diagnosis is fundamentally clinical — a tense, tender, irreducible hernia with obstruction — and the surgeon must not delay theatre to chase a scan in an obvious case. But imaging has a defined role: in the equivocal patient, in mapping complications, and in confirming bowel viability. This module, aligned to competency RD7.4, trains you to choose the right investigation, read the signs of ischaemia, and integrate them into an emergency operative decision.
References
- Sutton's Textbook of Radiology, 6th edition, Chapter on the Acute Abdomen (textbook)
- Grainger & Allison's Diagnostic Radiology, 6th edition, Chapter on the Gastrointestinal Tract and Bowel Obstruction (textbook)
- Bailey & Love's Short Practice of Surgery, Chapter on Hernias (clinical correlation) (guideline)
- World Society of Emergency Surgery (WSES) guidelines on emergency repair of complicated abdominal wall hernias (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 68-year-old man comes to casualty with 12 hours of central abdominal pain, vomiting and a painful lump in his right groin that he 'usually pushes back in' but today cannot. The lump is tense, exquisitely tender, and the overlying skin is reddened. He has not passed flatus since the pain began. The surgical resident's reflex is to send him for a CT to 'confirm'. But the clinical picture — an irreducible, tender hernia with bowel obstruction — already names the diagnosis: this is a strangulated hernia, and the blood supply to the trapped bowel is being choked off minute by minute. The right call is to resuscitate and take him to theatre, not to delay for imaging the diagnosis is already shouting. Knowing when imaging helps, and when it merely wastes ischaemic time, is the skill this module teaches.
WHY THIS MATTERS
Groin and abdominal-wall hernias are among the commonest surgical conditions, and strangulation is their most feared complication because compromised blood supply converts a routine elective repair into a life-threatening emergency. As a final-year student and intern on the surgical firm, you will be the first to examine these patients and the first to decide whether to call the registrar and whether to request imaging. Competency RD7.4 requires you to integrate imaging findings into the management of a hernia with strangulation — to understand that imaging confirms ischaemia, maps complications such as closed-loop obstruction, and distinguishes a dead loop from a merely trapped but viable one. Getting this right shortens the time to a life-saving operation; getting it wrong — by over-relying on a scan in an obvious case — costs bowel and sometimes life.
RECALL
Before reading further, recall:
- Hernia terminology (from Surgery): a hernia is reducible if the contents return to the abdomen; irreducible (incarcerated) if they cannot be reduced but remain viable; and strangulated when the blood supply to the contents is compromised, causing ischaemia. Strangulation is the dangerous step beyond incarceration.
- Groin hernia anatomy (from AN): inguinal hernias pass through the inguinal canal (the neck above and medial to the pubic tubercle); femoral hernias pass below and lateral to the pubic tubercle through the narrow, rigid femoral ring and are therefore especially prone to strangulation.
- Bowel ischaemia (from PY/Pathology): obstruction of venous then arterial flow leads to wall oedema, mucosal then transmural infarction, loss of peristalsis, and finally perforation. Reperfusion and bacterial translocation drive sepsis. Ischaemic bowel does not enhance with intravenous contrast.
- CT contrast enhancement: normal bowel wall takes up intravenous iodinated contrast and 'enhances' (brightens). Absent or reduced enhancement of a bowel loop is the key CT sign that its blood supply is compromised.
Clinical Scenario — The Tender Irreducible Hernia
The decisive first point — and the one most likely to be tested and most likely to be got wrong in practice — is that strangulation of a hernia is a clinical diagnosis, and a patient with an obviously strangulated hernia should go to theatre after resuscitation, not into a CT scanner. The clinical hallmark is an irreducible, tense, exquisitely tender hernia, often with overlying erythema, accompanied by features of bowel obstruction (colicky central abdominal pain, vomiting, distension, absolute constipation) and, as ischaemia advances, signs of systemic compromise (tachycardia, fever, peritonism). When all of these are present, imaging confirms what the bedside already knows and serves mainly to delay a time-critical operation; the surgical teaching is unambiguous that a clear strangulation is taken to theatre.
Where, then, does imaging earn its place? Imaging is genuinely useful in defined situations:
- The equivocal patient: an obese patient in whom the groin is hard to examine, an irreducible hernia that is not obviously tender, or a patient with abdominal obstruction but no obvious external hernia (an internal or obturator hernia, easily missed clinically).
- Mapping complications and viability: confirming closed-loop obstruction, demonstrating ischaemia by absent enhancement, and identifying free fluid, perforation or other intra-abdominal pathology that changes the operative plan.
- Distinguishing strangulation from simple incarceration: an irreducible but viable (incarcerated) hernia may be managed differently from a frankly ischaemic one, and imaging can support that distinction when the clinical picture is unclear.
The governing principle is therefore one of judgement: in the clear-cut strangulation, do not let imaging delay the operation; in the uncertain case, a focused investigation answers the questions that change management. Femoral hernias deserve a special mention — they are smaller, harder to feel, more common in older women, and far more likely to strangulate, so a low threshold for imaging and for surgery applies.
Imaging Strategy — Ultrasound at the Bedside, CT for Confirmation
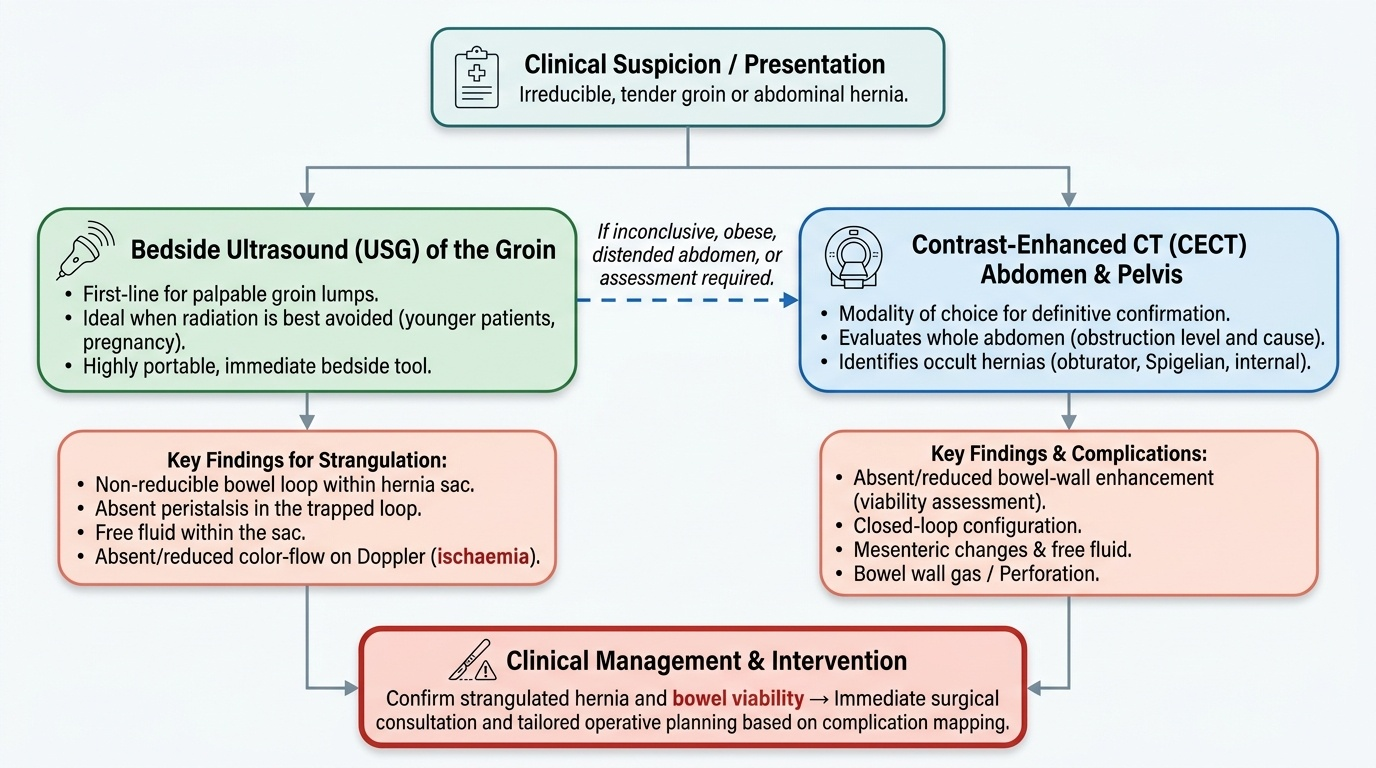
When imaging is indicated, the choice lies principally between bedside ultrasound (USG) and contrast-enhanced CT abdomen and pelvis, and the selection follows the same modality logic used throughout acute imaging: what is the question, how fast and how accessible is the answer, and what does the patient's situation permit. Ultrasound is immediate, portable, radiation-free and excellent at the groin; CT is the comprehensive 'map everything' study and is the modality of choice when the whole abdomen must be assessed for the level, cause and complications of obstruction. The two are complementary rather than competing, and many patients begin with a focused ultrasound and proceed to CT when broader assessment is required.
Ultrasound (USG) — bedside, first-line for the groin:
USG is particularly valuable for the groin lump and in patients in whom radiation is best avoided (younger patients, pregnancy). It can demonstrate a non-reducible bowel loop within the hernia sac, absent peristalsis in the trapped loop (a sign that it is no longer functioning), free fluid within the sac, and — using colour Doppler — absent or reduced colour-flow in the bowel wall, which signals ischaemia. Its limitations are operator dependence and difficulty in the obese or very distended abdomen.
Contrast-enhanced CT abdomen/pelvis — modality of choice for confirmation and complication mapping:
CT is the most sensitive and specific investigation for confirming a strangulated hernia and for mapping its complications. With intravenous contrast it directly assesses bowel-wall enhancement (the single most important sign of viability), and it defines the level and cause of obstruction, demonstrates closed-loop configuration, free fluid, mesenteric changes and perforation. CT also detects clinically occult hernias (obturator, Spigelian, internal) that explain an obstruction with no obvious external lump. Iodinated contrast is used to assess enhancement; in a patient with poor renal function this is weighed against the diagnostic need, but in a surgical emergency the information usually justifies it.
A plain abdominal X-ray may show dilated bowel loops and air–fluid levels confirming obstruction, but it cannot assess viability and does not replace CT; its role is limited in this context.
Provided image
SELF-CHECK
A 70-year-old woman has a small, tender, irreducible lump below and lateral to the pubic tubercle and signs of small-bowel obstruction. The surgeon is confident this is a strangulated femoral hernia. What is the most appropriate course of action?
A. Delay surgery to obtain a contrast CT to absolutely confirm strangulation before operating
B. Resuscitate and proceed to emergency surgery, as a clinically strangulated hernia is an operative emergency and imaging should not delay theatre
C. Attempt vigorous manual reduction of the hernia in the emergency department first
D. Discharge with analgesia and arrange an outpatient ultrasound
Reveal Answer
Answer: B. Resuscitate and proceed to emergency surgery, as a clinically strangulated hernia is an operative emergency and imaging should not delay theatre
A clinically obvious strangulated hernia — irreducible, tender, with obstruction — is a surgical emergency; the patient should be resuscitated and taken to theatre without delaying for confirmatory imaging. Strangulation is a clinical diagnosis and a CT in this setting only wastes ischaemic time. Vigorous reduction of a strangulated hernia is dangerous (it can reduce dead bowel into the abdomen — 'reduction en masse'). Femoral hernias are especially prone to strangulation and must not be sent home.
Imaging Findings — Recognising Bowel Ischaemia and Closed-Loop Obstruction
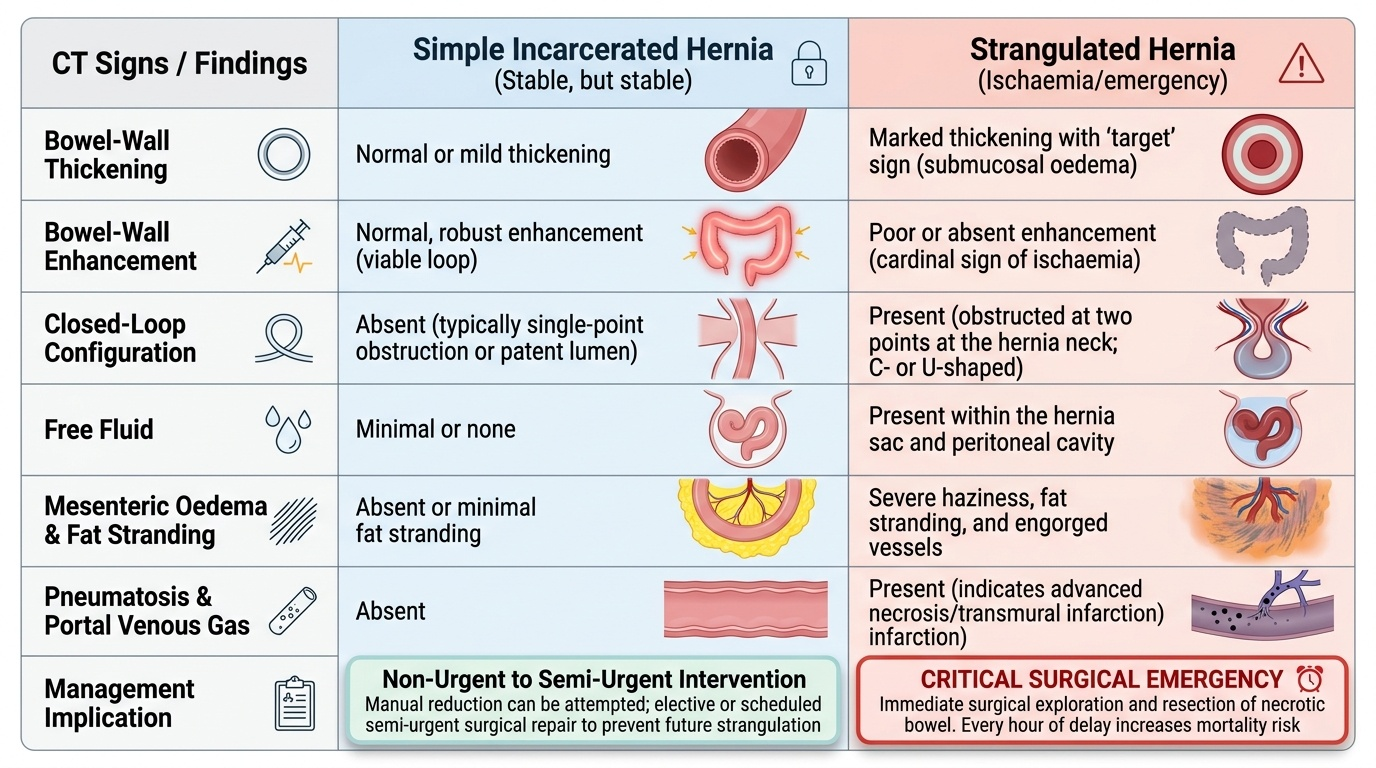
When a scan is obtained, the interpretive task is to answer two linked questions: is this bowel obstructed in a closed loop, and is it ischaemic? The findings that answer them are the same ones that drive the surgeon's urgency, so reading them is a directly applied skill rather than an academic exercise. On contrast-enhanced CT the most important single observation is the enhancement of the bowel wall: a viable loop brightens with intravenous contrast, whereas an ischaemic loop shows poor or absent enhancement — the most reliable sign that the bowel is dying. Around this central sign cluster a constellation of supportive findings, and the more of them that are present, the higher the likelihood of strangulation and the greater the urgency.
The key CT findings in a strangulated hernia are:
- Bowel-wall thickening: the trapped, congested loop thickens from oedema; it may show a 'target' appearance.
- Poor or absent bowel-wall enhancement: the cardinal sign of ischaemia — the loop fails to take up intravenous contrast.
- Closed-loop obstruction: a segment obstructed at two points (the hernia neck), seen as a C- or U-shaped fluid-filled loop with converging mesenteric vessels at the constriction — a configuration that is intrinsically prone to ischaemia.
- Free fluid: fluid within the hernia sac and in the peritoneal cavity, increasing with ischaemia.
- Mesenteric oedema and fat stranding: haziness and engorgement of the mesentery around the trapped loop, with engorged mesenteric vessels.
- Pneumatosis intestinalis and portal venous gas: gas within the bowel wall, and gas tracking into the portal veins — late, ominous signs of established transmural infarction.
- Free intraperitoneal gas: indicates perforation.
On ultrasound, the corresponding signs are a non-reducible loop within the sac, absent peristalsis, free fluid in the sac, a thickened bowel wall, and absent colour-flow on Doppler indicating loss of perfusion. By contrast, a simple incarcerated (viable) hernia shows a trapped loop that still enhances normally, with preserved wall and little or no free fluid — the imaging counterpart of bowel that is trapped but alive.
Provided image
SELF-CHECK
A contrast-enhanced CT in a patient with an irreducible inguinal hernia shows a C-shaped fluid-filled small-bowel loop within the sac that does NOT enhance, with surrounding free fluid and mesenteric fat stranding. What do these findings indicate?
A. A simple incarcerated but viable hernia that can be managed conservatively
B. A strangulated hernia with bowel ischaemia and closed-loop obstruction requiring emergency surgery
C. An uncomplicated reducible hernia that needs only elective repair
D. Normal post-prandial bowel appearance of no clinical significance
Reveal Answer
Answer: B. A strangulated hernia with bowel ischaemia and closed-loop obstruction requiring emergency surgery
Absent bowel-wall enhancement is the cardinal CT sign of ischaemia; combined with a closed-loop (C-shaped) configuration, free fluid and mesenteric fat stranding, this is a strangulated hernia with a non-viable loop — an emergency requiring urgent operation, likely with resection of the dead segment. A simple incarcerated hernia would still ENHANCE normally with preserved wall and minimal free fluid. These findings cannot represent a reducible or normal hernia.