Page 7 of 25
PA27.5-6 | Glomerular Diseases — SDL Guide (Part 2)
Focal Segmental Glomerulosclerosis (FSGS)
Focal Segmental Glomerulosclerosis: Pathology and Clinical Course
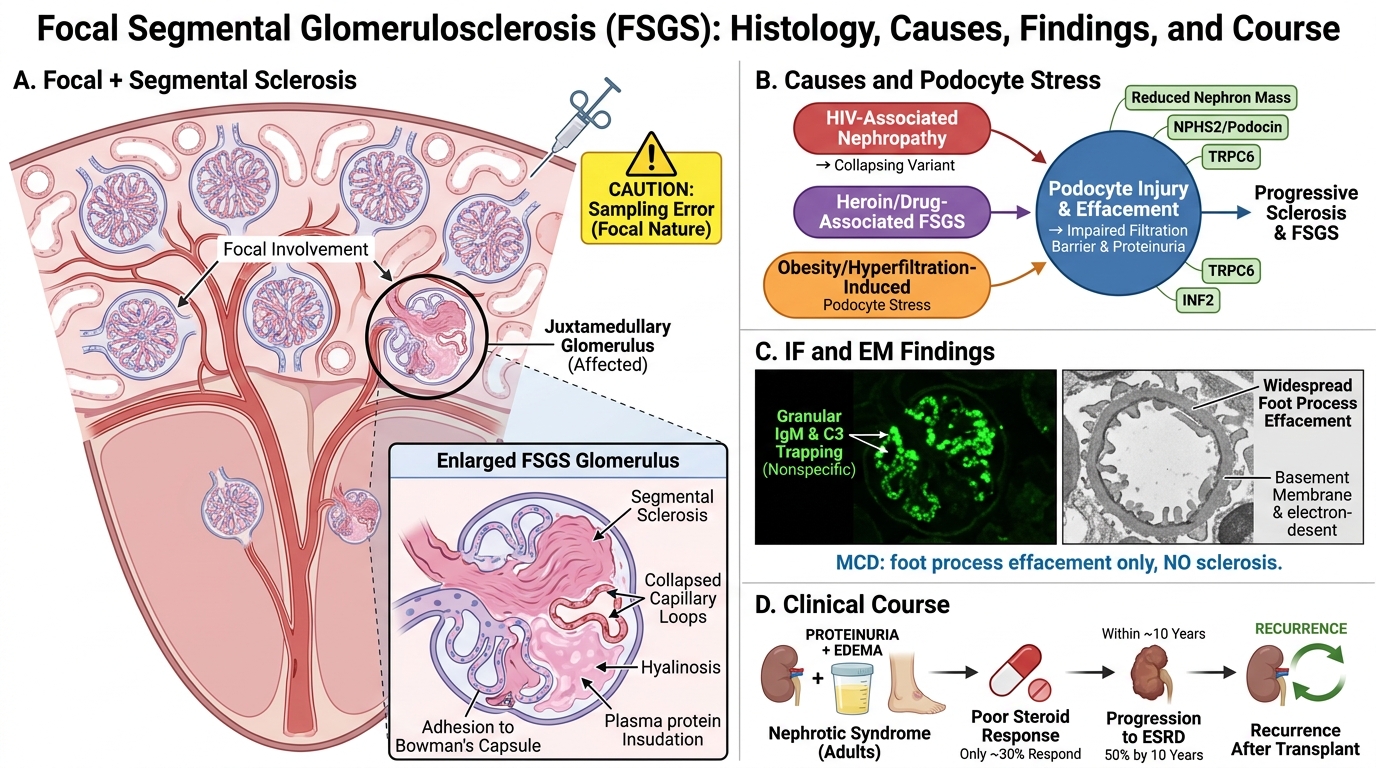
Focal segmental glomerulosclerosis means sclerosis (scarring/collapse) affecting some glomeruli (focal = < all) and only part of each affected glomerulus (segmental = < whole tuft). It is the most common cause of nephrotic syndrome in adults in many series.
Causes — remember the triad: HIV, heroin (or other drugs), obesity
• Primary (idiopathic): Circulating permeability factors; suPAR implicated
• HIV-associated nephropathy (HIVAN): collapsing variant; severe course
• Heroin nephropathy: now rare; similar histology to idiopathic FSGS
• Obesity-related: Hyperfiltration-induced podocyte stress (maladaptive FSGS)
• Secondary to reduction in nephron mass: post-unilateral nephrectomy, reflux nephropathy
• Genetic: mutations in NPHS2 (podocin), TRPC6, INF2
Pathology:
• LM: Focal and segmental areas of glomerular sclerosis — hyalinosis (insudation of plasma proteins), collapse of capillary loops, adhesion to Bowman's capsule. The JUXTAMEDULLARY glomeruli are affected first (sampling error on biopsy is real).
• IF: Non-specific IgM and C3 in sclerotic segments (entrapped, not deposited immunologically).
• EM: Foot process effacement in sclerotic AND non-sclerotic segments — this is the key difference from MCD where only the foot processes are abnormal.
Clinical course: Poor. Only 30% respond to steroids. ~50% progress to ESRD within 10 years. Recurs in transplanted kidneys (especially if circulating permeability factor is the cause), making FSGS one of the most feared diagnoses in nephrology.
Membranous Nephropathy
Membranous Nephropathy: Pathology and Clinical Correlates
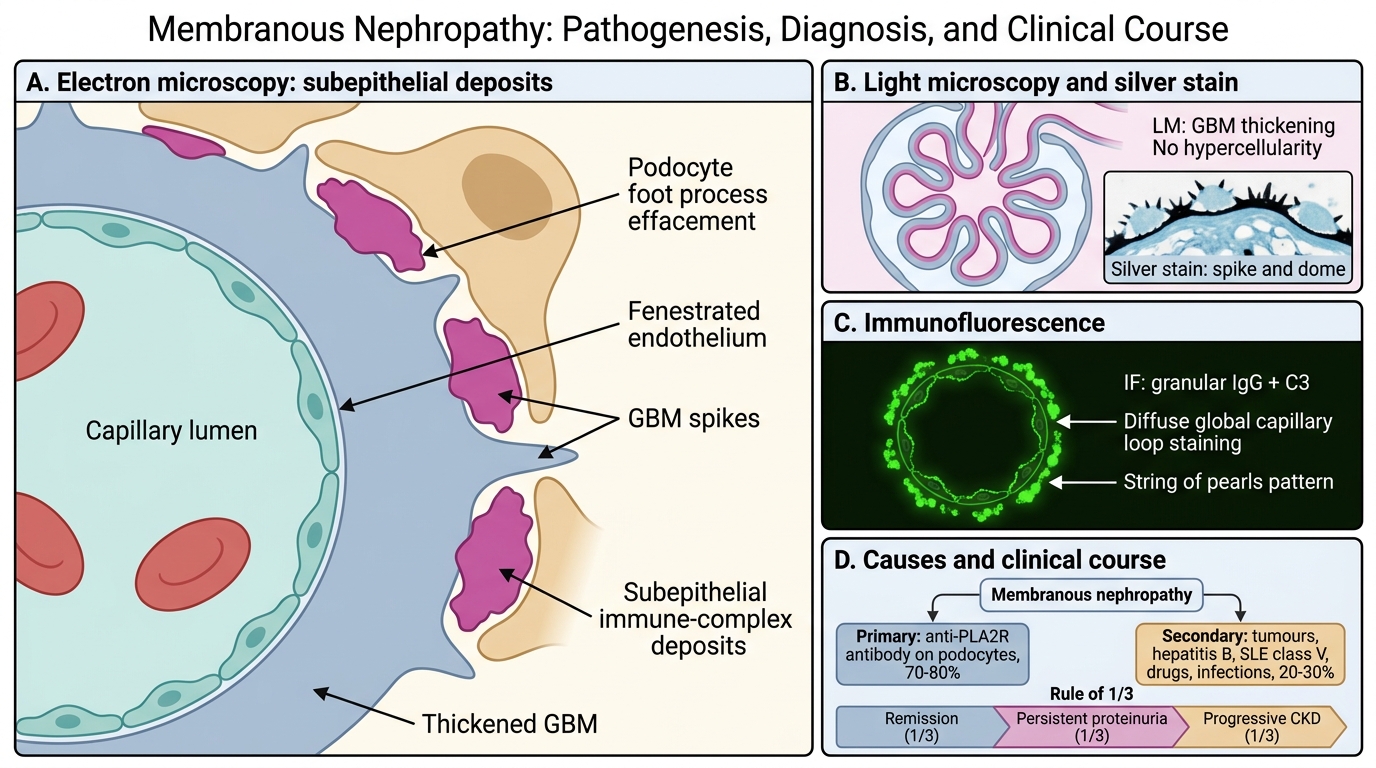
Membranous nephropathy is the commonest cause of primary nephrotic syndrome in adults (especially 30-60 years). It is defined by subepithelial immune-complex deposits that thicken the GBM.
Primary (70-80%): Autoantibody against phospholipase A2 receptor (PLA2R) on podocytes. PLA2R antibody titre correlates with disease activity and is now used clinically to monitor response.
Secondary (20-30%): Solid tumours (lung, colon — paraneoplastic), hepatitis B, SLE (lupus membranous = Class V), drugs (gold, penicillamine, NSAIDs), infections.
Rule of 1/3: ~1/3 spontaneous complete remission, ~1/3 persistent proteinuria without progression, ~1/3 progressive CKD.
Pathology:
• LM: GBM thickening without hypercellularity (this is important — no proliferation, no inflammation). Silver methenamine stain shows a characteristic 'spike and dome' pattern — the 'spikes' are projections of GBM matrix growing up between the subepithelial deposits ('domes').
• IF: Granular IgG (and C3) deposits in a diffuse, global, subepithelial distribution — like a string of pearls along the capillary loop.
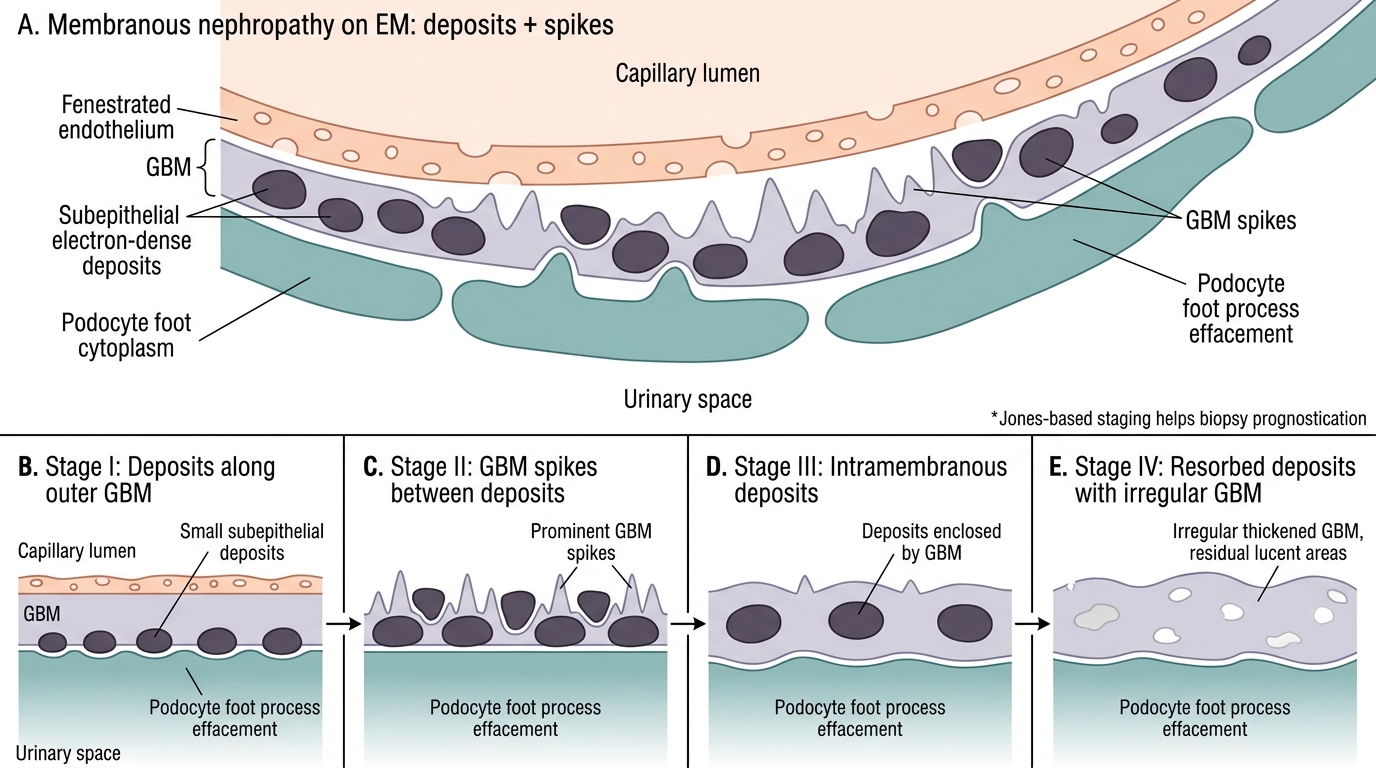
• EM: Subepithelial electron-dense deposits separated by GBM spikes. In advanced disease, deposits are incorporated into the GBM (intramembranous stage) and eventually resorb, leaving lucent holes in the GBM (post-deposit stage).
Membranous Nephropathy: EM Features and Jones Stages
Stages (Jones-based staging): Stage I (subepithelial deposits, no spikes) → Stage II (spikes present) → Stage III (deposits surrounded, intramembranous) → Stage IV (resorption, irregular GBM) — useful for prognostication on biopsy reports.
Membranoproliferative GN (MPGN)
Membranoproliferative Glomerulonephritis: Overlap Pattern and Classification
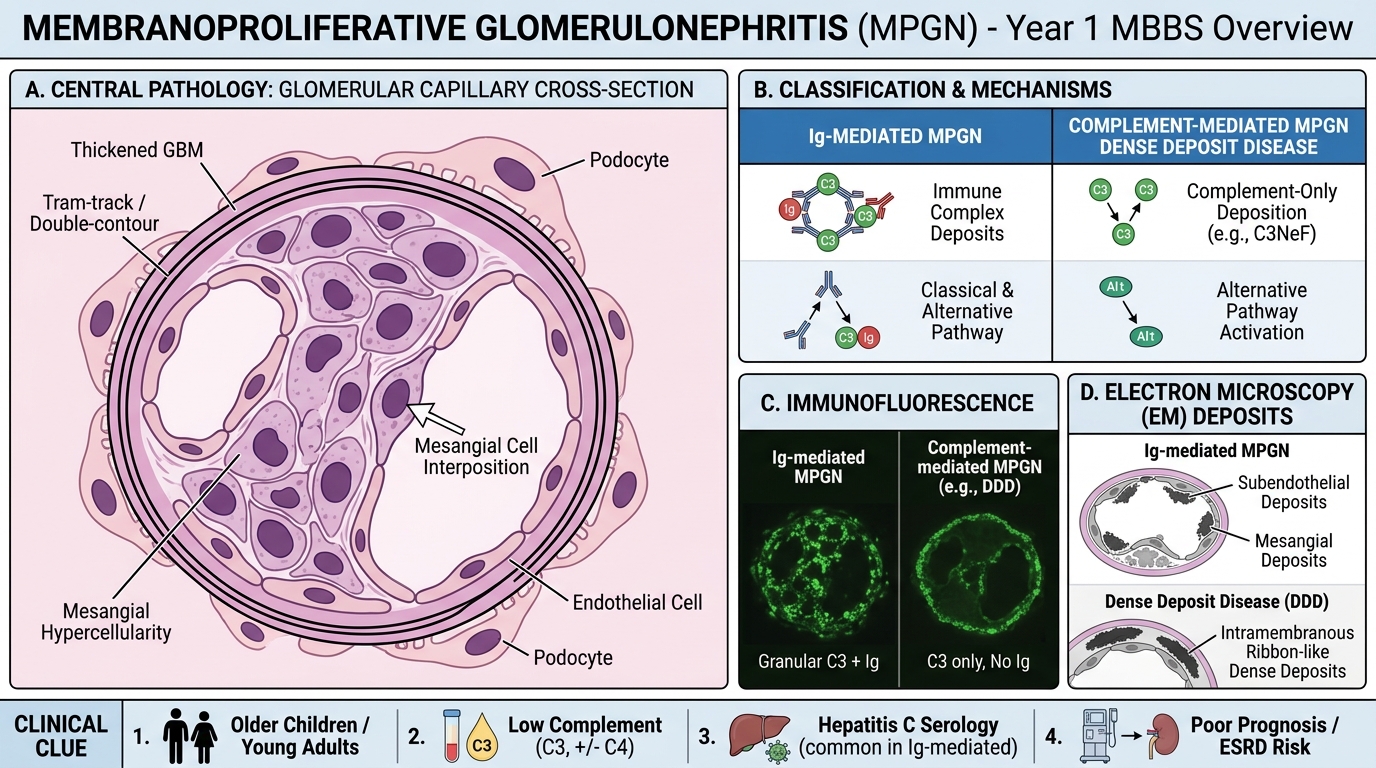
Membranoproliferative glomerulonephritis combines features of both nephrotic and nephritic syndrome — it is the great 'overlap' disease.
Classification (modern immune-based):
• Ig-mediated MPGN (former Type I): Immune-complex deposition in mesangium and subendothelium; causes = hepatitis C (most common), cryoglobulinaemia, SLE. C3 + C4 both low (classical pathway activation).
• Complement-mediated MPGN (former Type II / Dense Deposit Disease): Uncontrolled alternative pathway due to C3 nephritic factor (C3NeF, autoantibody stabilising C3 convertase) or factor H deficiency. Only C3 low (alternative pathway). IF: C3 only, no Ig.
Pathology:
• LM: Mesangial hypercellularity + GBM thickening + 'tram-track' or double-contour GBM (PAS/silver stain). The double contour is created by mesangial cell interposition between the endothelium and the GBM — the mesangium literally grows into the capillary wall.
• IF: Granular C3 ± Ig along capillary walls (pattern depends on type).
• EM: Subendothelial + mesangial deposits (Ig-mediated); intramembranous ribbon-like dense deposits (Dense Deposit Disease).
Clinical: Presents in older children and young adults. Low complement is the clue. Hepatitis C serology essential. Poor prognosis; ~50% reach ESRD in 10 years.
SELF-CHECK
A 4-year-old with nephrotic syndrome has a biopsy showing normal glomeruli on LM, negative IF, and diffuse foot process effacement on EM. Which finding on urinalysis is most expected?
A. Red cell casts in urine
B. Oval fat bodies with Maltese-cross birefringence under polarised light
C. White cell casts indicating tubular infection
D. Granular casts indicating tubular necrosis
Reveal Answer
Answer: B. Oval fat bodies with Maltese-cross birefringence under polarised light
This is minimal change disease (MCD). The massive proteinuria (> 3.5 g/day) leads to urinary loss of lipoproteins, which appear as oval fat bodies and Maltese-cross birefringence under polarised light — classic findings of nephrotic syndrome. Red cell casts are a nephritic, not nephrotic, feature. MCD is characterised by selective proteinuria without haematuria.