Page 14 of 22
PA9.1-2 | Amyloidosis — SDL Guide (Part 2)
Organ Involvement and Clinical Consequences
Amyloid deposits between and around cells, causing progressive pressure atrophy and vascular compromise. The organs most affected and the consequences vary by amyloid type.
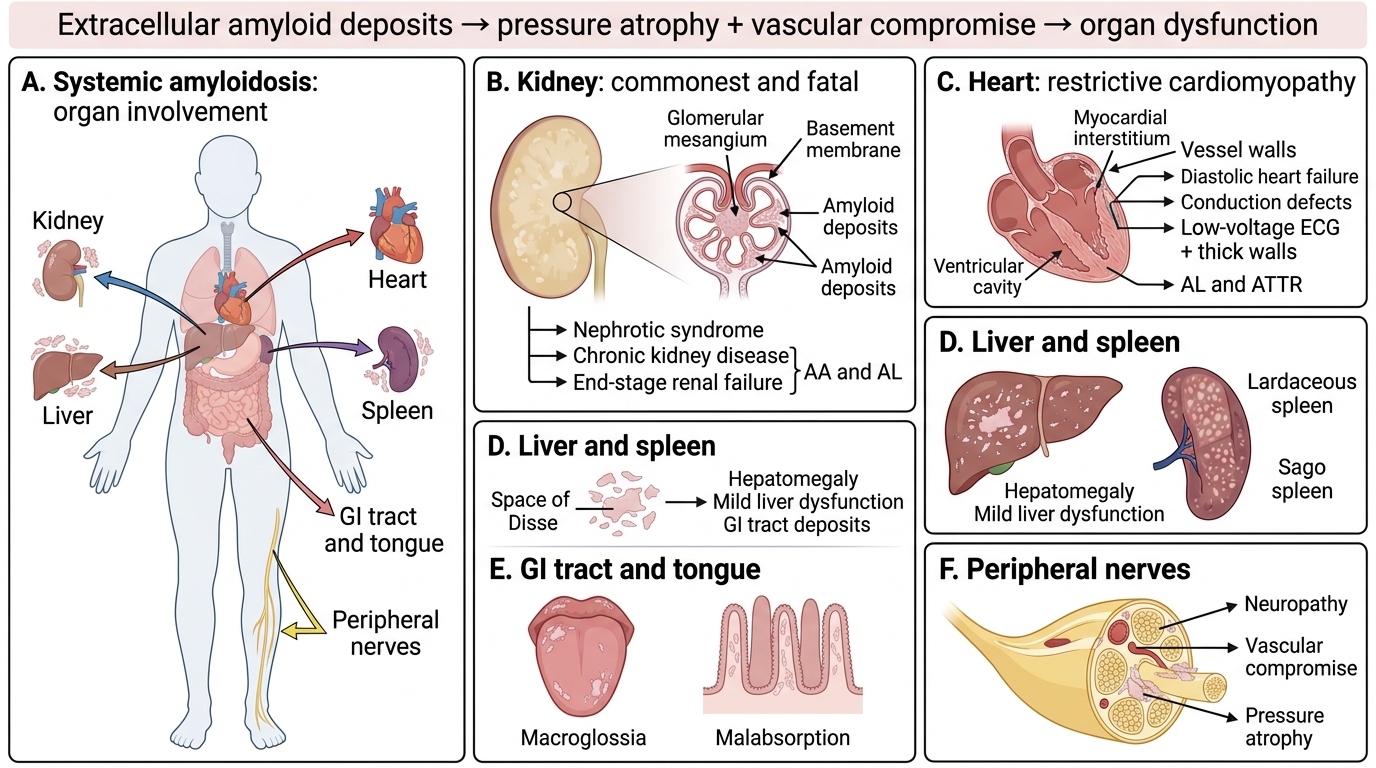
Systemic Amyloidosis: Organ Involvement and Clinical Consequences
Kidney — the most commonly affected and the leading cause of death in systemic amyloidosis
- Deposits in glomerular mesangium and basement membrane → obliterates filtration surface
- Clinically: nephrotic syndrome (massive proteinuria, hypoalbuminaemia, oedema) → progressive chronic kidney disease → end-stage renal failure
- Gross: enlarged, pale, firm, waxy-cut-surface kidneys
- AA and AL types both devastate the kidney
Heart
- Deposits in myocardial interstitium and vessel walls → restrictive cardiomyopathy
- Clinically: diastolic heart failure, conduction defects (heart block), low-voltage ECG pattern despite echocardiographic hypertrophy — a classic ECG-echo mismatch
- Echocardiography: granular sparkling pattern, thickened walls, small ventricular cavity
- AL and senile ATTR primarily
Liver and Spleen
- Liver: deposits in space of Disse → hepatomegaly, mild liver dysfunction (jaundice rare)
- Spleen: two patterns:
- Sago spleen — deposits in follicles → tapioca-grain appearance
- Lardaceous spleen — diffuse deposits in red pulp → homogeneous, lard-like cut surface
- Clinically: splenomegaly, hyposplenism (functional asplenia risk)
Gastrointestinal Tract
- Tongue: macroglossia — hallmark of AL; firm, rubbery enlargement
- Wall deposits → dysmotility, malabsorption, protein-losing enteropathy
- Submucosal deposits → "accordion" mucosal folds on endoscopy
Peripheral and Autonomic Nerves
- Deposits compress nerve fibres → sensorimotor peripheral neuropathy (painful, length-dependent)
- Autonomic neuropathy: postural hypotension, impotence, bladder dysfunction
- Prominent in familial ATTR and AL
Other sites: adrenal (adrenal insufficiency), skin (waxy papules in AL), joints (amyloid arthropathy)
CLINICAL PEARL
The ECG-echo mismatch in cardiac amyloid: In most causes of left ventricular hypertrophy (hypertension, aortic stenosis), ECG shows high-voltage QRS complexes. In amyloid cardiomyopathy, the thickened walls on echo are filled with amyloid (electrically inert), so the ECG shows low voltage or a pseudo-infarct pattern. This dissociation between echo wall thickness and ECG voltage is a red-flag sign for cardiac amyloid.
Macroglossia is not caused by muscle hypertrophy — it is amyloid infiltration of the tongue stroma. It is virtually pathognomonic of systemic AL amyloidosis when found in an adult.
Morphology — Gross and Microscopic Features
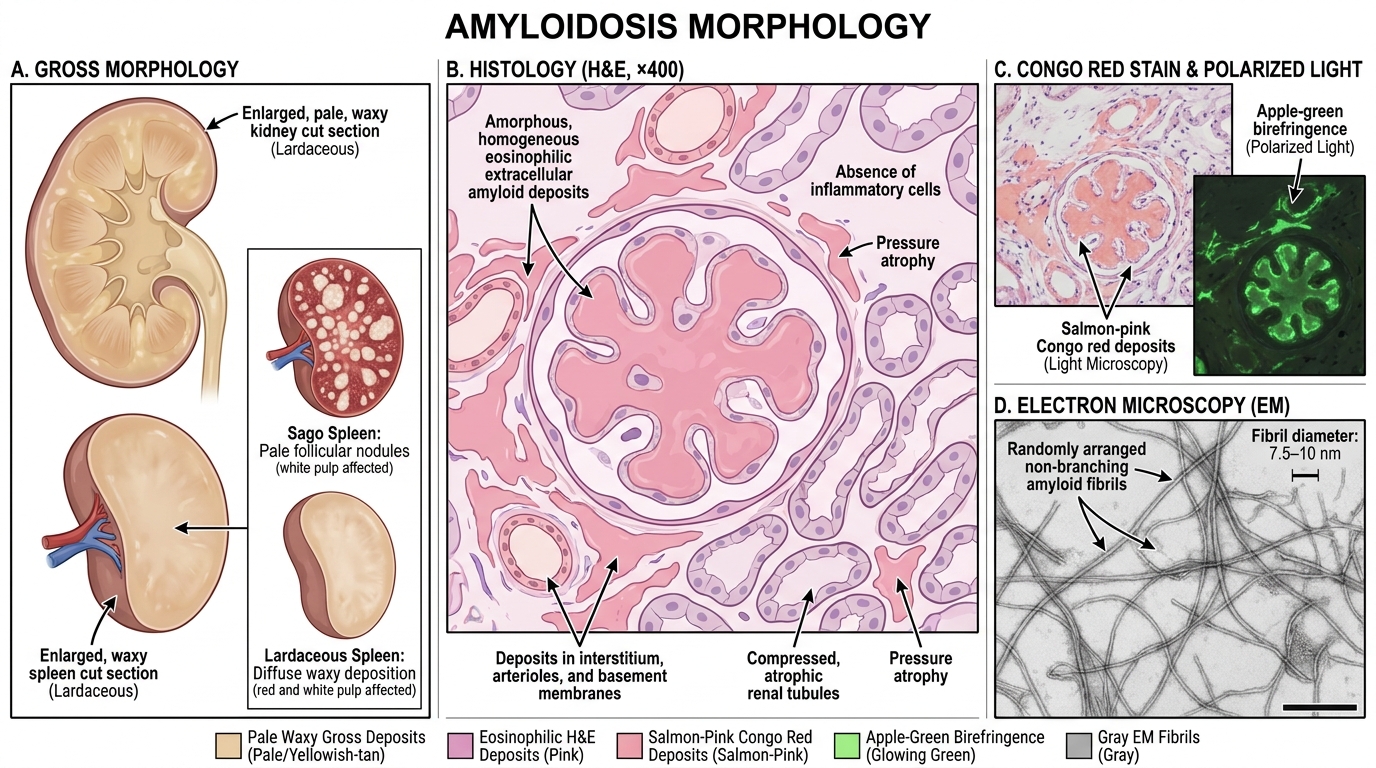
Gross morphology:
Affected organs are typically:
• Enlarged, firm, and pale
• Cut surface has a waxy, translucent appearance — described historically as "lardaceous" (lard-like)
• Iodine reaction: Lugol's iodine stains amyloid brown; dilute H₂SO₄ turns it blue-violet (mahogany colour)
• Spleen shows sago (follicular) or lardaceous (diffuse) patterns as above
Microscopic morphology (H&E):
- Amyloid appears as amorphous, homogeneous, eosinophilic, hyaline extracellular material
- Deposits around small blood vessels, between cells, and in basement membranes
- No cellular inflammatory response in established deposits (unlike acute inflammation)
- Over time, adjacent parenchymal cells undergo pressure atrophy — functional tissue is replaced by inert protein
Special stain — Congo red (the gold standard):
- Congo red on standard light microscopy: salmon-pink staining of deposits
- Congo red under crossed polarised light: apple-green birefringence — pathognomonic
- Sensitivity ~85%, specificity ~97% when birefringence is assessed by an experienced observer
Morphology of Amyloidosis
Electron microscopy (research/reference labs):
• Non-branching fibrils, 7.5–10 nm diameter, randomly arranged
• P component seen as pentagonal structures associated with fibrils
Diagnosis — Biopsy Strategies
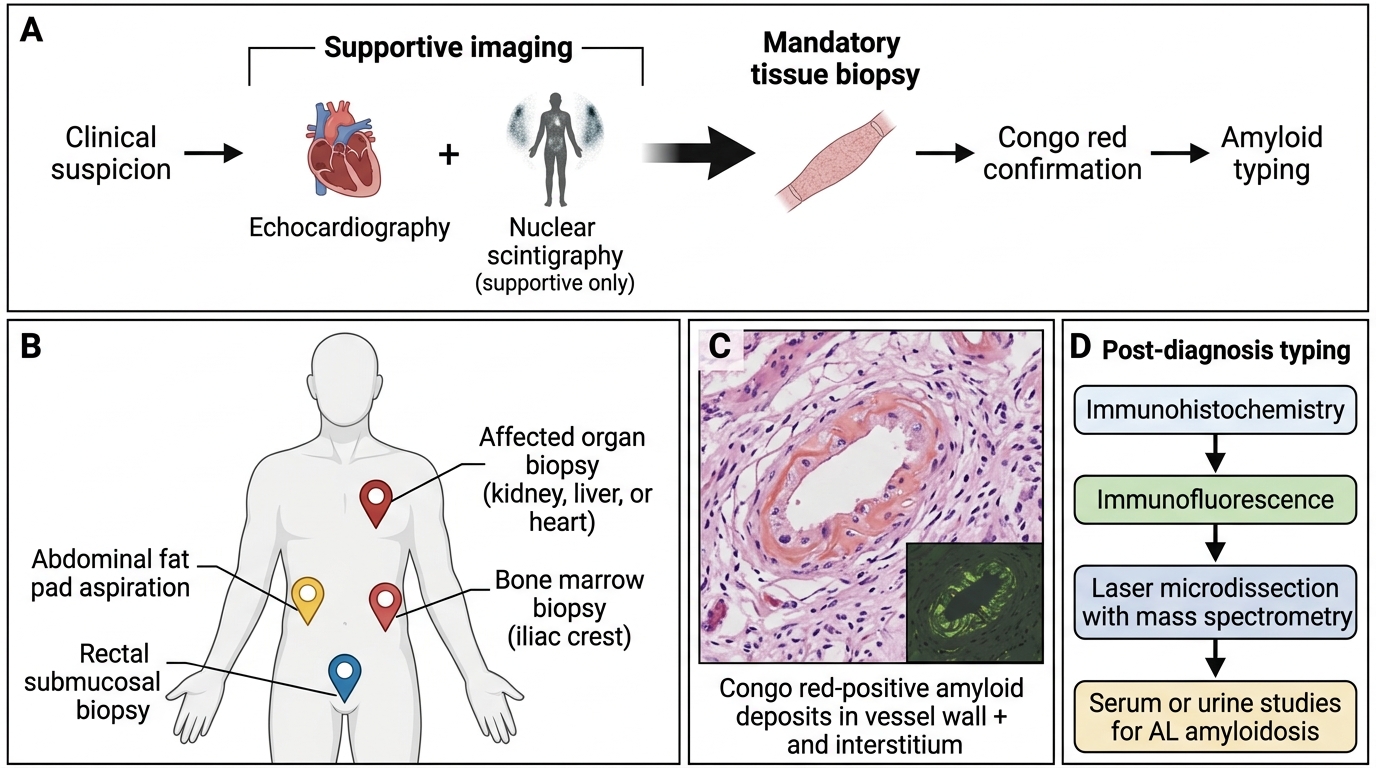
Biopsy Strategy for Diagnosis of Amyloidosis
Tissue biopsy is mandatory for definitive diagnosis. Imaging (echocardiography, nuclear scintigraphy with SAP or DPD) can suggest the diagnosis and help with typing, but histological confirmation with Congo red is required.
Preferred biopsy sites (systemic amyloidosis):
| Site | Yield | Notes |
|---|---|---|
| Abdominal fat pad aspiration | ~80% sensitivity | Least invasive; first choice in suspected systemic disease |
| Rectal biopsy (submucosal) | ~75–80% | Good alternative; submucosal vessels consistently involved |
| Bone marrow biopsy | ~60–70% | Simultaneously assesses plasma cell burden in AL |
| Affected organ (kidney, liver, heart) | >90% | Highest yield but most invasive; used when above are negative |
Typing after diagnosis:
- Immunohistochemistry (anti-κ, anti-λ, anti-SAA, anti-TTR) — widely available; AL can be difficult
- Laser microdissection + mass spectrometry — gold standard for protein typing; resolves difficult cases
- Serum/urine studies: SPEP, UPEP, serum free light chains → plasma cell dyscrasia
- Genetic testing: for ATTR mutations in familial disease
- SAP scintigraphy — whole-body amyloid load and distribution (not available everywhere)
Practical point: Abdominal fat pad + bone marrow together achieve ~90% sensitivity for systemic AL — non-invasively sufficient to start treatment in most patients.
SELF-CHECK
At autopsy, a 70-year-old man's spleen is enlarged and shows scattered, translucent, tapioca-grain–like deposits in the white pulp on cut section. Which pattern of splenic amyloidosis does this describe?
A. Lardaceous spleen — diffuse deposits in the red pulp
B. Sago spleen — deposits confined to the follicles
C. Amyloid angiopathy — deposits in splenic artery walls only
D. Infiltrative pattern — deposits in the capsule and trabeculae
Reveal Answer
Answer: B. Sago spleen — deposits confined to the follicles
Sago spleen is the follicular pattern — amyloid deposits in the white pulp (follicles), producing discrete, translucent grey nodules resembling sago or tapioca pearls. Lardaceous spleen (option A) describes the diffuse red-pulp pattern, which produces a homogeneous, lard-like, grey-white cut surface. Both patterns can coexist in advanced disease.