Page 5 of 17
RD7.4 | Imaging in Strangulated Hernia — SDL Guide (Part 2)
Impact on Management — Integrating Findings into Emergency Surgery
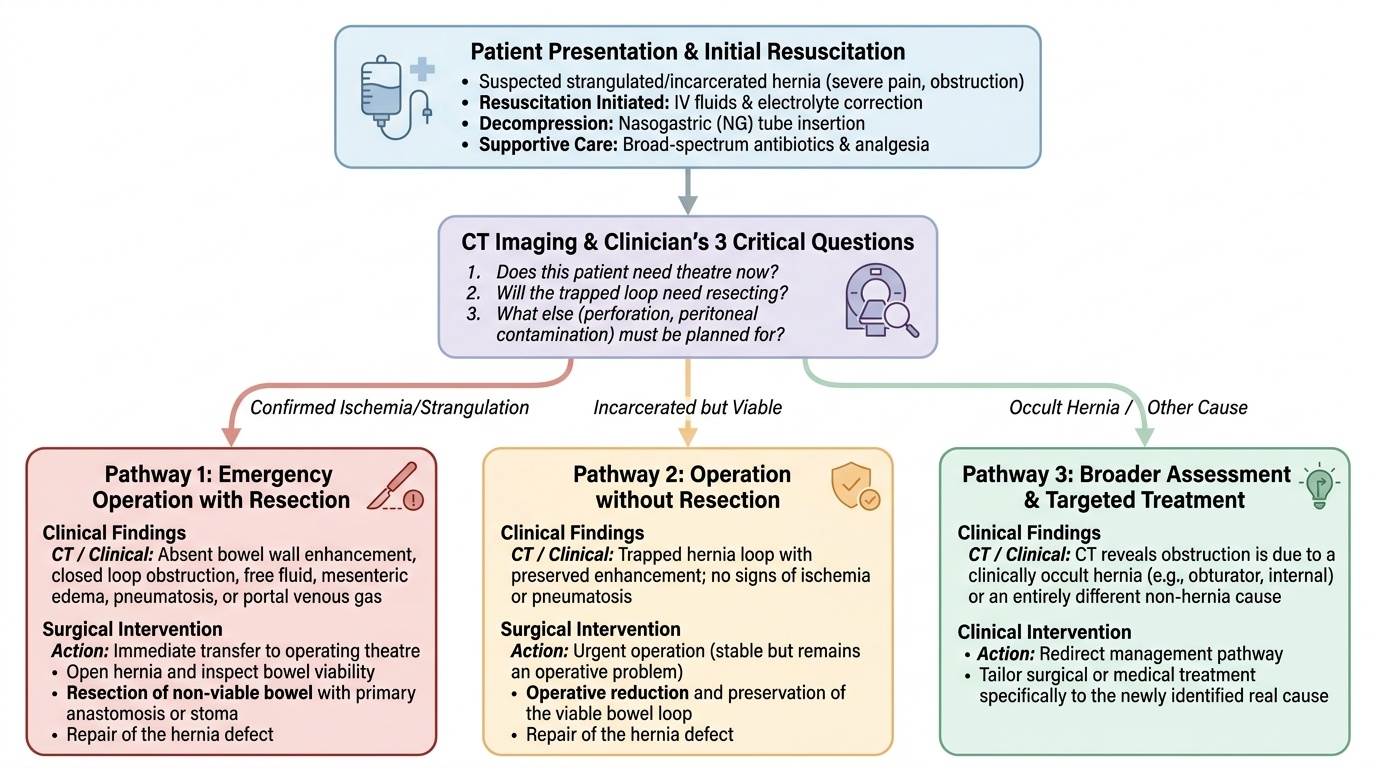
The integrate (KH) core of RD7.4 is to convert the imaging picture into an operative plan, and in a strangulated hernia the link between finding and action is short and sharp: signs of ischaemia mean the bowel may be dead and the patient needs an emergency operation, while preserved viability changes the timing and the extent of surgery. The clinician reads the scan not to admire it but to answer the surgeon's three questions — does this patient need theatre now, will the trapped loop need resecting, and what else (perforation, peritoneal contamination) must be planned for? The management pathways below all begin from resuscitation, because these are sick patients with fluid and electrolyte losses from obstruction and often with sepsis.
Pathway 1 — Emergency operation with resection (ischaemia/strangulation confirmed):
When the clinical picture or imaging shows ischaemia — absent enhancement, a closed loop, free fluid, mesenteric oedema, and especially pneumatosis or portal venous gas — the patient needs an urgent operation. At surgery the hernia is opened, the trapped bowel inspected for viability, and non-viable bowel is resected with primary anastomosis or stoma as appropriate, after which the defect is repaired. Pre-operative resuscitation (intravenous fluids, correction of electrolytes), a nasogastric tube to decompress the obstructed bowel, broad-spectrum antibiotics, and analgesia accompany the decision to operate. The imaging finding of frank infarction does not change the destination (theatre) but does prepare the team to resect.
Pathway 2 — Operation without resection (irreducible/incarcerated but viable):
When imaging shows a trapped loop that still enhances and there are no ischaemic features, the bowel is likely viable; the patient still usually needs an operation to relieve the obstruction and repair the hernia, but the trapped loop may be reduced and preserved rather than resected. Timing may be slightly less frantic than in frank strangulation, but an irreducible obstructed hernia is still an operative problem.
Pathway 3 — Resuscitation, broader assessment, and treating the real cause:
When CT reveals that the obstruction is due to a clinically occult hernia (obturator, internal) or to an entirely different cause, management is directed accordingly. In all cases imaging that demonstrates perforation (free intraperitoneal gas) or established peritonitis mandates urgent surgery and intensive resuscitation.
A crucial safety point integrating imaging and clinical care: never attempt forceful manual reduction of a strangulated hernia, because reducing dead bowel back into the abdomen ('reduction en masse') hides the infarcted loop and leads to delayed perforation and peritonitis — a trap that imaging may then reveal too late.
Provided image
SELF-CHECK
A patient with a strangulated hernia is being prepared for theatre. While waiting, the intern considers firmly pushing the tense, tender hernia back to relieve the patient's pain. Why is this dangerous, and what does subsequent imaging often reveal if it is done?
A. It is safe and recommended as it relieves the obstruction without surgery
B. Forceful reduction can push non-viable (dead) bowel back into the abdomen ('reduction en masse'), where it can perforate; later imaging may show free fluid, free gas and an infarcted loop
C. It only risks recurrence of the hernia and has no acute danger
D. It is dangerous solely because it is painful for the patient
Reveal Answer
Answer: B. Forceful reduction can push non-viable (dead) bowel back into the abdomen ('reduction en masse'), where it can perforate; later imaging may show free fluid, free gas and an infarcted loop
Forceful reduction of a strangulated hernia can return ischaemic or dead bowel into the peritoneal cavity ('reduction en masse'), where the loss of the external sign delays diagnosis until the loop perforates and causes peritonitis; subsequent imaging may then show free intraperitoneal gas, free fluid and a non-enhancing infarcted loop. The danger is therefore not merely pain or recurrence but concealed bowel infarction and perforation. Strangulated hernias are operated, not forcibly reduced.
CLINICAL PEARL
Pearl 1 — Strangulation is a clinical diagnosis: A tense, tender, irreducible hernia with obstruction goes to theatre after resuscitation. Do not let a confirmatory scan delay the operation in an obvious case — ischaemic bowel does not wait for a CT slot.
Pearl 2 — Absent enhancement = dead bowel: On contrast CT, the single most important sign is whether the bowel wall enhances. A loop that does NOT take up contrast is ischaemic; a loop that does is viable. Build every interpretation around this one observation.
Pearl 3 — Respect the femoral hernia: Femoral hernias (below and lateral to the pubic tubercle, commoner in older women) are small, easily missed and disproportionately likely to strangulate. Have a low threshold to image and to operate.
Pearl 4 — Never force-reduce a strangulated hernia: 'Reduction en masse' returns dead bowel to the abdomen and converts a visible emergency into a hidden perforation. If reduction is ever attempted, it is gentle and only in carefully selected non-strangulated cases.
Self-Assessment — Strangulated Hernia Imaging Decisions
Work through these scenarios as the surgical doctor on call, integrating the imaging findings into a management plan before reading the discussion.
Scenario A: A 66-year-old man has a tense, tender, irreducible right inguinal hernia, vomiting, distension and absolute constipation for 10 hours, with a heart rate of 110 and a low-grade fever. The intern asks whether to book a CT to confirm strangulation before calling theatre. What is your answer?
Discussion: No CT first. The clinical picture — irreducible, tender hernia with obstruction and early systemic signs — is a clinically strangulated hernia, which is an operative emergency. The correct action is to resuscitate (intravenous fluids, electrolyte correction), pass a nasogastric tube, give antibiotics and analgesia, and take the patient to theatre. Imaging here only delays the operation; the diagnosis is already made at the bedside.
Scenario B: A 58-year-old obese woman has central abdominal pain, vomiting and distension, but no obvious external hernia is palpable through her abdominal wall. Plain X-ray shows dilated small-bowel loops. What imaging do you choose and what specifically are you looking for?
Discussion: This is exactly the situation where imaging earns its place. Obtain a contrast-enhanced CT abdomen and pelvis to find the cause and level of the small-bowel obstruction. Look specifically for a clinically occult hernia (obturator or internal hernia), a closed-loop configuration, and — critically — bowel-wall enhancement to judge viability. If a non-enhancing closed loop with free fluid is found, integrate this as ischaemia and arrange emergency surgery; if the trapped loop enhances, viability is preserved but operative relief of the obstruction is still needed.
Scenario C: A CT done for an irreducible umbilical hernia shows a trapped small-bowel loop that enhances normally, mild bowel-wall thickening, but no free fluid, no closed loop, and no pneumatosis. The patient is uncomfortable but stable. How do you interpret and integrate these findings?
Discussion: Normal enhancement with preserved wall and no ischaemic features indicates an incarcerated but viable hernia rather than strangulation. The bowel is trapped but alive. Integrate this as: the patient still needs surgical management to relieve the irreducible obstruction and repair the defect, but the trapped loop is likely to be reducible and preserved at operation rather than resected, and the situation is urgent but not the same minute-by-minute emergency as a non-enhancing infarcted loop. Continued monitoring for any change toward ischaemic features is essential while surgery is organised.