Page 16 of 25
PA27.3-4 | Acute & Chronic Renal Failure — SDL Guide (Part 2)
Phases of ATN
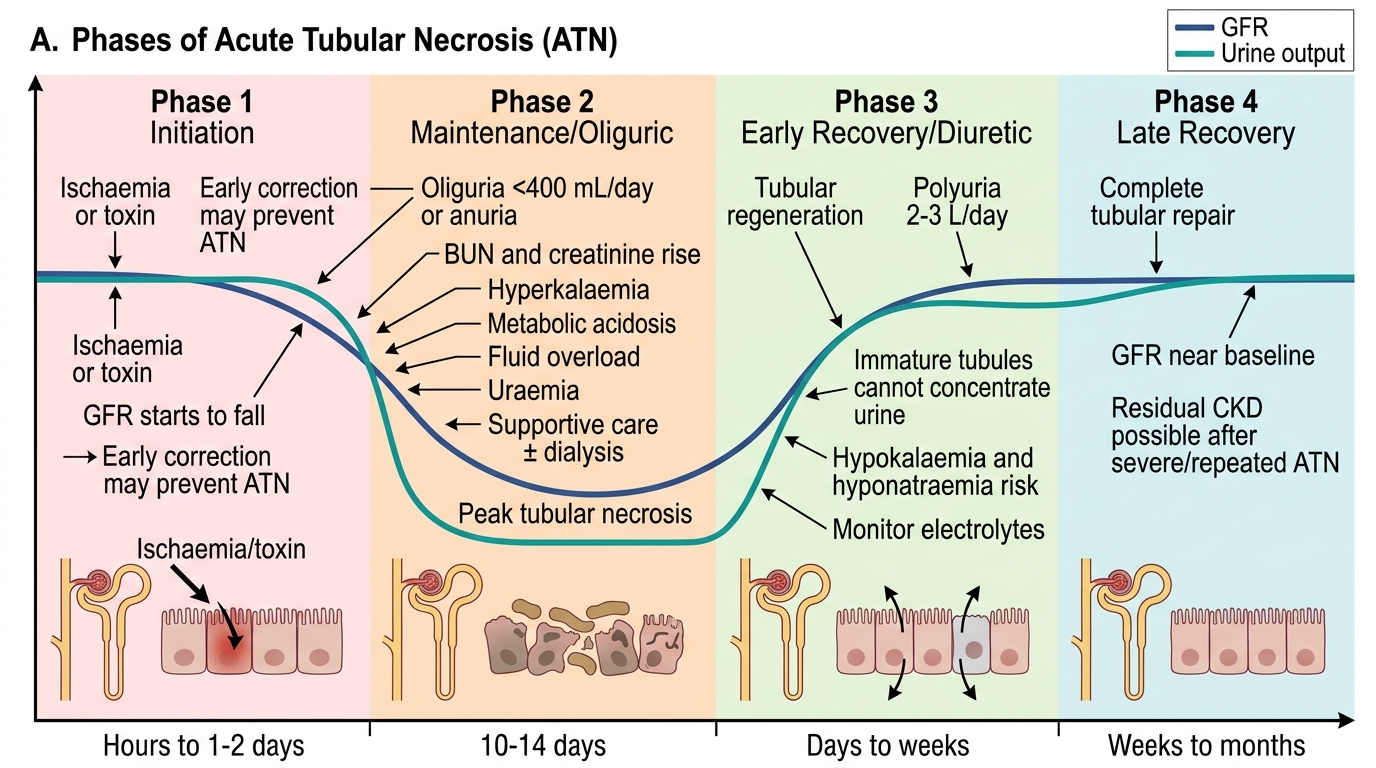
Phases of Acute Tubular Necrosis
ATN progresses through four stereotyped phases. Recognising which phase a patient is in guides clinical management.
Phase 1 — Initiation (hours to 1–2 days): The injurious event (ischaemia or toxin) begins. GFR starts to fall but may not yet be clinically apparent. Prompt correction of ischaemia here can prevent full ATN.
Phase 2 — Maintenance/Oliguric phase (typically 10–14 days): GFR severely reduced. Oliguria (<400 mL/day) or even anuria. BUN and creatinine rise steadily. This is the phase of greatest metabolic derangement: hyperkalaemia, metabolic acidosis, fluid overload, uraemia. Management is supportive ± dialysis. Renal biopsy (if done) shows peak tubular necrosis.
Phase 3 — Early recovery/Diuretic phase: Tubular epithelium regenerates (tubular cells have high regenerative capacity). GFR begins to recover. A polyuric phase may follow — urine output rises steeply (2–3 L/day). The regenerating tubules are functionally immature: cannot yet concentrate urine or reabsorb electrolytes → hypokalaemia and hyponatraemia can occur paradoxically. Monitor electrolytes closely.
Phase 4 — Late recovery: Complete tubular repair. GFR returns to near-baseline over weeks to months. Some patients with severe or repeated ATN develop residual CKD.
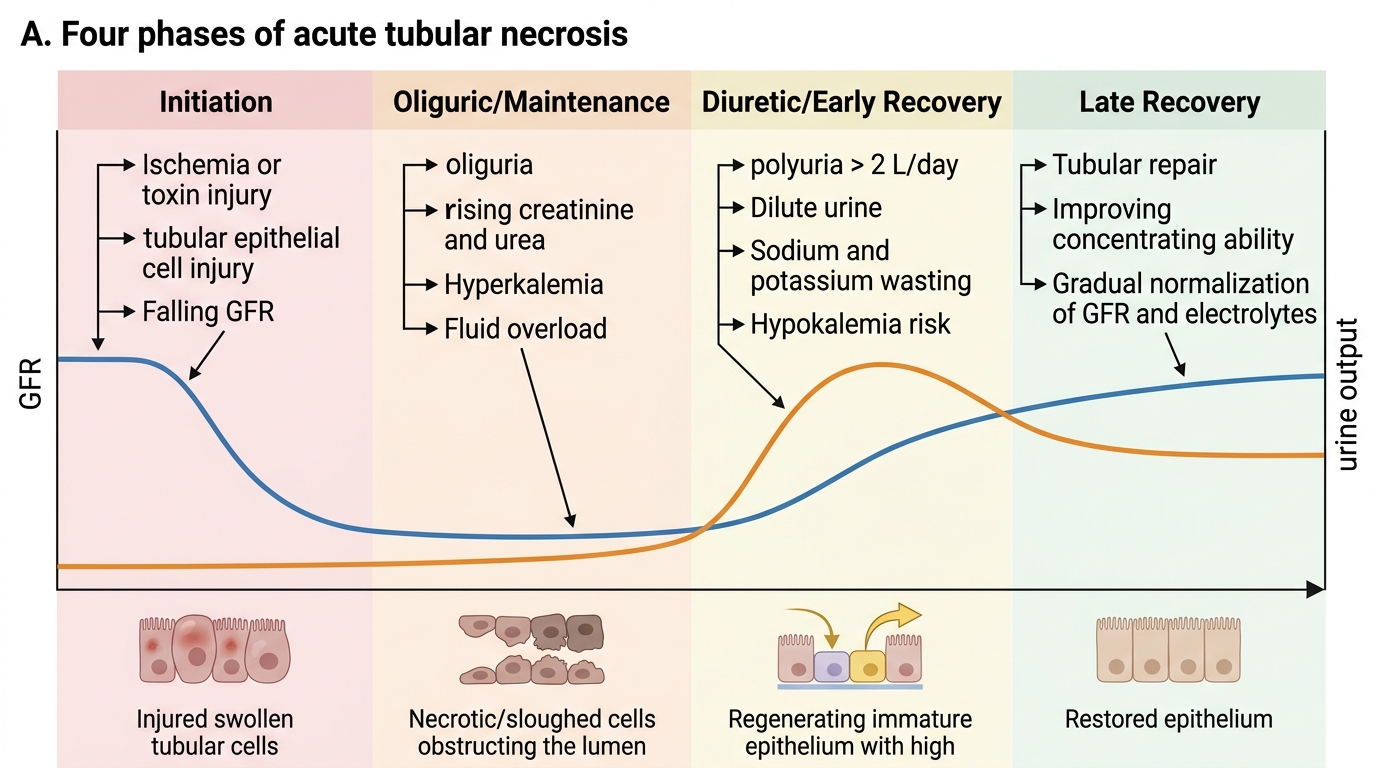
Four Phases of Acute Tubular Necrosis
SELF-CHECK
A patient recovering from ATN after septic shock is now producing 3.5 L of urine per day. His latest potassium is 2.9 mmol/L. Which phase of ATN is he in, and why is hypokalaemia occurring?
A. Oliguric phase; tubular necrosis prevents reabsorption
B. Initiation phase; ischaemia impairs Na/K-ATPase
C. Diuretic/early recovery phase; regenerating tubules cannot yet concentrate or reabsorb electrolytes
D. Late recovery phase; excessive urinary potassium loss due to aldosterone excess
Reveal Answer
Answer: C. Diuretic/early recovery phase; regenerating tubules cannot yet concentrate or reabsorb electrolytes
Polyuria (>2 L/day) with hypokalaemia defines the diuretic/early recovery phase. Regenerating tubular epithelium is functionally immature — it cannot reabsorb sodium, potassium, or water efficiently, leading to high-volume dilute urine with electrolyte wasting. This phase is often overlooked clinically; failure to replace potassium can cause dangerous arrhythmias. The paradox (improving AKI → hypokalaemia) reflects tubular immaturity, not aldosterone.
CLINICAL PEARL
The four urine indices that distinguish prerenal from intrinsic (ATN) AKI:
| Index | Prerenal | ATN |
|---|---|---|
| Urine Na | <20 mmol/L | >40 mmol/L |
| FENa | <1% | >2% |
| Urine osmolality | >500 mOsm/kg | ~300 mOsm/kg |
| Urine:plasma creatinine ratio | >40 | <20 |
Mnemonic: in ATN, the 'T' stands for Tubular damage → the tubule can no longer hold onto sodium → everything flips.
Caveat: FENa is unreliable in patients on diuretics, contrast nephropathy (early), and myoglobinuria. Use FEUrea in those settings.
Complications of AKI
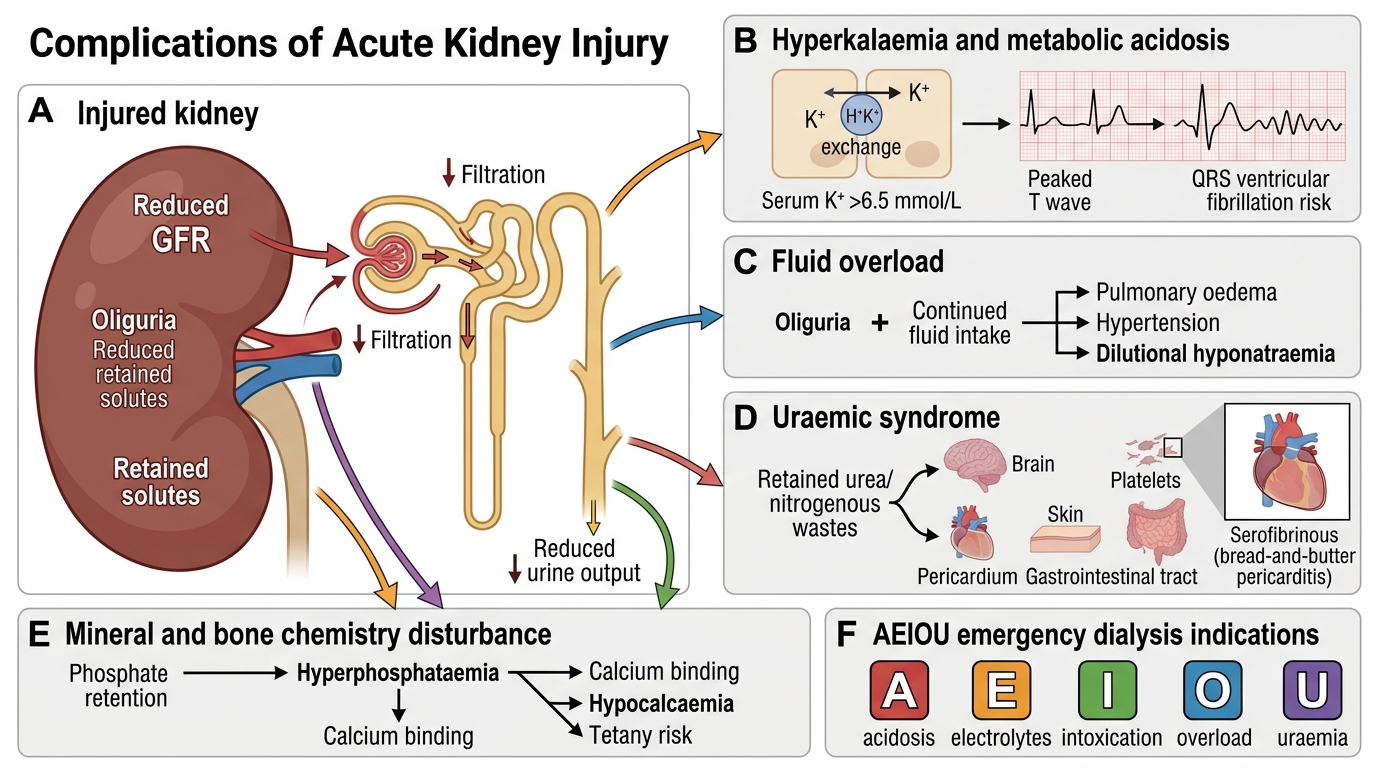
Complications of Acute Kidney Injury
The oliguric phase of AKI generates life-threatening metabolic derangements that require urgent recognition:
1. Hyperkalaemia — ↓GFR + acidosis (H⁺/K⁺ exchange pushes K⁺ out of cells). Serum K⁺ >6.5 mmol/L → cardiac arrhythmia risk (peaked T waves → widened QRS → VF). Indication for emergency dialysis.
2. Metabolic acidosis — kidneys cannot excrete H⁺ or regenerate HCO₃⁻. High anion-gap metabolic acidosis (phosphates, sulphates accumulate). Worsens hyperkalaemia and myocardial function.
3. Fluid overload — oliguria + continued fluid intake → pulmonary oedema, hypertension, hyponatraemia (dilutional).
4. Uraemic syndrome — accumulation of urea and other nitrogenous waste products: nausea, vomiting, encephalopathy, asterixis, pericarditis (serofibrinous; 'bread-and-butter' appearance), bleeding tendency (platelet dysfunction), pruritus.
5. Anaemia — shortened red-cell survival + ↓EPO production (early in AKI, prominent in CKD).
6. Hyperphosphataemia and hypocalcaemia — impaired phosphate excretion → ↑PO₄³⁻ → complexes Ca²⁺ → ↓iCa²⁺ → tetany risk.
Remember the acronym AEIOU for dialysis indications in AKI: Acidosis (pH <7.1), Electrolytes (refractory hyperkalaemia), Intoxication (dialysable toxins), Overload (pulmonary oedema refractory to diuretics), Uraemia (encephalopathy/pericarditis/bleeding).
Chronic Kidney Disease — Definition, Causes, and Staging
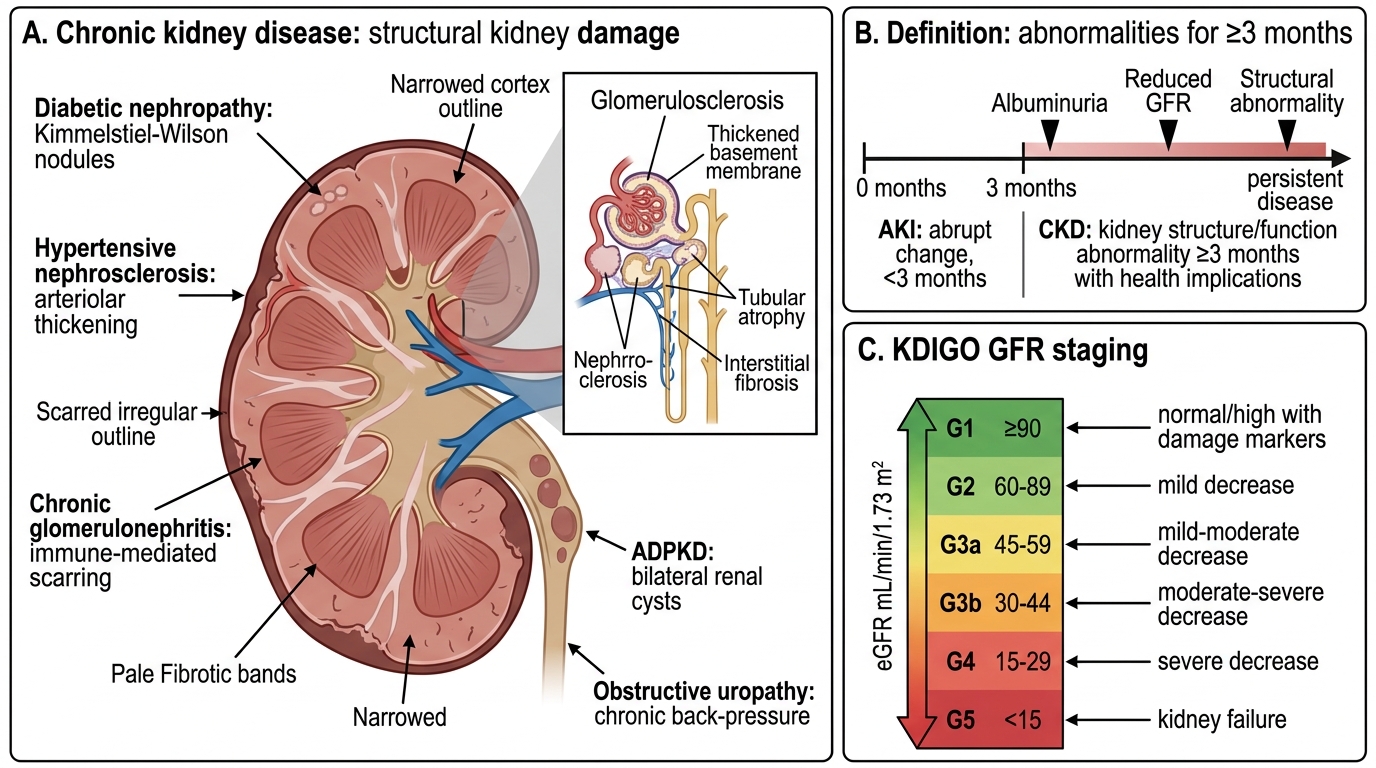
Chronic Kidney Disease: Definition, Causes, and GFR Staging
Chronic kidney disease (CKD) is defined by KDIGO as: abnormalities of kidney structure or function (or both) present for ≥3 months with implications for health. This 3-month threshold distinguishes CKD from AKI.
Five major causes (MBBS examination staples):
1. Diabetic nephropathy — global #1 cause (~35–40% in developed nations; ~30% in India). Kimmelstiel-Wilson nodules, diffuse glomerulosclerosis.
2. Hypertensive nephrosclerosis — arteriolar and arterial disease → ischaemic glomerulosclerosis.
3. Chronic glomerulonephritis — post-streptococcal GN, IgA nephropathy, FSGS, membranous nephropathy (late).
4. Polycystic kidney disease (PKD) — autosomal dominant (ADPKD, PKD1/PKD2 mutations); bilateral cysts replace parenchyma.
5. Obstructive uropathy — posterior urethral valves (children), BPH, recurrent stones → chronic back-pressure damage.
KDIGO GFR staging:
| Stage | GFR (mL/min/1.73 m²) | Description |
|---|---|---|
| G1 | ≥90 | Normal/high GFR with kidney damage markers |
| G2 | 60–89 | Mildly decreased |
| G3a | 45–59 | Mild-moderately decreased |
| G3b | 30–44 | Moderate-severely decreased |
| G4 | 15–29 | Severely decreased |
| G5 | <15 | Kidney failure (renal replacement therapy) |
Albuminuria category (A1/A2/A3) is overlaid on the GFR stage to risk-stratify — a G3a patient with heavy proteinuria (A3) progresses faster than one without.
SELF-CHECK
A 52-year-old woman with type 2 diabetes for 15 years has a GFR of 38 mL/min/1.73 m² and urine albumin-to-creatinine ratio of 350 mg/g (A3). What is her CKD GFR stage, and what structural finding would you expect on renal biopsy?
A. G2; minimal change disease
B. G3b; diffuse glomerulosclerosis and Kimmelstiel-Wilson nodular deposits
C. G4; acute tubular necrosis
D. G5; end-stage kidney with cortical thinning only
Reveal Answer
Answer: B. G3b; diffuse glomerulosclerosis and Kimmelstiel-Wilson nodular deposits
GFR 30–44 = Stage G3b. In diabetic nephropathy (the #1 cause of CKD globally), biopsy shows diffuse mesangial expansion (diffuse glomerulosclerosis) and, classically, Kimmelstiel-Wilson nodules (nodular glomerulosclerosis) — acellular PAS-positive deposits in the peripheral mesangium. Tubular atrophy and interstitial fibrosis are also present at this stage. This patient's heavy albuminuria (A3) places her in the highest progression-risk category.