Page 15 of 22
PA9.1-2 | Amyloidosis — SDL Guide (Part 3)
Systemic vs Localised Amyloidosis — Summary Framework
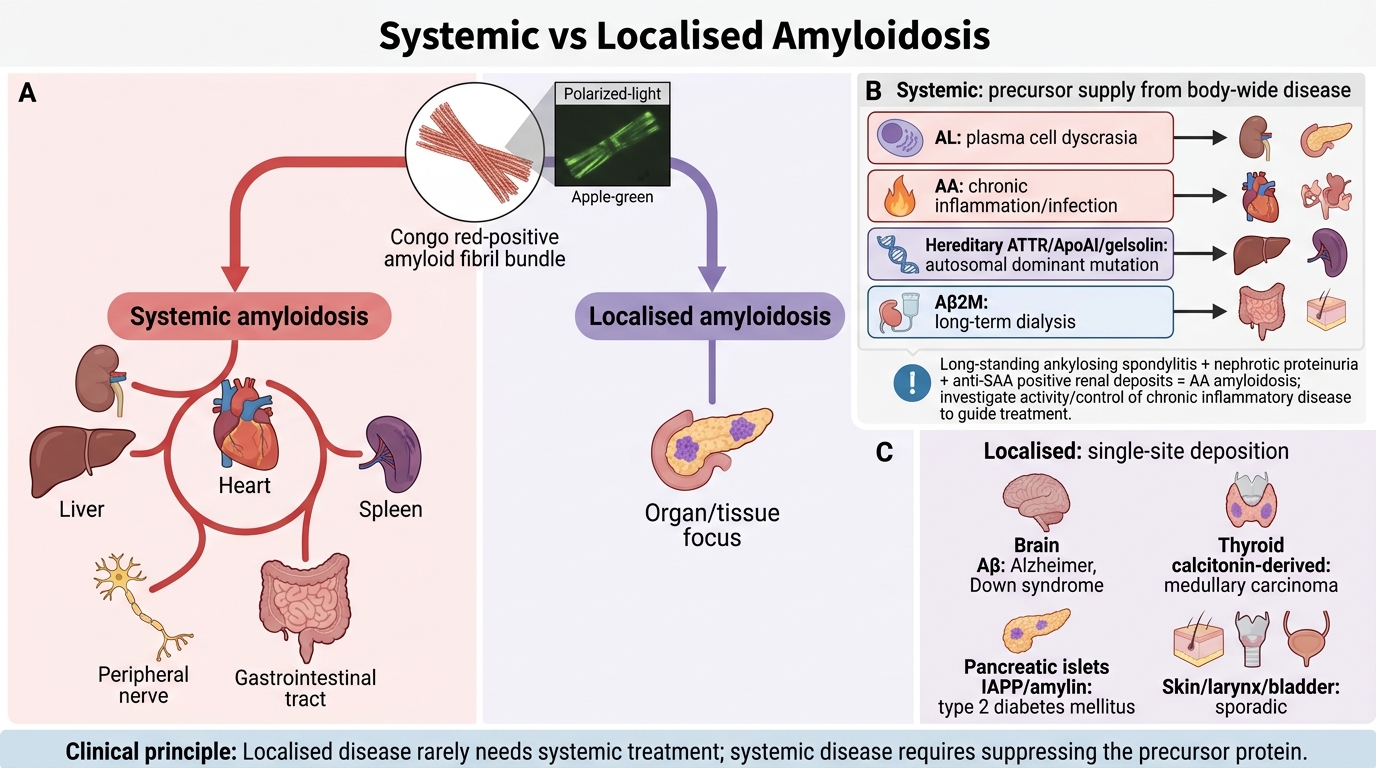
Systemic vs Localised Amyloidosis
Systemic (generalised) amyloidosis: Amyloid deposits in multiple organ systems. May be:
- Primary systemic (AL): associated with plasma cell dyscrasia; no predisposing chronic illness
- Secondary systemic (AA): complicates chronic inflammatory or infectious diseases
- Heredofamilial systemic (ATTR, ApoAI, gelsolin, etc.): autosomal dominant point mutations
- Dialysis-associated (Aβ2M): specific to long-term renal replacement therapy
Localised amyloidosis: Deposits restricted to a single organ or tissue. Usually less clinically severe unless it involves a critical structure.
Examples:
• Brain (Aβ) — Alzheimer, Down syndrome
• Thyroid (calcitonin-derived) — medullary carcinoma
• Pancreatic islets (IAPP/amylin) — type 2 DM
• Skin, larynx, bladder (sporadic)
Key clinical principle: Localised amyloidosis rarely requires systemic treatment. Systemic amyloidosis, by contrast, requires treatment of the underlying cause (suppress the supply of the precursor protein): chemotherapy for AL, anti-inflammatory treatment or disease-modifying therapy for AA, tafamidis or liver transplantation for hereditary ATTR.
SELF-CHECK
A 55-year-old man with long-standing ankylosing spondylitis is found to have nephrotic-range proteinuria. His renal biopsy shows Congo red-positive deposits that stain with anti-SAA antibody on immunohistochemistry. Which of the following additional investigations is MOST appropriate to guide treatment?
A. Bone marrow trephine biopsy to detect plasma cell dyscrasia
B. Serum transthyretin level and TTR gene mutation analysis
C. Assessment of inflammatory disease activity (CRP, ESR) and optimisation of anti-inflammatory therapy
D. Long-term haemodialysis access planning
Reveal Answer
Answer: C. Assessment of inflammatory disease activity (CRP, ESR) and optimisation of anti-inflammatory therapy
This is AA amyloidosis (confirmed by anti-SAA immunohistochemistry) complicating ankylosing spondylitis. The cornerstone of AA management is suppression of the underlying chronic inflammatory disease to reduce SAA production. CRP/ESR reflect disease activity; disease-modifying therapy (NSAIDs, biologics — anti-TNF) can halt and even reverse early AA amyloid deposits. Bone marrow biopsy (A) is appropriate for AL, not AA. TTR analysis (B) is for ATTR. Dialysis (D) is for end-stage kidney disease, not a treatment strategy for the amyloidosis itself.