Page 10 of 24
PA2.{3,6-7} | Cellular Adaptations, Accumulations & Aging — SDL Guide (Part 2)
Hyperplasia
Hyperplasia: Mechanism, Types, and Distinction from Neoplasia
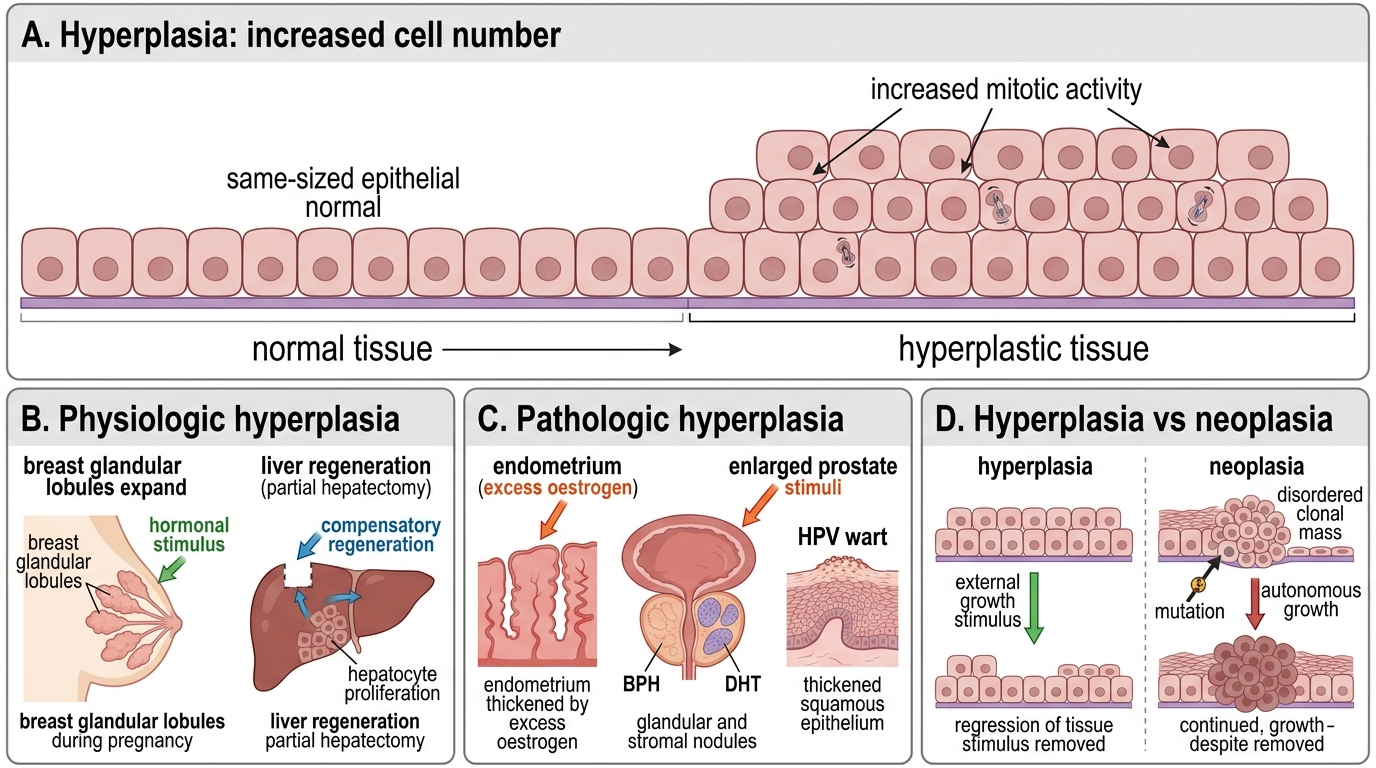
Hyperplasia is an increase in cell number in a tissue or organ, driven by increased mitotic activity in cells capable of division. It often accompanies hypertrophy.
Physiologic hyperplasia:
• Hormonal — endometrial hyperplasia at puberty/pregnancy; breast glandular hyperplasia in pregnancy
• Compensatory — liver regeneration after partial hepatectomy (up to 70% resection)
Pathologic hyperplasia:
• Endometrial hyperplasia from excess oestrogen (post-menopausal oestrogenic stimulation → risk of endometrial carcinoma)
• Benign prostatic hyperplasia (BPH) — glandular and stromal hyperplasia from dihydrotestosterone excess
• Skin warts — HPV-driven epithelial hyperplasia
Hyperplasia vs Neoplasia:
| Feature | Hyperplasia | Neoplasia |
|---|---|---|
| Growth stimulus | External (hormones, GFs) | Autonomous (mutation) |
| Growth control | Halts when stimulus removed | Continues without stimulus |
| Architecture | Preserved | Disrupted |
| Reversibility | Yes | No |
Pathologic hyperplasia, while controlled, provides fertile ground for neoplasia: if a proliferating cell acquires a mutation, that cell may escape normal growth control.
Metaplasia
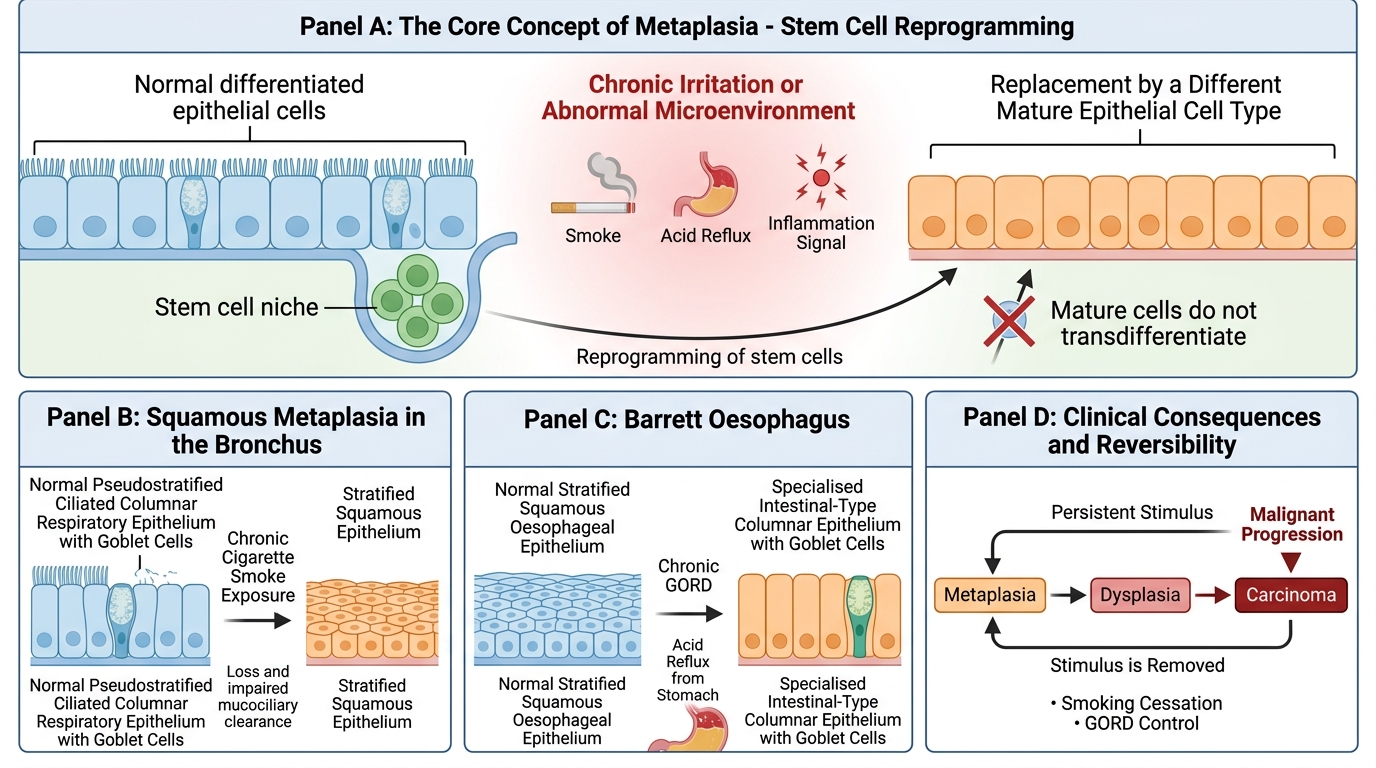
Metaplasia is a reversible change in which one differentiated cell type is replaced by another, usually in response to chronic irritation or abnormal microenvironment.
Squamous metaplasia (most common):
• Respiratory tract: bronchial pseudostratified columnar epithelium → squamous epithelium in chronic smokers
• Cervix: endocervical columnar → squamous at transformation zone (normal physiologic variant → pathologic with HPV)
• Urinary bladder, gallbladder with chronic inflammation
Columnar (glandular) metaplasia:
• Barrett oesophagus: normal stratified squamous oesophageal epithelium → specialised intestinal-type columnar epithelium, driven by chronic GORD. Clinically significant because it is a pre-neoplastic lesion (risk of oesophageal adenocarcinoma ×30–40).
Mechanism: Reprogramming of stem cells — the resident (or migrating) stem cells differentiate down a different pathway in response to altered signals (retinoic acid, BMP). The mature cells themselves do not transdifferentiate; new cells emerge with a different phenotype.
Reversibility and risk: Metaplasia is reversible if the stimulus is removed (e.g., bronchial metaplasia partially regresses on smoking cessation). However, the new epithelium may be less functional (loss of cilia → impaired mucociliary clearance) and carries a risk of malignant transformation if the stimulus persists — particularly if squamous metaplasia passes through a dysplastic phase.
Metaplasia: Stem Cell Reprogramming and Clinical Risk
CLINICAL PEARL
Barrett's oesophagus is detected on endoscopy as 'salmon-pink' tongues of mucosa extending up from the gastro-oesophageal junction. Histological confirmation requires goblet cells (alcian blue positive). Surveillance biopsies every 3–5 years look for progression to dysplasia. Low-grade dysplasia → high-grade → adenocarcinoma is the classic sequence. Never call Barrett's 'just metaplasia' in a clinical setting — it demands active surveillance.
Dysplasia — Disordered Growth and Pre-neoplastic Risk
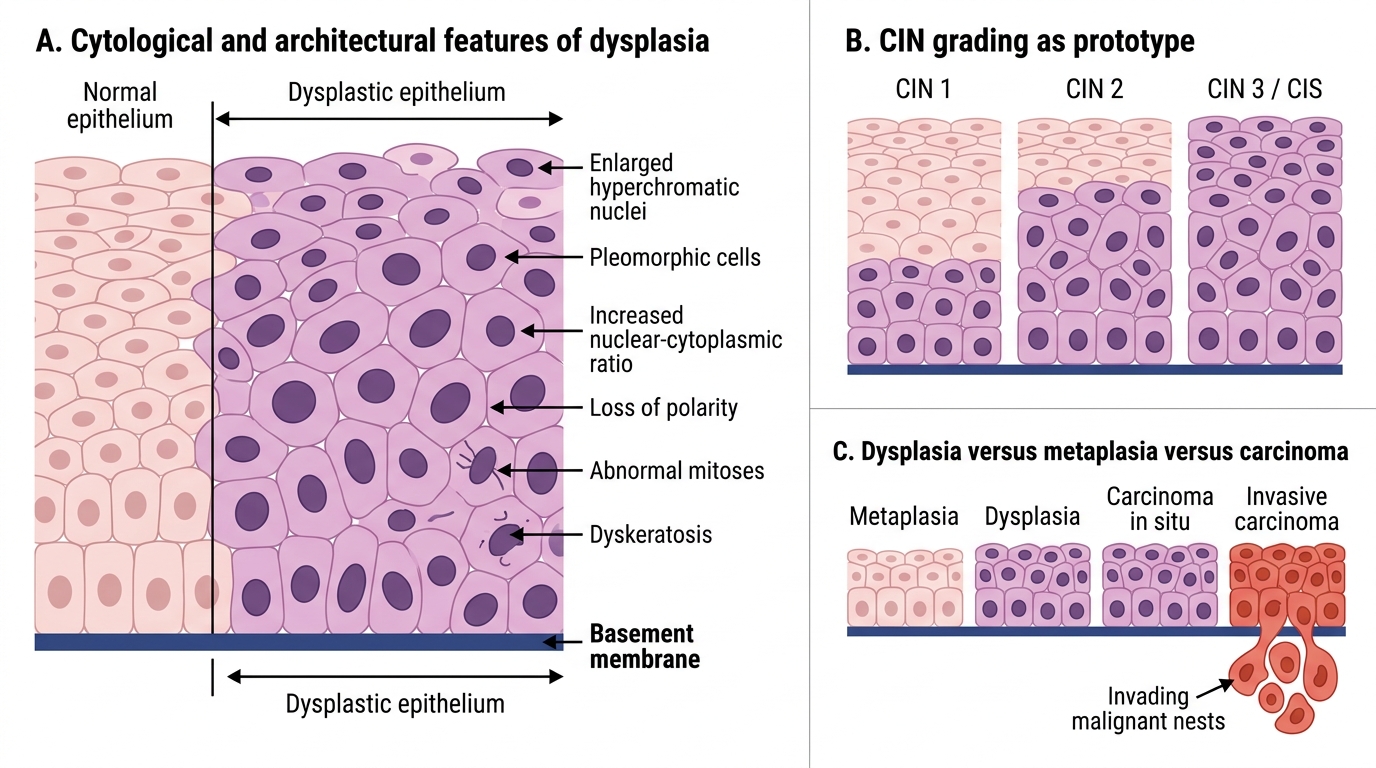
Dysplasia (literally 'disordered growth') refers to a spectrum of architectural and cytological abnormalities in a tissue, intermediate between normal and carcinoma in situ. It is not synonymous with metaplasia, nor with cancer.
Cytological features of dysplasia:
• Pleomorphism — variation in cell size and shape
• ↑ Nuclear-cytoplasmic ratio
• Nuclear hyperchromatism
• Loss of polarity — cells no longer arranged perpendicular to basement membrane
• Abnormal mitotic figures
• Premature keratinisation (dyskeratosis)
Grading — cervical intraepithelial neoplasia (CIN) as prototype:
• CIN 1 (mild dysplasia): changes confined to lower ⅓ of epithelium
• CIN 2 (moderate): lower and middle ⅓
• CIN 3 / CIS (severe/carcinoma in situ): full thickness, basement membrane intact
Dysplasia vs Metaplasia vs Cancer:
| Metaplasia | Dysplasia | Carcinoma in situ | Invasive carcinoma | |
|---|---|---|---|---|
| BM intact | Yes | Yes | Yes | No |
| Architecture | Preserved | Partially disrupted | Fully disrupted | Invasive |
| Reversibility | Yes | Partially | No | No |
| Cytological atypia | Absent | Present | Marked | Marked |
Dysplasia is pre-neoplastic, not malignant. Low-grade dysplasia may regress; high-grade dysplasia (CIN 3) has significant risk of progression and is treated.
Dysplasia: Disordered Growth and Pre-neoplastic Risk
SELF-CHECK
A 28-year-old woman's Pap smear shows cells with a high nuclear-cytoplasmic ratio, nuclear hyperchromatism, and loss of polarity. Colposcopic biopsy confirms changes confined to the lower two-thirds of the cervical epithelium with an intact basement membrane. What is the correct diagnosis?
A. Squamous metaplasia of the cervix
B. CIN 1 (mild dysplasia)
C. CIN 2 (moderate dysplasia)
D. Invasive squamous cell carcinoma
Reveal Answer
Answer: C. CIN 2 (moderate dysplasia)
Changes extending through the lower two-thirds of the epithelium with cytological atypia (↑ N:C ratio, hyperchromatism, loss of polarity) and an intact basement membrane define CIN 2. CIN 1 involves only the lower third; CIN 3/CIS involves full thickness. Invasion requires basement membrane breach. Metaplasia lacks cytological atypia.