Page 17 of 26
PA31.{5,7} | Diabetes Mellitus & Pancreatic Cancer — SDL Guide (Part 3)
Chronic Complications — Pathological Basis of Microangiopathy
The chronic complications of diabetes arise from the damaging effects of prolonged hyperglycaemia on blood vessels and nerves. Microangiopathy — disease of small vessels (capillaries and arterioles) — is the unifying pathological mechanism for nephropathy, retinopathy, and neuropathy.
Biochemical mechanisms of hyperglycaemia-induced vascular damage (the four classical pathways):
- Non-enzymatic glycation (NEG): Glucose reacts with proteins (collagen, fibronectin, IgG) → advanced glycation end-products (AGEs) → crosslinking of structural proteins → thickened, rigid basement membranes; also activate monocytes/macrophages to release TNF-α and IL-1
- Polyol pathway (aldose reductase): Excess intracellular glucose → reduced by aldose reductase to sorbitol (accumulates in cells — osmotic damage) → then oxidised to fructose; NADPH is consumed → reduced glutathione → increased oxidative stress; particularly damaging in lens (cataracts), Schwann cells (neuropathy), pericytes of retinal vessels
- Protein kinase C (PKC) activation: Excess diacylglycerol (DAG) from hyperglycaemia → PKC-β activation → increased VEGF (retinal neovascularisation), TGF-β (basement membrane thickening), and ET-1 (vasoconstriction)
- Hexosamine pathway: Excess fructose-6-phosphate diverted → O-GlcNAc modification of proteins → altered gene expression → PAI-1↑, TGF-α↑
Morphological hallmark — basement membrane thickening:
- All small vessels in diabetes show diffuse thickening of the capillary basement membrane, detectable ultrastructurally
- Paradoxically, despite structural thickening, the membrane is more permeable than normal (to albumin and large molecules)
- The mechanism is AGE-mediated crosslinking + type IV collagen overproduction by endothelial cells
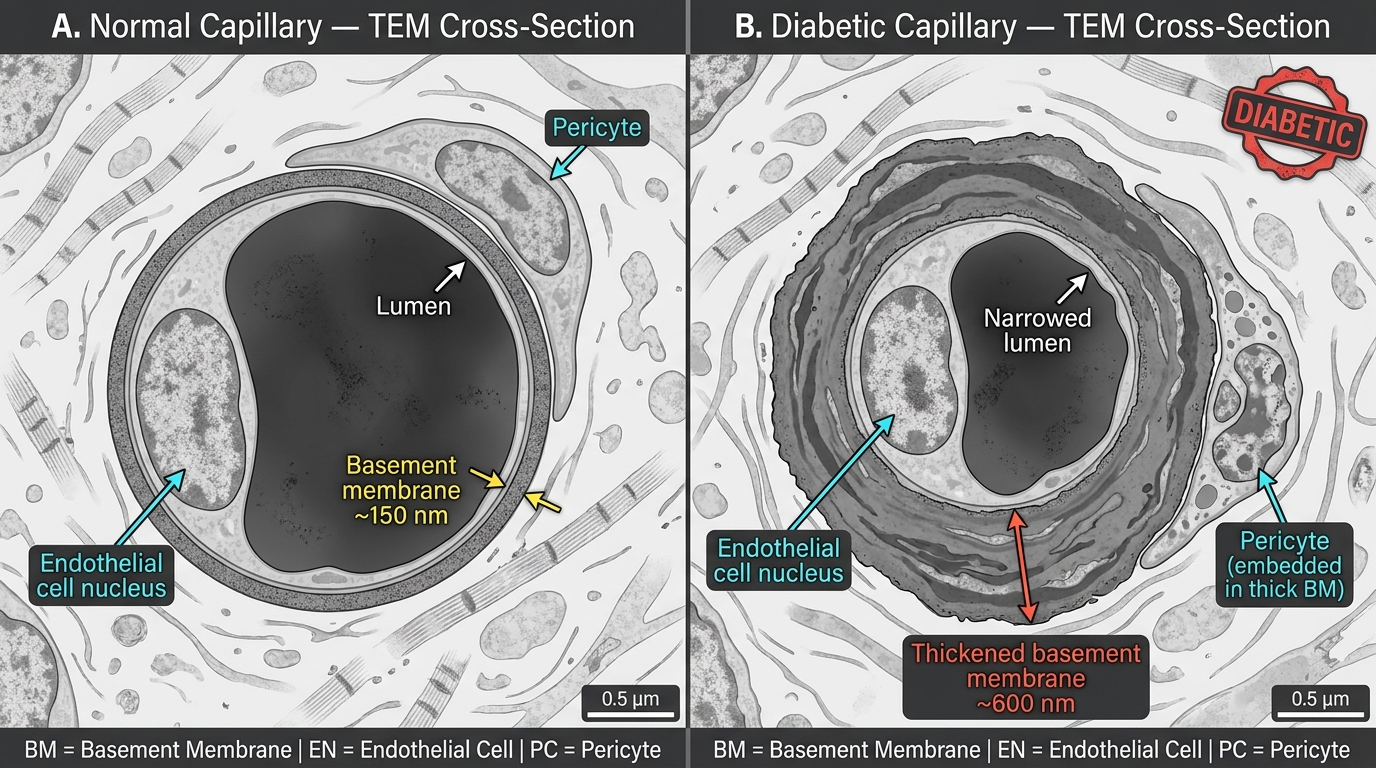
TEM Comparison: Normal vs. Diabetic Capillary Basement Membrane Thickening
Diabetic Nephropathy — Kimmelstiel-Wilson Lesion
Diabetic nephropathy (diabetic glomerulosclerosis) is the leading cause of end-stage renal disease (ESRD) in India and globally. It develops in approximately 30–40% of T1DM and 25% of T2DM patients.
Natural history:
1. Glomerular hyperfiltration (GFR elevated) — early; due to haemodynamic changes; no symptoms
2. Microalbuminuria (30–300 mg/day, detected by urinary ACR) — first clinical sign; marks glomerular injury
3. Macroalbuminuria / overt proteinuria (>300 mg/day) → nephrotic range proteinuria → GFR begins to fall
4. Declining GFR → chronic kidney disease → ESRD over 10–20 years from onset
Gross morphology: Kidneys initially enlarged (glomerular hypertrophy), later shrunken and scarred in ESRD
Microscopic morphology — the diagnostic hallmarks:
- Diffuse glomerulosclerosis — increase in mesangial matrix and basement membrane thickening throughout all glomeruli; most common change; not specific to DM
- Nodular glomerulosclerosis (Kimmelstiel-Wilson lesion) — the pathognomonic lesion:
- Kimmelstiel-Wilson (KW) nodules: rounded, laminated, PAS-positive mesangial deposits at the periphery of the glomerulus
- Composed of acellular matrix material (glycoprotein)
- Located at the periphery of lobules, not centrally (unlike amyloid)
- Capillary loops are displaced peripherally around the nodule
- Often seen alongside microaneurysms of the glomerular capillary loops
- Afferent and efferent arteriolar hyalinosis — thickening of arteriolar walls with PAS-positive hyaline deposits; efferent arteriolar hyalinosis is virtually pathognomonic of DM (other causes of hyalinosis affect only afferent)
- Capsular drop and fibrin cap — exudative lesions: accumulation of plasma proteins between parietal epithelium and Bowman's capsule (capsular drop) or filling a capillary loop (fibrin cap)
- Tubular changes: Glycogen vacuoles in proximal tubular epithelium (Armanni-Ebstein lesion) in severe uncontrolled DM
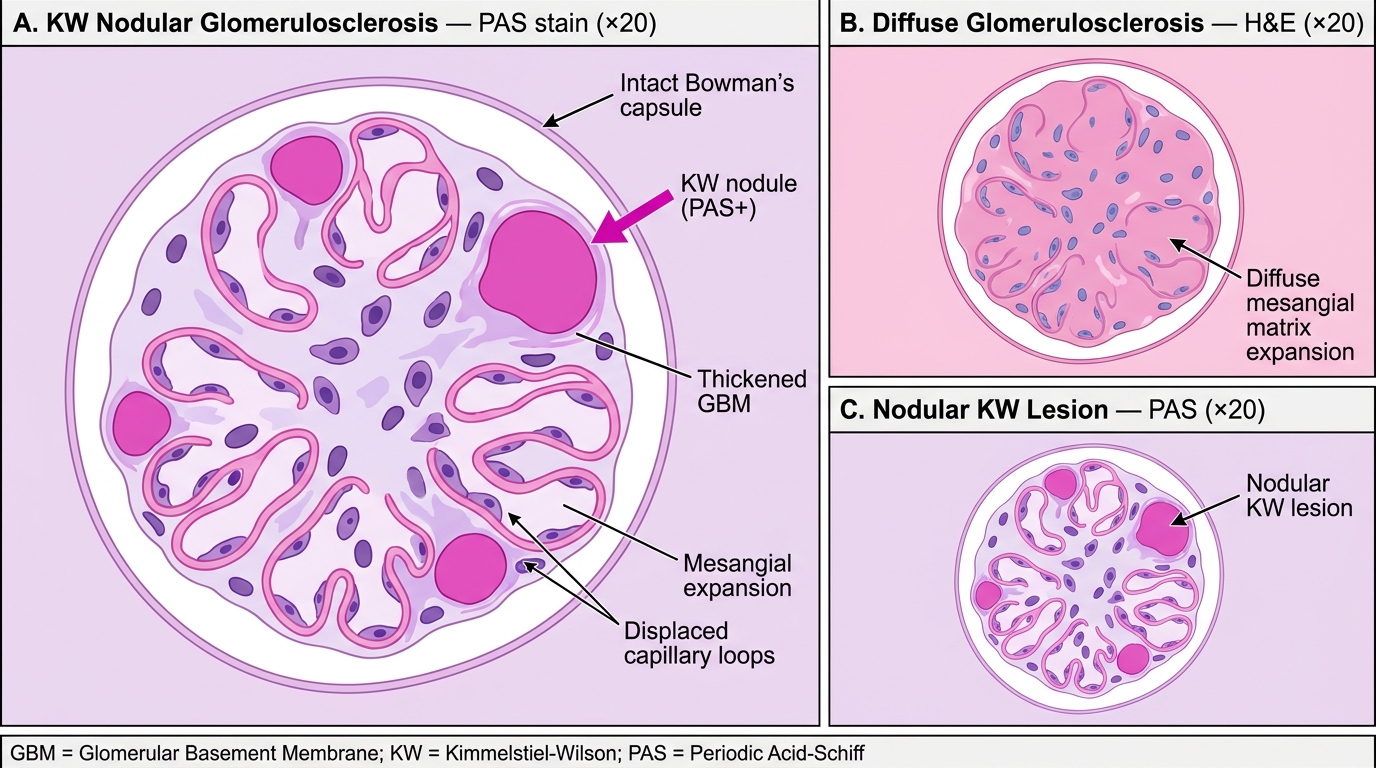
Kimmelstiel-Wilson Nodular Glomerulosclerosis — PAS vs H&E Histology
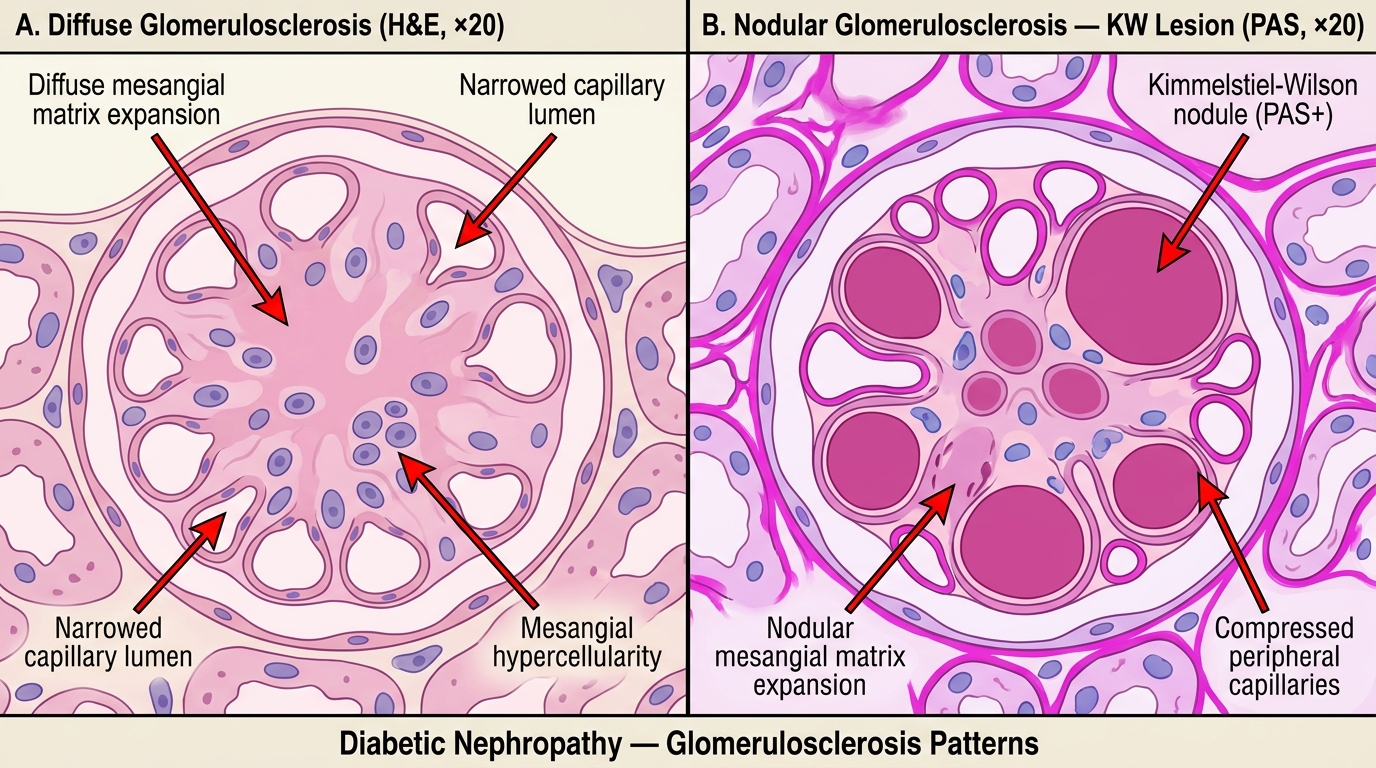
Diabetic Glomerulosclerosis: Diffuse vs Nodular (KW) Patterns
Diabetic Retinopathy, Neuropathy, and Macrovascular Disease
Diabetic retinopathy — the leading cause of blindness in working-age adults in India:
Non-proliferative (background) retinopathy:
- Retinal capillary basement membrane thickening → pericyte loss → capillary microaneurysms (first visible lesion on fundoscopy)
- Dot and blot haemorrhages (dot = microaneurysm rupture, blot = intraretinal haemorrhage)
- Hard exudates — lipid deposits from leaking vessels (cream-white deposits with sharp borders)
- Cotton-wool spots — microinfarcts of the nerve fibre layer (soft exudates, fluffy borders)
- Macular oedema — increased vascular permeability → fluid accumulation in the macula → visual impairment
Proliferative retinopathy:
- Retinal ischaemia → VEGF release → neovascularisation (new vessels grow on retinal surface / optic disc — fragile, bleed easily)
- Vitreous haemorrhage → sudden blindness
- Tractional retinal detachment → permanent visual loss
Diabetic neuropathy — the most common complication (~50% of patients at 25 years of DM):
- Mechanism: polyol pathway (sorbitol in Schwann cells) + microangiopathy of vasa nervorum (endoneurial capillaries) → segmental demyelination + axonal loss
- Most common pattern: distal symmetrical sensorimotor polyneuropathy ("glove and stocking" distribution) — affects small fibres first (pain, temperature) then large fibres (vibration, proprioception)
- Autonomic neuropathy: gastroparesis, postural hypotension, neurogenic bladder, erectile dysfunction, silent MI (painless because cardiac autonomic neuropathy masks chest pain)
Macrovascular disease — accelerated atherosclerosis:
- DM is a major independent risk factor for coronary artery disease (CAD), peripheral arterial disease (PAD), and stroke
- Mechanism: endothelial dysfunction (↓NO, ↑ET-1), dyslipidaemia (↑TG, ↑LDL, ↓HDL), prothrombotic state (↑PAI-1, ↑platelet aggregation), hypertension (common co-morbidity)
- Atherosclerosis in DM: more diffuse, more distal (involves tibial and popliteal arteries in PAD), more aggressive
Diabetic foot — a convergence of neuropathy, ischaemia, and infection:
- Neuropathy → loss of protective pain sensation → unnoticed trauma → ulceration
- Ischaemia (PAD) → impaired wound healing
- Hyperglycaemia → impaired neutrophil function → infection → polymicrobial (including anaerobes) → osteomyelitis → amputation
- Charcot arthropathy: neuropathic joint destruction, typically midfoot, with bony fragmentation and collapse
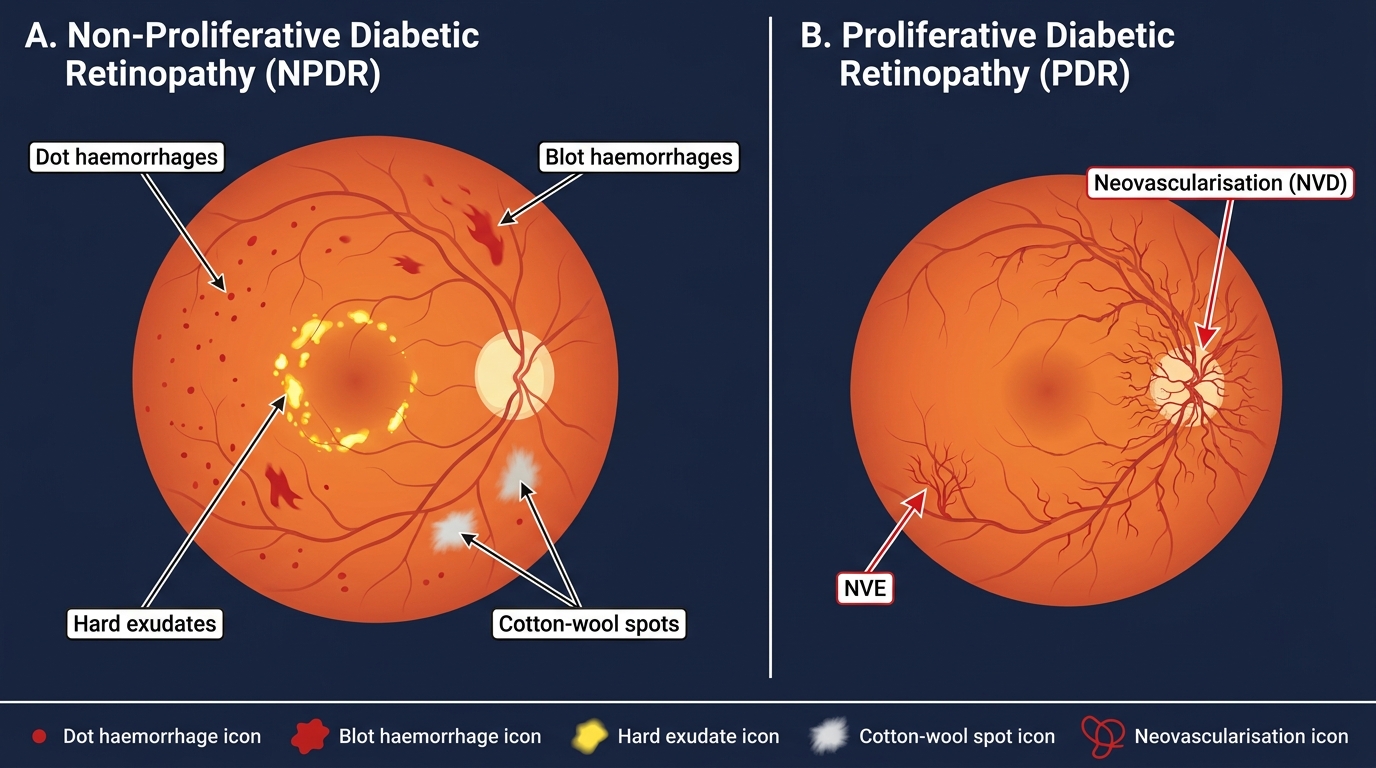
Diabetic Retinopathy — NPDR vs PDR Fundus Comparison
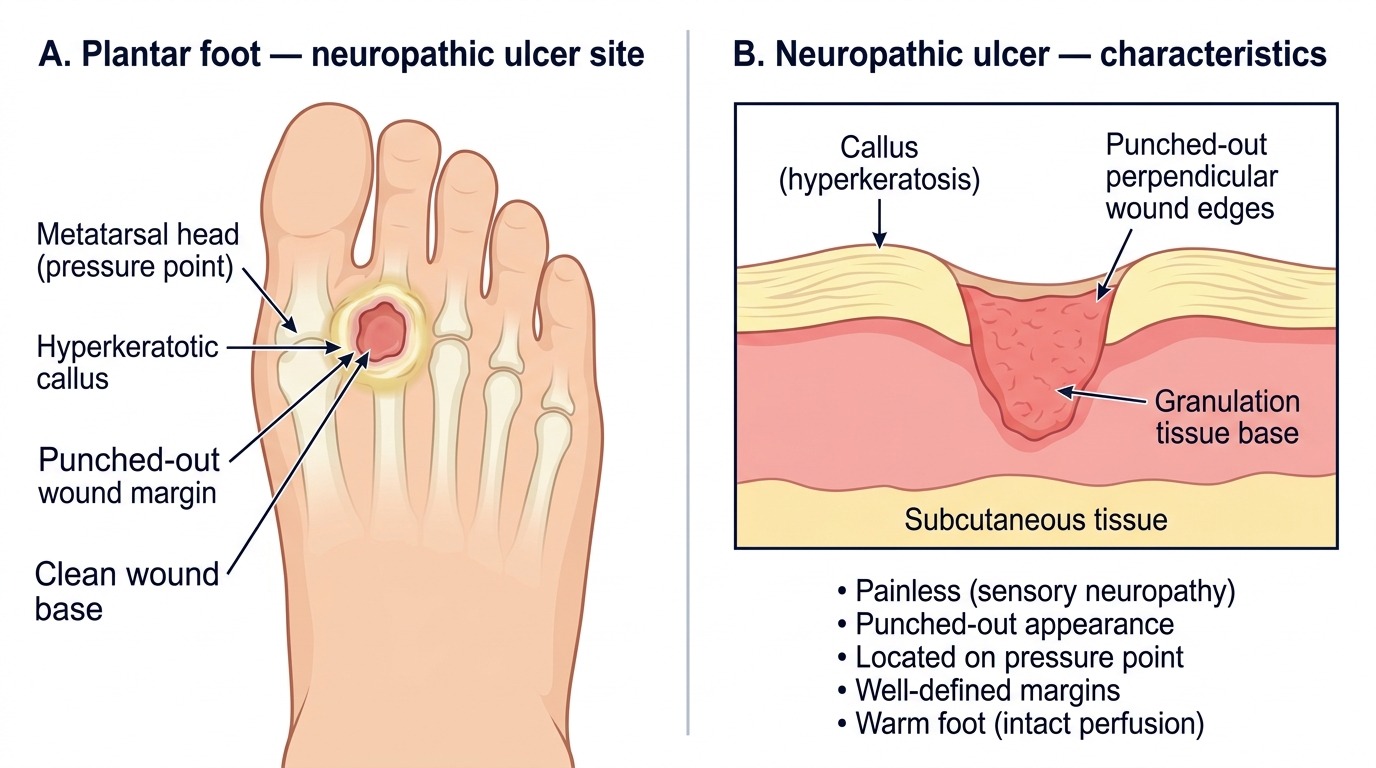
Diabetic Neuropathic Foot Ulcer — Site and Characteristics
SELF-CHECK
A 58-year-old man with 22-year history of T2DM undergoes renal biopsy for nephrotic-range proteinuria. Histology shows rounded, PAS-positive acellular deposits at the periphery of glomerular lobules, with displaced capillary loops. Efferent arteriolar hyalinosis is also noted. What is the most likely diagnosis?
A. Amyloid nephropathy
B. Focal segmental glomerulosclerosis
C. Nodular diabetic glomerulosclerosis (Kimmelstiel-Wilson lesion)
D. Membranoproliferative glomerulonephritis
Reveal Answer
Answer: C. Nodular diabetic glomerulosclerosis (Kimmelstiel-Wilson lesion)
The combination of rounded PAS-positive mesangial nodules at the periphery of lobules with efferent arteriolar hyalinosis is pathognomonic of diabetic nodular glomerulosclerosis (Kimmelstiel-Wilson lesion). Amyloid deposits are also acellular and PAS-positive but are Congo-red positive with apple-green birefringence and typically involve the mesangium centrally and also vessels. FSGS shows focal segmental sclerosis (not nodular). MPGN shows mesangial hypercellularity, double contours, and tram-tracking — not discrete nodules. Efferent arteriolar hyalinosis is virtually pathognomonic of diabetes (other diseases only affect the afferent arteriole).